

Abstract
Bochdalek hernia occurs from a congenital defect of the diaphragm, allowing the passage of abdominal structures into the thoracic cavity, limiting lung expansion and ventilatory function. Bochdalek hernia is common in neonates but rarely occur in adults; there are only 4 documented cases in the elderly population. We present a case of an 88-year-old woman with severe hypoxia and respiratory failure that required ventilatory support, in whom bilateral Bochdalek hernias progressed over the years and severely invaded the thoracic cavity, causing acute decompensation. This is a rare condition in adults but can cause substantial morbidity when the involvement of the thoracic cavity is severe.
Introduction
Bochdalek hernia is caused by a posterolateral defect of the diaphragm due to the failure of the pleuroperitoneal folds to fully mature. This anomaly was first described in 1848, although it may have been discovered as early as the 17th century.1,2 This type of hernia allows the passage of gastrointestinal structures into the thoracic cavity, which limits lung expansion, functional capacity, and ventilatory performance. Bochdalek hernia is common in neonates and rare in adults, especially in the elderly.3 We present a case of an 88-year-old woman admitted to our hospital with hypoxia and respiratory failure that required ventilatory support, and who was found to have bilateral Bochdalek hernias severely invading the thoracic cavity.
Case Report
An 88-year-old woman with a medical history of kyphoscoliosis, stage 3 chronic kidney disease, hiatal hernia, COPD (for which she was on home oxygen), and diastolic heart failure presented to the emergency department with a 3-day history of progressive shortness of breath and increased oxygen requirement, from 2 L/min to 6 L/min. She also reported poor appetite for the last week. She presented with generalized weakness, described as lack of energy all over her body with worsening fatigue, asthenia, and adynamia. There were no other associated symptoms such as chest pain, fever, chills, cough, edema, or upper-respiratory symptoms. Prior to admission she was adherent to her medications, which included furosemide and potassium supplements. Pulmonary function tests (PFTs) performed about 6 months before this admission revealed a mixed restrictive and obstructive pattern: FEV1 60% of predicted, forced vital capacity (FVC) 70% of predicted, FEV1/FVC 65% of predicted, total lung capacity 90% of predicted, residual volume 115% of predicted, and diffusing capacity of the lung for carbon monoxide 60% of predicted.
On examination she was hemodynamically stable, afebrile, and hypoxemic, with SpO2 of 73% on room air, which increased to 93% on supplemental oxygen at 4 L/min via nasal cannula. She had signs of moderate respiratory distress and was diaphoretic, tachypneic, and she had labored breathing, with use of the accessory respiratory muscles, and spoke in short sentences. Auscultation revealed bilateral crackles. There was bilateral pitting edema on the lower extremities. Laboratory tests, including the serum metabolic assay 7 (SMA 7), hepatic panel, and complete blood count were normal. Brain natriuretic peptide was 787 mg/dL. Troponin, brain-type and muscle-type creatine kinase, cardiac index, and D-dimer were negative. Electrocardiogram demonstrated sinus rhythm at 72 beats/min, without abnormalities.
Chest radiograph showed opacification of the mid-left and lower left lung fields, with prominent interstitial vessels and bilateral pleural effusions (Figure 1). Non-contrast computed tomography revealed features suggestive of congestive cardiac failure, with interlobular interstitial markings in the upper lobes, ground-glass opacities, small bilateral pleural effusions, air bronchograms, and possible underlying atelectasis in the left lower lobe, with large bilateral Bochdalek hernias containing fat and small-bowel loops (Figure 2). The hernias were approximately 28 cm in the left hemithorax and 24.5 cm on the right. No consolidations were observed.

Chest radiograph shows prominent interstitial vessels consistent with pulmonary edema, bilateral opacification of the lower lobes, and blunting of the costodiaphragmatic angles.
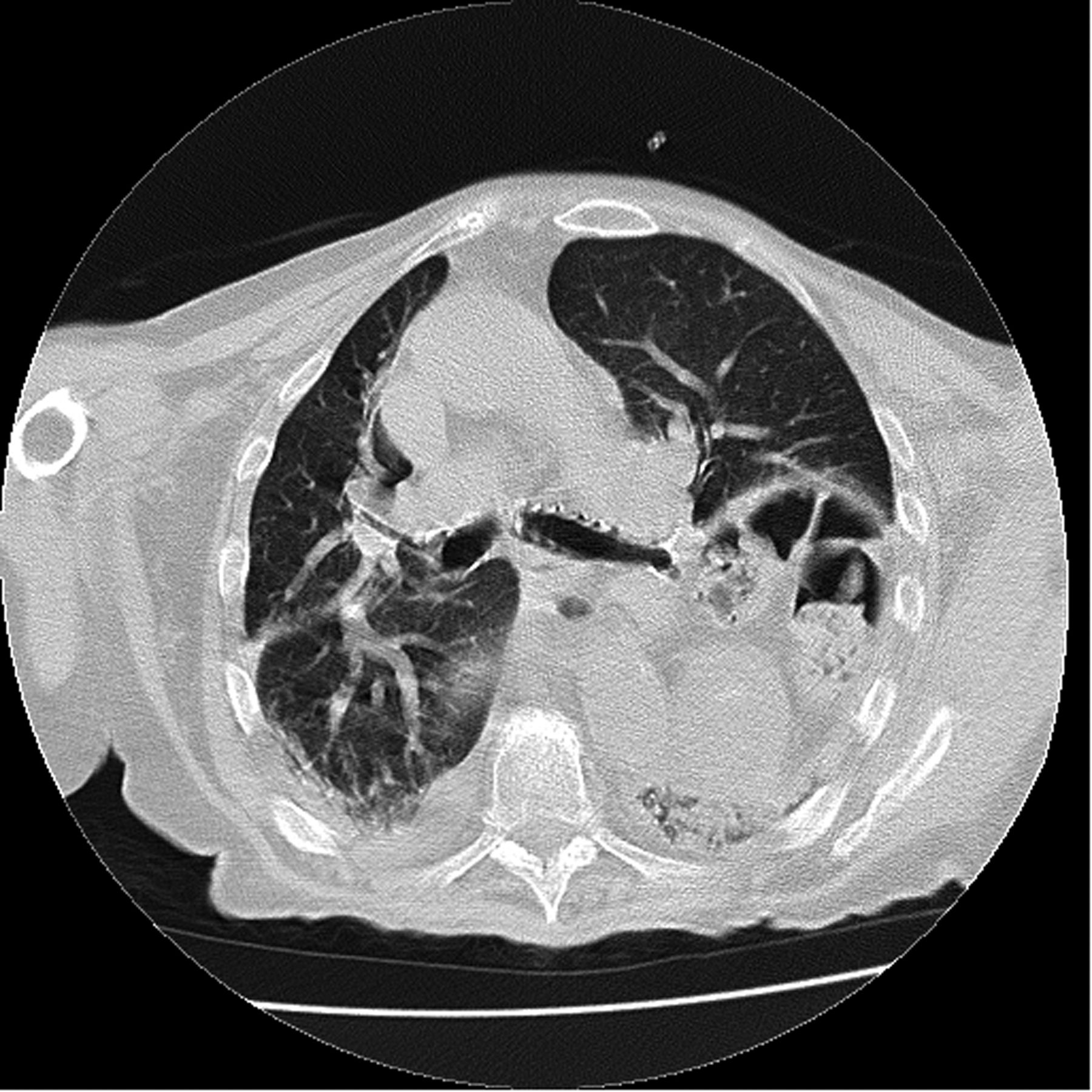
Computed tomogram shows intestinal loops (containing feces) within the thoracic cavity, up to the level of the carina on the left side.
A stress echocardiogram showed an ejection fraction of 60% in the right ventricle, hypokinesia, an abnormal left-ventricular relaxation, and pulmonary artery systolic pressure of 45 mm Hg, and no evidence of ischemia. On her previous 2-dimensional echocardiogram she had mild to moderate right-ventricular hypokinesis, ejection fraction of 55%, and pulmonary hypertension.
On the third hospital day she was found lethargic, with SpO2 of 88% on supplemental oxygen at 4 L/min via nasal cannula. Immediately, she was placed on bi-level positive airway pressure with an FIO2 of 0.60, inspiratory support of 14 cm H2O, and expiratory support of 5 cm H2O. Her initial arterial blood analysis showed severe respiratory acidosis: pH 7.11, PaCO2 134 mm Hg, HCO3 41.7 mEq/L, and PaO2 99 mm Hg.
She was admitted to the intensive care unit for close monitoring and impending respiratory failure, and treated with noninvasive ventilation (NIV). Her respiratory status, including CO2 retention, improved dramatically with NIV and she was transferred back to the medical floor. Cardiothoracic surgery was consulted for surgical repair of the diaphragmatic defects, but she refused surgery. She was discharged to a skilled nursing facility for rehabilitation on continuous oxygen at 5 L/min via nasal cannula. She went home on nasal cannula only, due to insurance issues and her reluctance to stay until NIV approval. However, NIV was started soon after discharge.
At one-week follow-up after discharge she was on NIV and reported adherence to therapy. The sniff test, vital capacity, and negative inspiratory force tests were not done at discharge, but they were scheduled to be done soon. Also, since surgery was no longer an option, we opted for an aggressive medical regimen. She was given an inhaler for intermittent use, and an incentive spirometer, and was scheduled for frequent follow-ups in the clinic. Since there is no standard medical approach Bochdalek hernia, we used supportive measurements to control her symptoms. Consequently, she was referred to a pulmonary rehabilitation program, but she refused to be enrolled.
Discussion
Bochdalek hernia is a congenital defect that arises from the posterolateral wall of the diaphragm when the pleuroperitoneal folds fail to close, leaving a persistent foramen that allows intestinal loops to enter the thorax. Only 15% of Bochdalek hernias present in the peritoneal sac, and in 90% of cases it occurs on the left side, because the fusion of the pleuroperitoneal folds occurs earlier in the embryonic life on the right.4 The liver also provides some protection on the right, hindering the entry of the intestines into the thorax.
Bochdalek hernia was first described in 1848 by Vincent Alexander Bochdalek, a Czech anatomist, and it has been classically described in neonates, with some reports of occurrence in early adulthood and rare occurrence in the elderly.5 The estimated incidence in adults is around 6% according to early series,6 and its usual presentation includes abdominal symptoms such as vague discomfort, nausea, and vomiting, caused mostly by the retroperitoneal fat that invades the thoracic cavity and limits peristalsis and gastrointestinal mobility. Other reports have suggested that the actual incidence might be much lower, as seen in a study by Mullins et al, in which they evaluated 13,138 computed tomograms from patients 29–91 years old. Bochdalek hernia occurred in 0.17% of that population, and most of the hernias were small to moderate size. Fourteen percent were bilateral, which corresponded to 0.02% of the total population in that study.7
In adults the majority of Bochdalek hernias are found incidentally as they are usually small and asymptomatic.2,6,8–11 In the rare cases in which symptoms do occur, especially in adults, a triggering event is usually present, such as trauma, exercise, sexual intercourse, anxiety, or another factor associated with increased metabolic demand or thoracic and abdominal pressure, such as pregnancy, labor, large food ingestion, and even sneezing or coughing.1
To date only 4 cases of bilateral Bochdalek hernia in adults have been reported,12–15 and only 2 cases have been reported in octogenarians, with only one being bilateral. Our patient highlights Bochdalek hernia as an unusual cause of respiratory failure in an octogenarian. Our patient was unusual in that this congenital defect persisted throughout her entire life until the current critical presentation. Typically, large Bochdalek hernias have been associated with pulmonary hypoplasia after birth, whereas small Bochdalek hernias allow normal lung development and are asymptomatic until a triggering event.3
Our patient's large bilateral Bochdalek hernias contributed to acute decompensation of her respiratory function. We believe her hernia progressed over the years, as she was diagnosed more than 10 years previously, and the intestine reached a high thoracic level (Fig. 3). Moreover, her baseline cardiopulmonary function was already compromised with heart failure, severe kyphoscoliosis, and a mixed obstructive/restrictive pulmonary disorder, on the basis of diagnosis of moderate COPD according to the Global Initiative for Chronic Obstructive Lung Disease guidelines (FEV1/FVC < 70, FEV1 50–80% of predicted), which limited her ventilatory function and gas exchange. Her PFTs revealed a mixed obstructive and restrictive disorder, with an obstructive pattern from her COPD, but without air trapping or hyperinflation, as evidenced by a low total lung capacity and residual volume, probably secondary to a restrictive disorder from the hernia compressing the lungs. Also, the mild decrease in the diffusing capacity of the lung for carbon monoxide can be explained by the pulmonary hypertension and probably by the emphysema from the moderate COPD, which could explain the dyspnea.

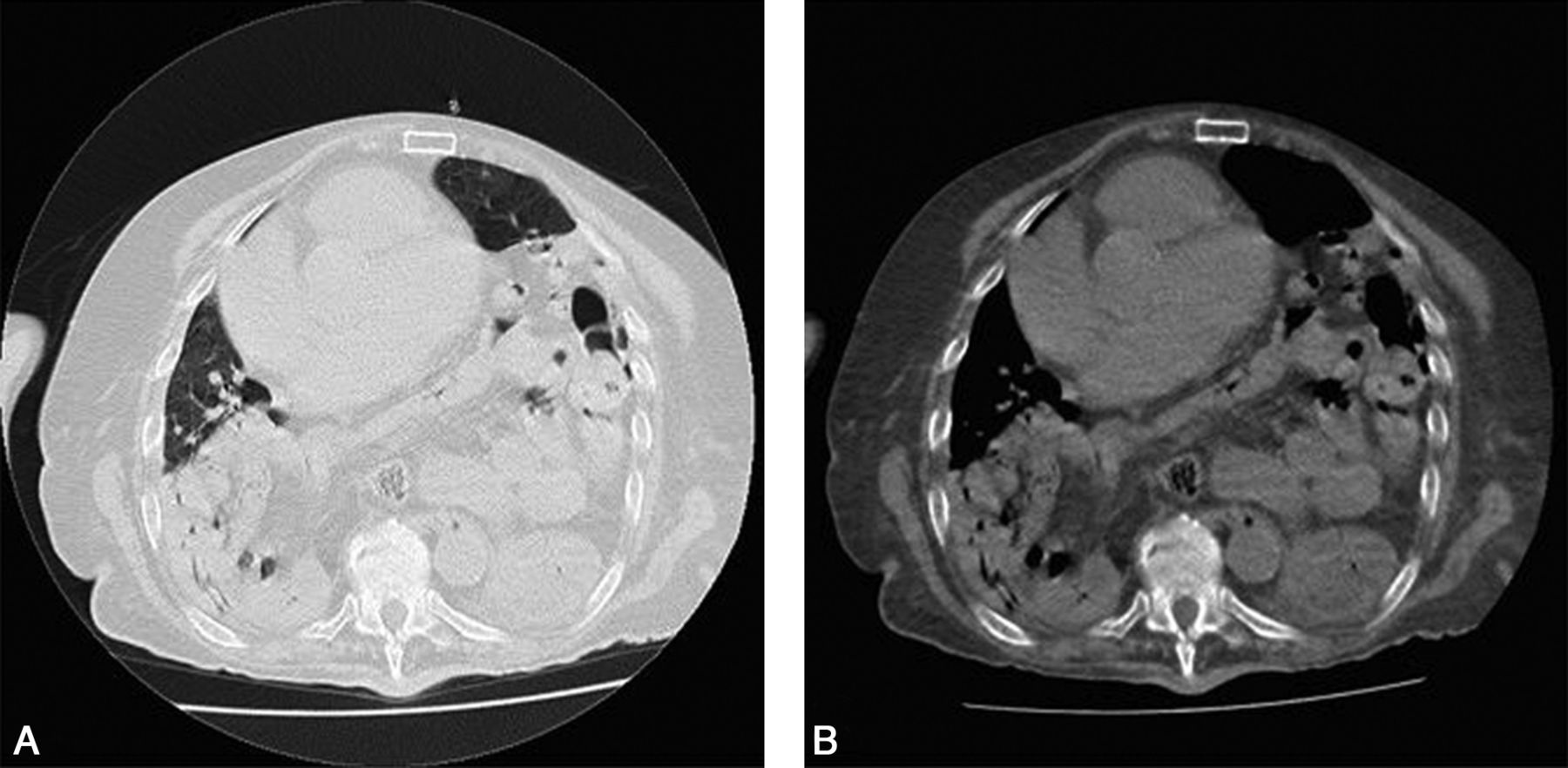
Computed tomogram shows bilateral intestinal invasion of the pulmonary cavities, both at the lung slice (A) and the mediastinal slice (B).
However, in our patient the triggering event that finally led to her acute clinical picture was not established. She was slowly deteriorating over the years, due to poor follow-up. She had been suffering from chronic respiratory failure, associated with longer periods of physical inactivity with the progression of muscle wasting, leading to a quicker decline of her pulmonary function, until even minor effort made her dyspneic. Differential diagnosis on admission included a possibility of pulmonary embolism, COPD exacerbation, pneumonia, and atelectasis, but those were ruled out appropriately during the diagnostic workup. On the other hand, she was on long-term oxygen therapy at home for persistent hypoxia, according to her primary care physician. Moreover, she was on albuterol inhaler as needed, but she said that she used it only when she felt some wheezing, which was an uncommon scenario for her. This raises the question of whether she did have COPD, which is confirmed by the mixed disorder pattern in the PFTs. Therefore, it is likely that she had a mixed disorder with a history of COPD, based on her history of smoking and low PaO2. Furthermore, the fact that the computed tomogram revealed no evidence of interstitial lung disease supports the theory that the restrictive component of the PFTs was probably caused by the hernias.
We believe her acute presentation was caused by a multifactorial composite of events leading to respiratory failure, most likely associated with her impaired ventilation, where the Bochdalek hernias played a key role by limiting lung expansion. The pleural effusions also limited her ventilatory capacity and increased CO2 retention. The pulmonary hypertension was probably related to her impaired baseline cardiopulmonary reserve and function. This clinical presentation, in addition to the potential risk of strangulation, which correlates with the size of the hernia, makes this condition an indication for urgent surgical intervention.16 Our patient, however, refused surgery, given the scope of her comorbidities and advanced age, and accepted only medical treatment.
In summary, Bochdalek hernias are rare in the elderly. The prognosis usually depends on the size of the hernia, the patient's comorbidities, and bilaterality. The mortality rate for surgical correction is 3–32%,17 so early intervention is key in adults, especially with bilateral Bochdalek hernias, to prevent complications and decrease morbidity and mortality.
Footnotes
- Correspondence: Carlos L Alviar MD, Department of Internal Medicine and Pulmonary Diseases, St Luke's–Roosevelt Hospital Center, Columbia University College of Physicians and Surgeons, 1111 Amsterdam Avenue, New York NY 10025. E-mail: ca2369{at}columbia.edu.
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}