

Abstract
BACKGROUND: The Boussignac continuous positive airway pressure (CPAP) device effectively treats acute pulmonary edema, but data on airway pressure with the Boussignac CPAP system are sparse.
OBJECTIVE: To evaluate the Boussignac CPAP system's ability to maintain stable inspiratory and expiratory pressure levels, and to evaluate perceived exertion during breathing with the Boussignac CPAP system.
METHODS: With 18 healthy volunteers we recorded airway pressure and air flow during 10-min sessions at 5.0, 7.5, and 10.0 cm H2O. The participants were blinded to the sequence of the CPAP levels. Each session was ended with 10 forced breaths. We measured perceived exertion with the Borg category ratio 10 (Borg CR10) scale.
RESULTS: When the participants breathed at 20% of vital capacity and a peak expiratory flow of 14% of FEV1, the maximum pressure difference between inspiration and expiration was 4.0 cm H2O at CPAP 10 cm H2O. The changes in airway pressure were never large enough to reduce airway pressure to below zero. During the forced breaths, the expiratory volume was 38–42% of vital capacity and peak expiratory flow was 49–56% of FEV1. As air flow increased, both the drop in inspiratory airway pressure and the increase in expiratory airway pressure increased.
CONCLUSIONS: With CPAP, pressure changes are considered to be associated with increased work of breathing. The device's pneumatic performance is adequate during normal breathing with low air flow, but during forced breathing (high air flow) it did not maintain stable airway pressure, which could increase the work of breathing and cause respiratory fatigue. Thus, the Boussignac CPAP system might be less suitable for a patient breathing at a higher frequency.
- CPAP
- continuous positive airway pressure
- noninvasive ventilation
- air flow
- airway pressure
- Borg CR10 scale
- flow resistor
Introduction
Continuous positive airway pressure (CPAP) is used to treat respiratory insufficiency due to acute cardiogenic pulmonary edema1–3 and sleep apnea,4 and to prevent or treat postoperative pulmonary complications.5–7 With CPAP, airway pressure is positive during the whole breathing cycle. Positive expiratory pressure can be achieved with a threshold resistor or a flow resistor. With a threshold resistor, the CPAP is obtained with a valve that opens and closes when the airway pressure is the same as the magnitude of the resistor.8,9 With a flow resistor, the CPAP is obtained with an opposing flow or an orifice resistor.9 With threshold resistor or flow resistor CPAP, to establish and maintain the positive pressure the equipment has to deliver an air flow that exceeds the peak air flow created by the patient, during the whole breathing cycle. If pressure changes occur, respiratory work increases, which can lead to respiratory fatigue.10,11
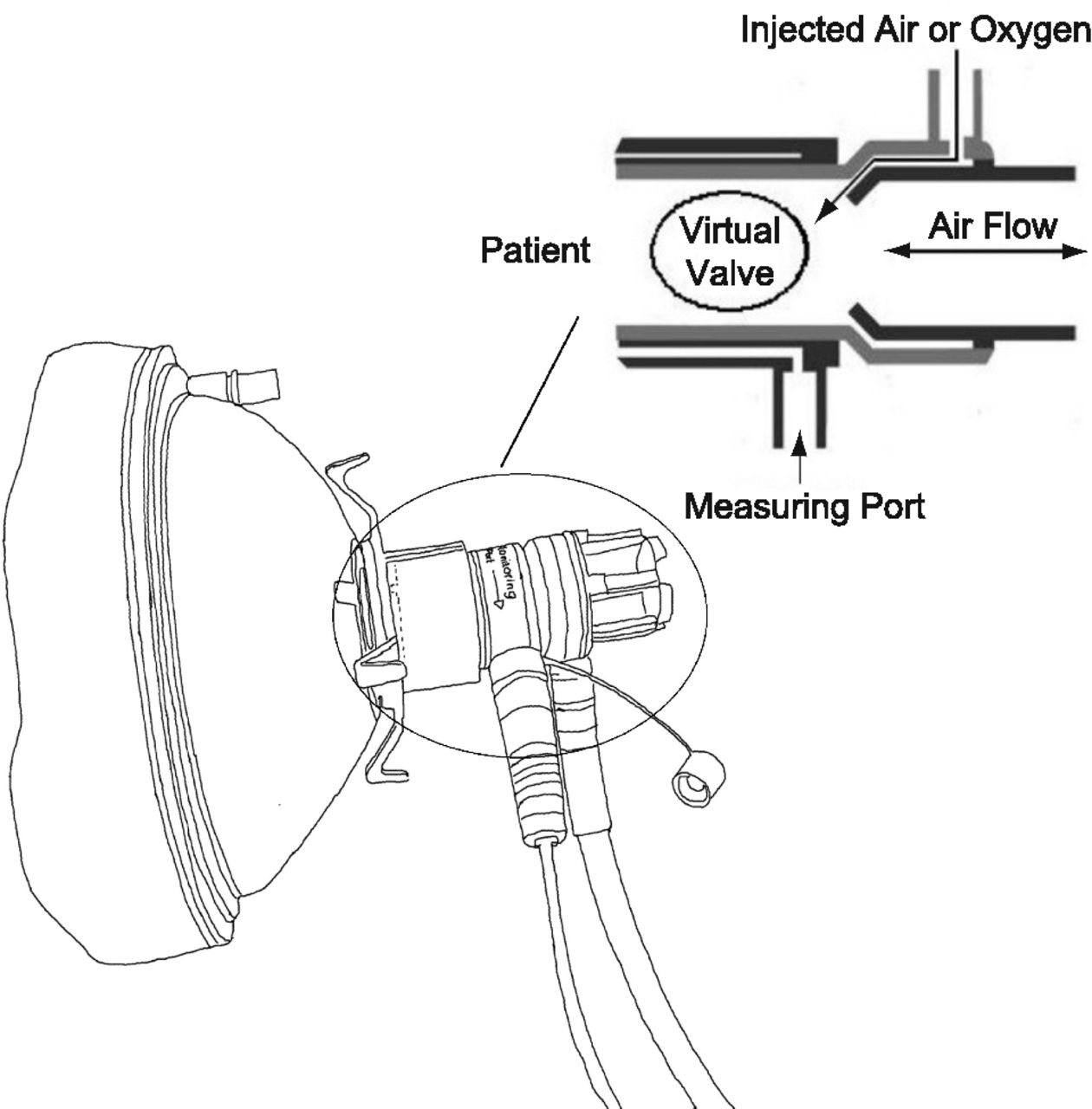
The Boussignac CPAP system (Vygon, Écouen, France) includes a plastic tube (5.5-cm long, inner diameter 13 mm) that has 4 micro-channels in the tube wall (Fig. 1). The tube is open to the atmosphere. With a flow meter, air or oxygen is injected into the micro-channels. When the delivered gas accelerates through the micro-channels, the gas molecules collide and turbulence occurs. The speed of the gas molecules is then transformed into pressure, thereby creating a virtual valve on the patient side of the tube. The speed of the gas flow through the micro-channels determines the CPAP level, which makes the pressure flow-dependent. The measurement port (see Fig. 1) allows pressure measurement or delivery of supplemental oxygen.2,3,12,13
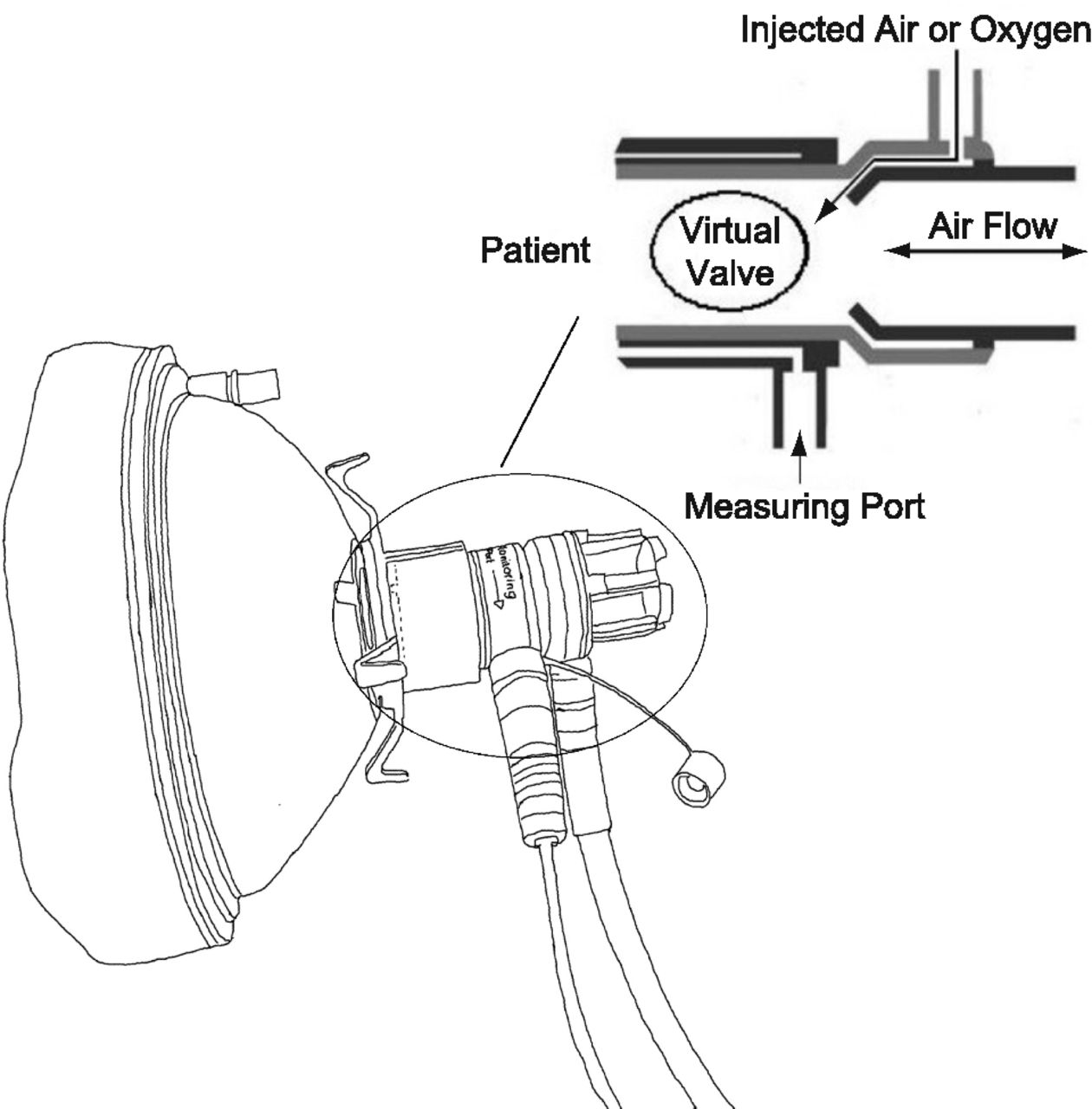
The Boussignac continuous positive airway pressure system. Air or oxygen is injected through the micro-channels in the wall of the plastic tube. As the gas molecules accelerate through the channels and enter the cylinder a virtual valve is created.
The Boussignac CPAP system is considered easy to use and it requires only a flow meter that delivers oxygen or air to create a continuous positive airway pressure.10,14,15 When oxygen is used, the amount of oxygen delivered to the patient and the CPAP level cannot be adjusted separately.16 If the measurement port is used to deliver supplementary oxygen, the possibility to monitor the CPAP level is lost.
In emergency departments and prehospital care, the Boussignac CPAP system effectively treats acute cardiogenic pulmonary edema2,3,13,17 and treats or prevents postoperative complications in obese patients.7,14 In a recent bench study, Bellani and co-workers10 evaluated the Boussignac CPAP system and observed that increased air flow was associated with enhanced airway pressure drop during inspiration. Those data indicate that the efficacy of the Boussignac CPAP system might be hampered during increased breathing efforts, which merits further investigation. We therefore studied the Boussignac CPAP system's ability to maintain stable inspiratory and expiratory pressure levels. We also evaluated perceived exertion during breathing with the Boussignac CPAP system.
Methods
This study was approved by the research ethics committee of Umeå University, and all the participants gave informed consent. We recruited 18 healthy volunteers: 13 women and 5 men, mean ± SD age 44 ± 8 years. All the participants were non-smokers and, prior to study participation, underwent spirometry (vital capacity [VC] and FEV1) (model S, Vitalograph, Buckingham, United Kingdom) to ensure they had normal lung function. We used the best of 3 measurements for both VC and FEV1.
Figure 2 shows the setup, which includes a face mask (Boussignac, Vygon, Écouen, France), a bacterial filter (BaktPlus, Codan Triplus, Kungsbacka, Sweden), a pressure transducer (PMSET 1TNF-R, Beckton Dickinson, Singapore), a flow sensor (Marquette Medical Systems, Jupiter, Florida), an air-flow transducer (SS11LA, Biopac Systems, Goleta, California), the Boussignac plastic tube (5.5-cm long, inner diameter 13 mm), and a flow meter to adjust the gas flow and thereby the CPAP level. A manometer (Vygon, Écouen, France) was connected to the monitoring port of the Boussignac plastic tube to measure the CPAP level. We measured end-tidal CO2 through a side port in the bacterial filter, and SpO2 (Marquette Medical Systems, Jupiter, Florida) via finger oximetry probe.

Experimental setup.
The participants sat on an adjustable chair in front of a table, with 90° hips and knees flexion, feet firmly on the floor, elbows on the chair armrests, and the hands on the armrests or in the lap, except during the first measurement period (at 0 cm H2O), during which the participant's hands were placed on the CPAP mask. Before the CPAP breathing tests, each participant was instructed how to use the Borg category ratio 10 (Borg CR10) perceived exertion scale,18 and to breathe as normally as possible during CPAP (ie, to think as little as possible about how they were breathing).
Figure 3 shows the study protocol. We tested 4 CPAP levels: 0 (control), 5.0, 7.5, and 10.0 cm H2O. The measurement sequence always started with 0 CPAP for 1 min, after which the participant scored his or her perceived exertion on the Borg CR10 scale.18 Then, in randomized order, the participant breathed at each CPAP level for 10 min. Each 10-min session ended with 10 forced breaths (as if running), to simulate respiratory distress, and holding the last exhalation for a couple of seconds. The participant scored his or her perceived exertion just before the 10 forced breaths.18 The participants were blinded to the order of the CPAP levels. To avoid carryover effects, the participant rested for 15 min between each CPAP level.

Study protocol. CPAP = continuous positive airway pressure.
During CPAP breathing airway pressure and air flow were continuously recorded, at 200 Hz, with data-acquisition software (Biopac Student Lab Pro 3.7.1, Biopac Systems, Goleta, California). We continuously recorded SpO2, heart rate (via pulse oximeter) and end-tidal CO2 at 0.5 Hz, with custom-made data-acquisition software (MRDView 2.4.2.6). We titrated air flow to the desired CPAP level with a manometer, and no adjustments of delivered air flow were made once the recording had started. Figure 4 shows a typical recording of airway pressure and air flow from one subject.
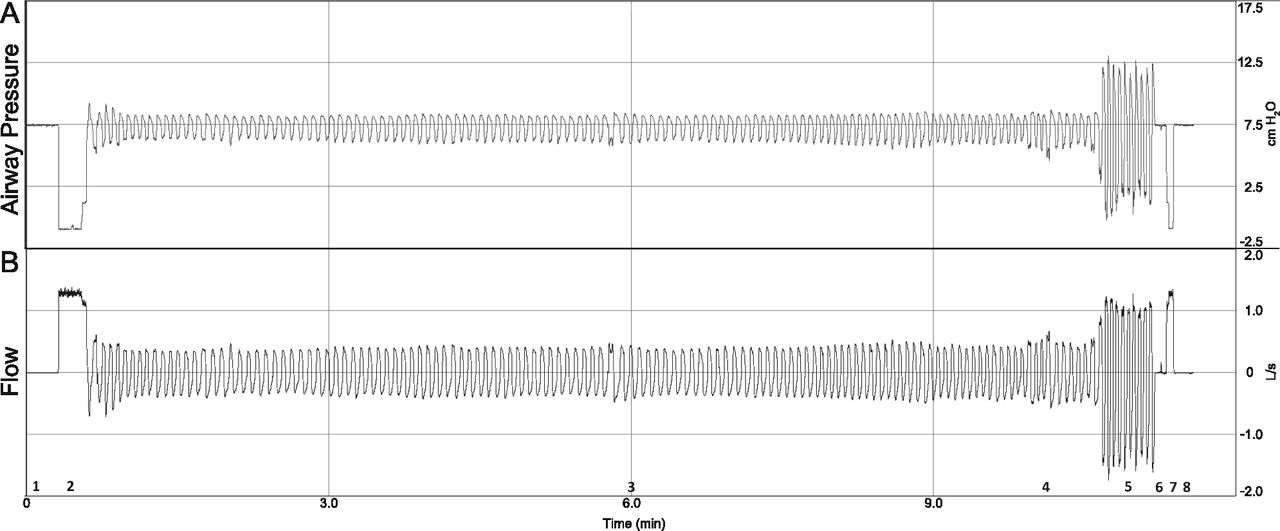
Typical wave forms of airway pressure (A) and air flow (B). After titrating the air flow to the desired continuous positive airway pressure (CPAP), the recording was started (1) and the CPAP mask was connected with a head-strap to the participant (2). After 10 min of CPAP breathing (3) the participant scored his or her perceived exertion (4), then took 10 forced breaths (5), and held the last exhalation for a couple of seconds (6). Then the mask was removed (7), and the recording was stopped (8) and the CPAP turned off.
Calibrations
We calibrated the equipment as described previously.19 Before the tests we calibrated the pressure transducer with a water column at 0 and 10 cm H2O. The air-flow transducer was calibrated with a 600-mL syringe before and after every participant. We measured the air flow and air pressure signals during a period of no air flow, and any offset in the signal was subtracted from the recorded signal during CPAP testing. The other sensors were calibrated by the manufacturer.
To eliminate high-frequency noise we filtered the recorded air flow and airway pressure signals with a numerical finite-impulse-response low-pass filter with a cutoff frequency of 10 Hz,20,21 implemented with a Hanning window with 39 coefficients.
Analysis
Analysis of the air flow and airway pressure recordings were done manually. For the 1-min recording at 0 cm H2O, we analyzed 10 breaths. For the 10-min recordings, we analyzed 10 breaths from the beginning, 10 from the middle, and 10 from the end of each 10 min period. Of the 10 forced breaths, we analyzed the first 9 breaths. The shift between inspiration and expiration was defined as the point where the air flow signal passed zero L/s (ie, when the air-flow signal changed from positive [inspiration] to negative [expiration] or vice versa). For SpO2, heart rate, and end-tidal CO2 we analyzed the last 5 sampled values from the 1-min recordings, the 10-min recordings, and the forced breathing period.
Statistical Analysis
We used repeated-measures analysis of variance to compare the CPAP levels. When the Mauchly test indicated that the assumption of sphericity had been violated, we applied the Greenhouse-Geisser correction. We used the Bonferroni correction as a post hoc test. For each CPAP level, we compared the normal-breathing data and the forced-breathing data with the paired t test. P < .05 was considered statistically significant. Data are presented as mean ± SD, except for the Borg CR10 scores, which are reported as median and range values. Data analysis was with statistics software (SPSS 18.0, SPSS, Chicago, Illinois).
Results
One of our participants interrupted the 10 cm H2O trial after a couple of minutes, due to severe respiratory fatigue, but completed the trials at the other CPAP levels. Due to a drift in the air-flow signal at 10 cm H2O, we excluded data from another participant, which reduced the number of 10 cm H2O periods to 16. Data are also missing for SpO2, heart rate, and end-tidal measurements at 0 cm H2O (control) for one subject, due to recording problems. With another subject we failed to obtain data during the forced breaths in the 5 cm H2O session. The 0 cm H2O (control) Borg CR10 score was not recorded with one participant.
Demographics
Our 18 participants were 171 ± 8 cm tall and weighed 77 ± 12 kg. Their pulmonary function was normal: VC 4.22 ± 0.97 L (92–127% of predicted), FEV1 3.40 ± 0.72 L (84–127% of predicted). SpO2 was 97–98% during all measurements. Heart rate was 70 ± 9 beats/min at CPAP of 0 cm H2O. At CPAP of 5.0, 7.5, and 10.0 cm H2O, respectively, heart rate was 75 ± 8 beats/min (P < .001), 74 ± 11 beats/min (P = .006), and 76 ± 12 beats/min (P < .001) during normal breathing, and 78 ± 9 beats/min (P < .001), 81 ± 15 beats/min (P = .001), and 82 ± 14 beats/min (P < .001) during forced breathing.
Changes in Airway Pressure
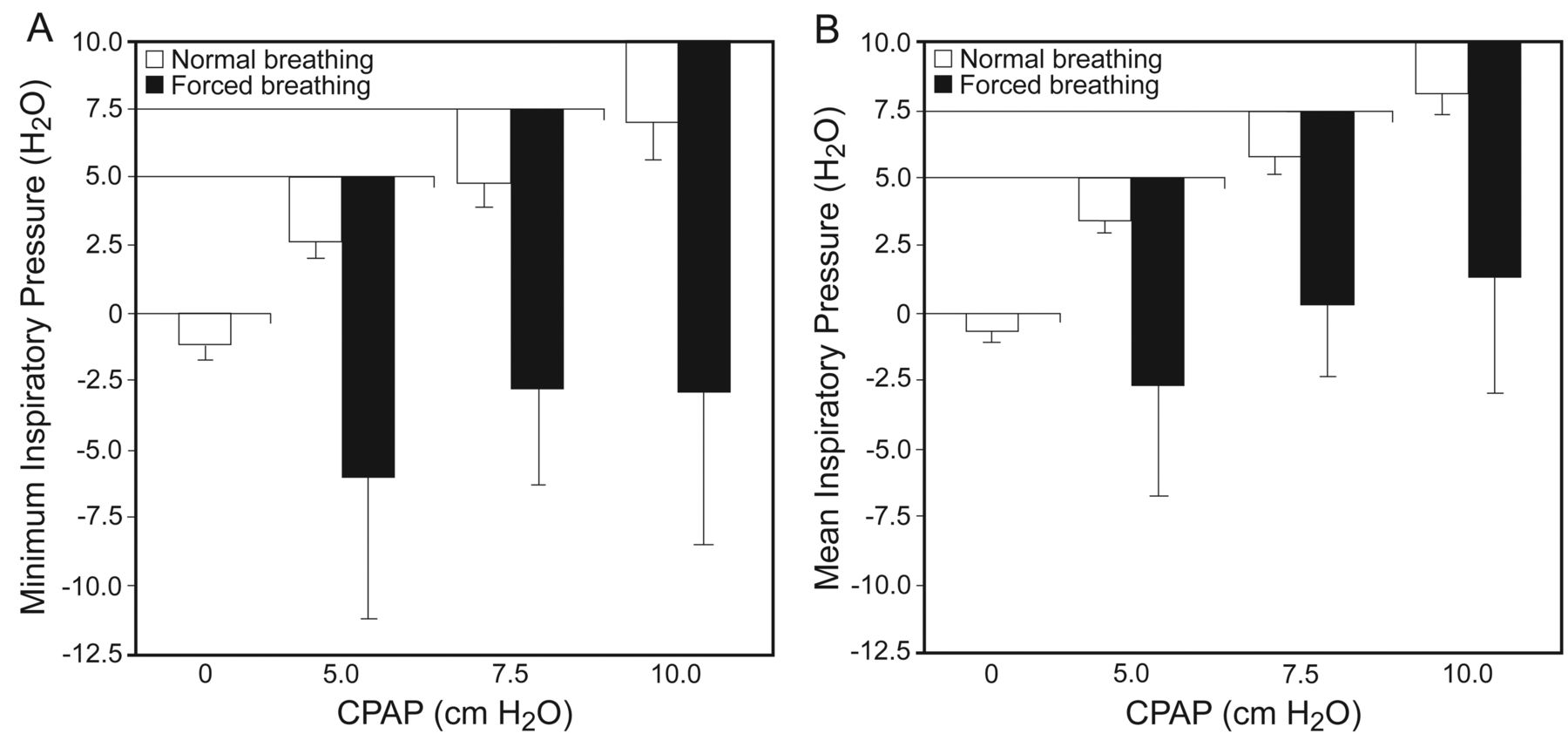
During inspiration, airway pressure decreased (Fig. 5). The pressure drop was larger at all CPAP levels, during both normal and forced breathing, than during 0 CPAP (control). During normal breathing, as the CPAP level increased, the decrease in airway pressure was enhanced. At a given CPAP level, airway pressure was lower during forced breaths than during normal breathing.

A: Minimum inspiratory airway pressure at 4 continuous positive airway pressure (CPAP) levels, during normal breathing and forced breathing. P < .001 for control versus normal breathing and forced breathing, at all CPAP levels. P = .006 for normal breathing at CPAP of 5 cm H2O versus 7.5 cm H2O. P = .006 for forced breathing at CPAP of 7.5 cm H2O versus 10 cm H2O. P < .001 for normal breathing versus forced breathing at the corresponding CPAP levels. B: Mean inspiratory airway pressure. P < .001 for control versus normal breathing and forced breathing, at all CPAP levels. P = .01 for normal breathing at CPAP of 5 cm H2O versus 7.5 cm H2O. P < .02 for forced breathing at CPAP of 7.5 cm H2O versus 10 cm H2O. P < .001 for normal breathing versus forced breathing at the corresponding CPAP levels.
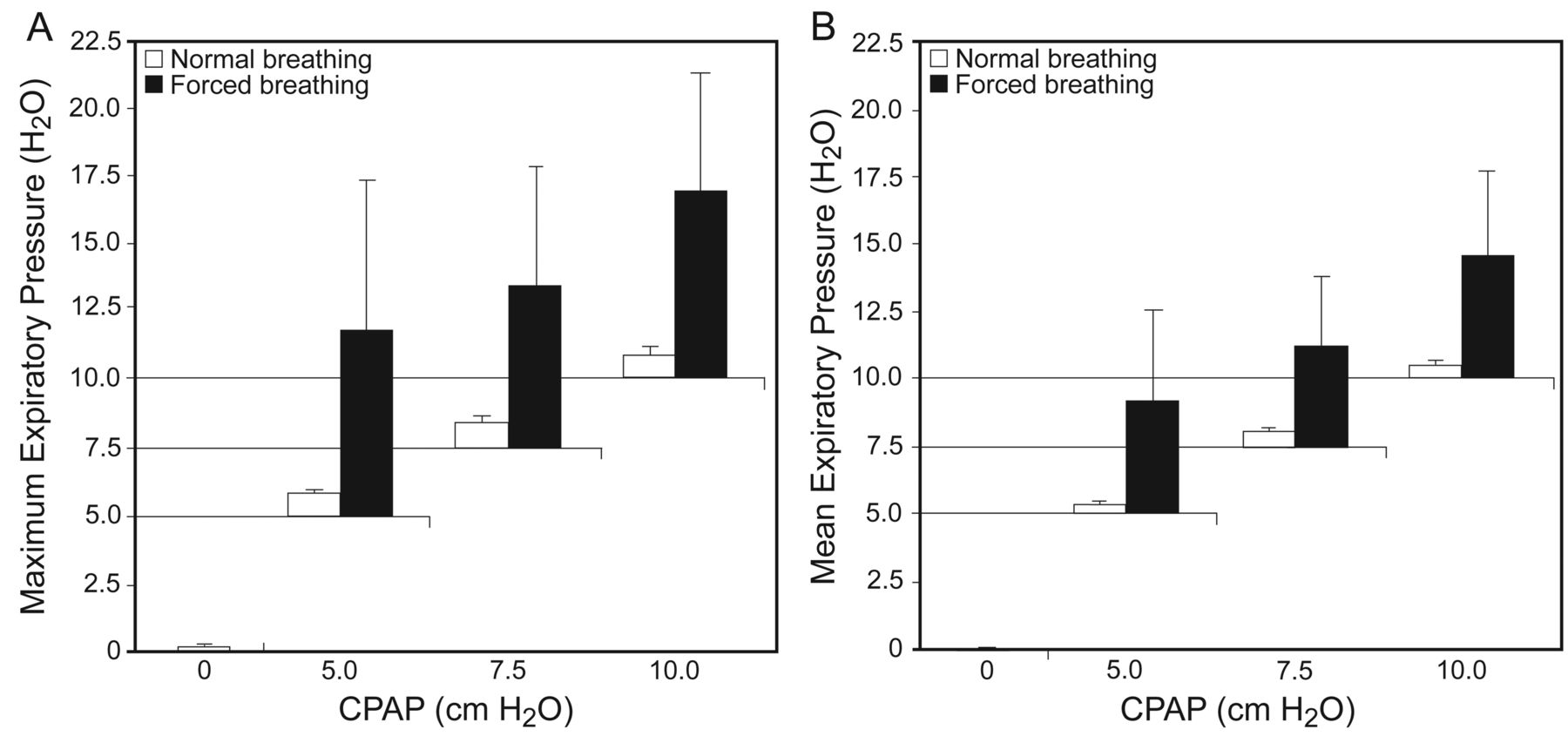
Figure 6 shows the maximum and mean airway pressure increases during expiration. Both the maximum and mean airway pressure was slightly higher during CPAP of 5.0, 7.5, and 10.0 cm H2O than during control normal breathing. Airway pressure increased with increasing CPAP. The airway pressure increase was higher during forced breathing than during control normal breathing or normal breathing at that CPAP level.
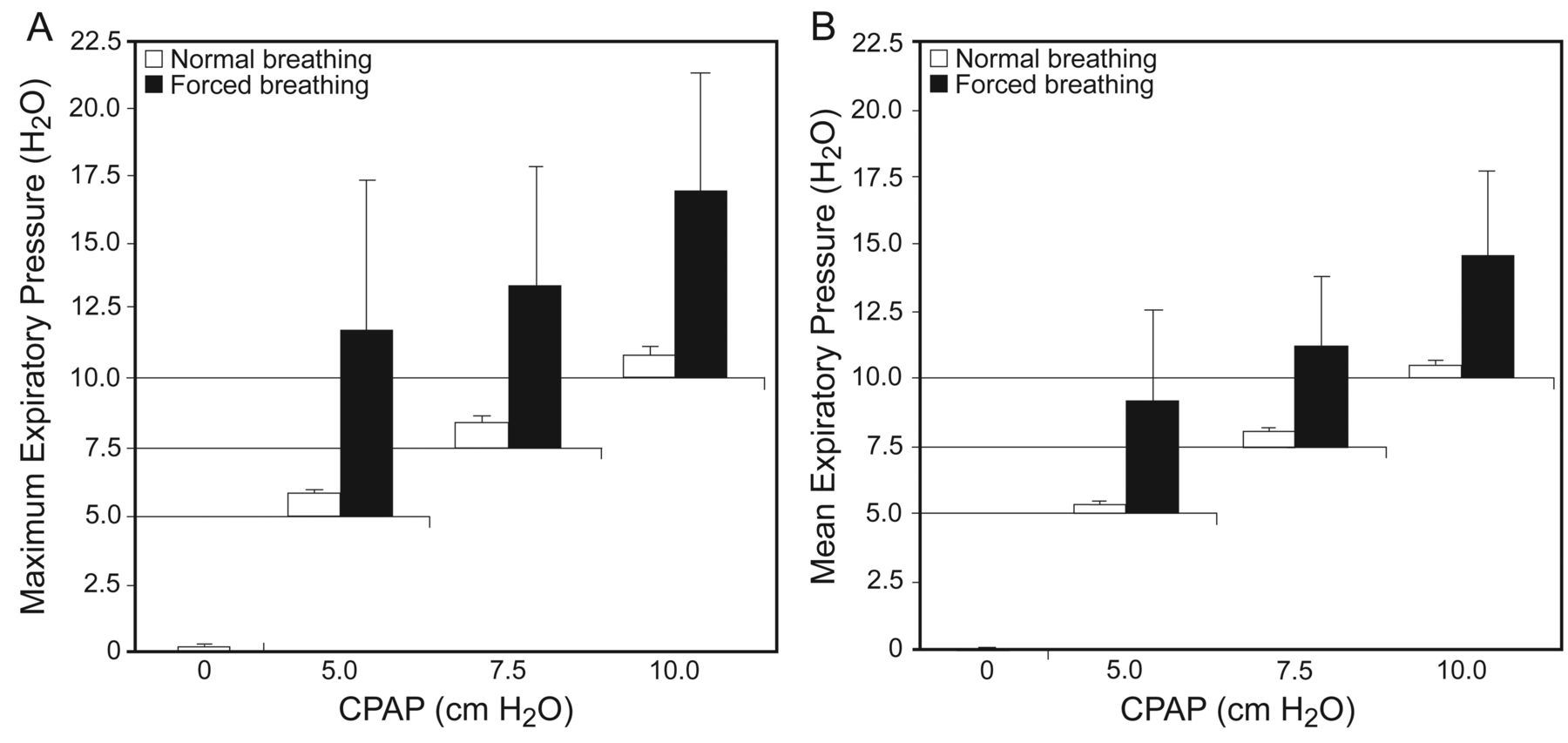
A: Maximum expiratory airway pressure at 4 continuous positive airway pressure (CPAP) levels, during normal breathing and forced breathing. P < .001 for control versus normal breathing and forced breathing, at all CPAP levels. P < .001 for normal breathing at CPAP of 5 cm H2O versus 7.5 cm H2O, and P = .026 for CPAP of 7.5 cm H2O versus 10 cm H2O. P < .001 for normal breathing versus forced breathing at the corresponding CPAP levels. B: Mean expiratory airway pressure. P < .001 for control versus normal breathing and forced breathing, at all CPAP levels. P < .001 for normal breathing at CPAP of 5 cm H2O versus 7.5 cm H2O, and for CPAP of 7.5 cm H2O versus 10 cm H2O. P < .001 for normal breathing versus forced breathing at the corresponding CPAP levels.
Changes in Air Flow
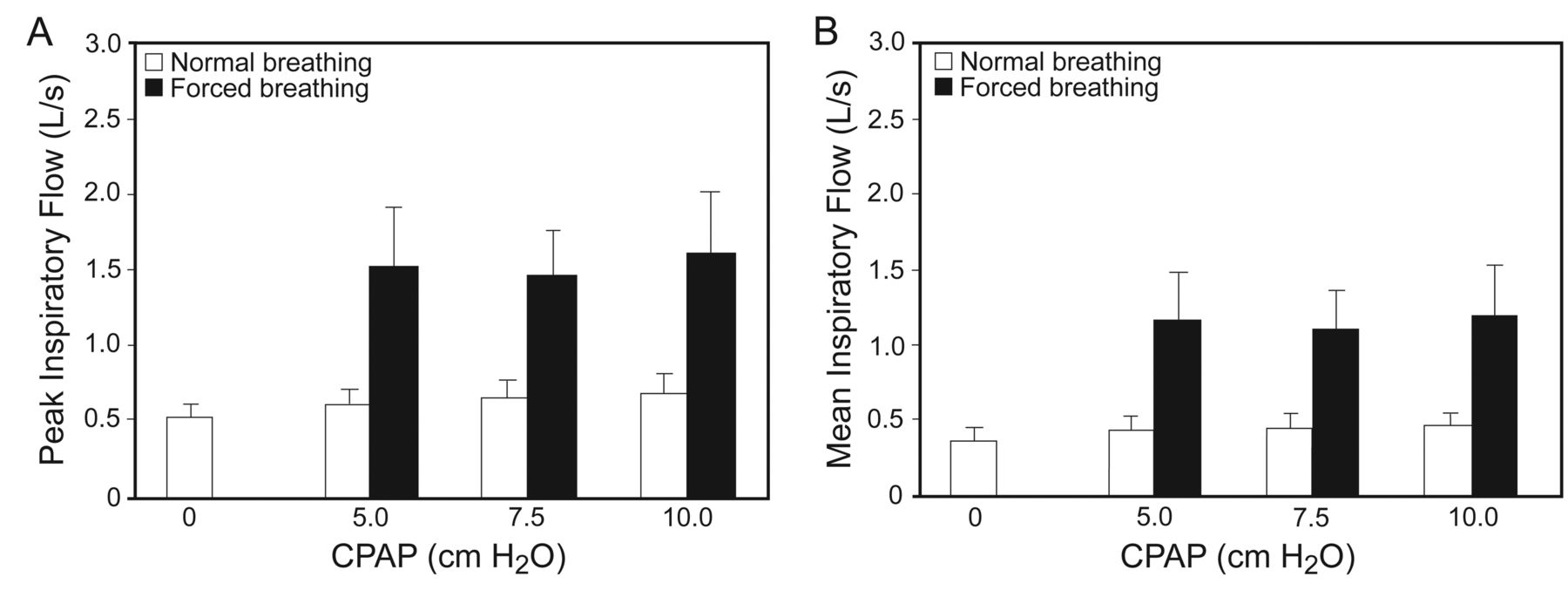
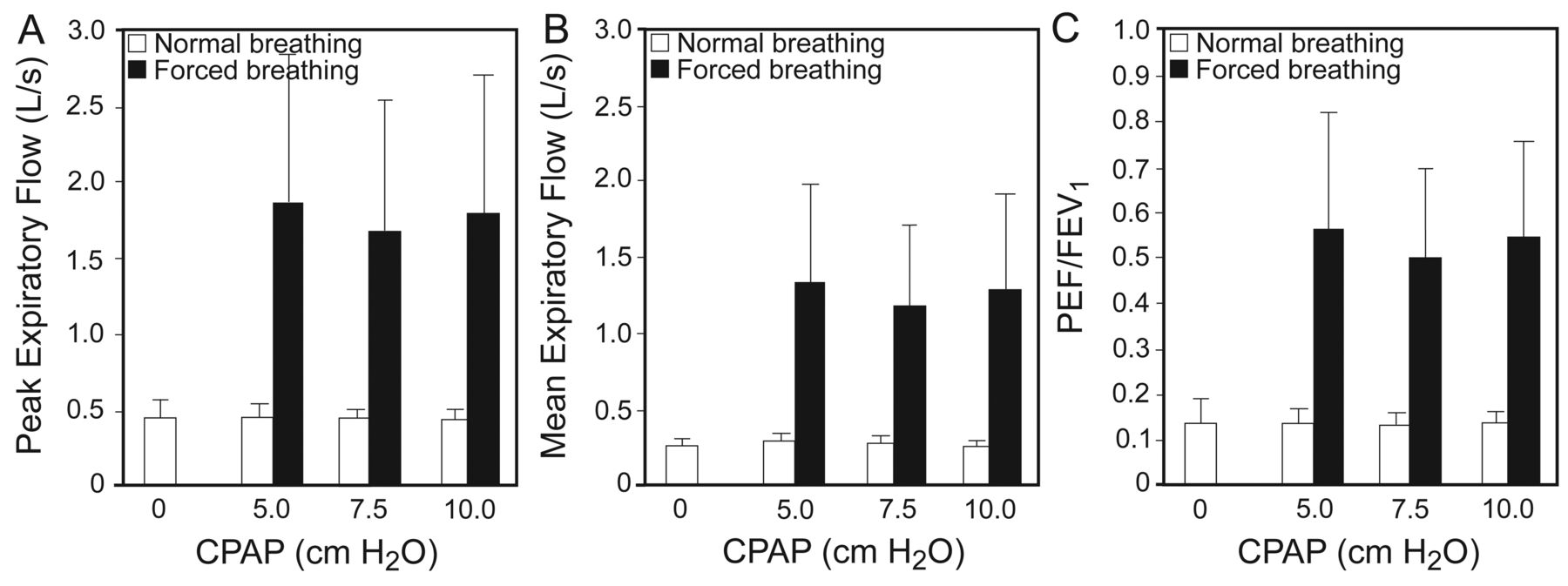
Figures 7 and 8 show the peak and mean inspiratory and expiratory flows, respectively. Figure 8 also shows the ratio of peak expiratory flow to FEV1. Both the peak and mean inspiratory and expiratory flows were higher during forced breathing than during breathing normally at the corresponding CPAP levels. The peak and mean inspiratory and expiratory flows were higher during normal and forced CPAP breathing than during control normal breathing. During normal breathing, peak expiratory flow was 14% of FEV1, irrespective of the CPAP level. During forced breathing, peak expiratory flow was 49–56% of FEV1.
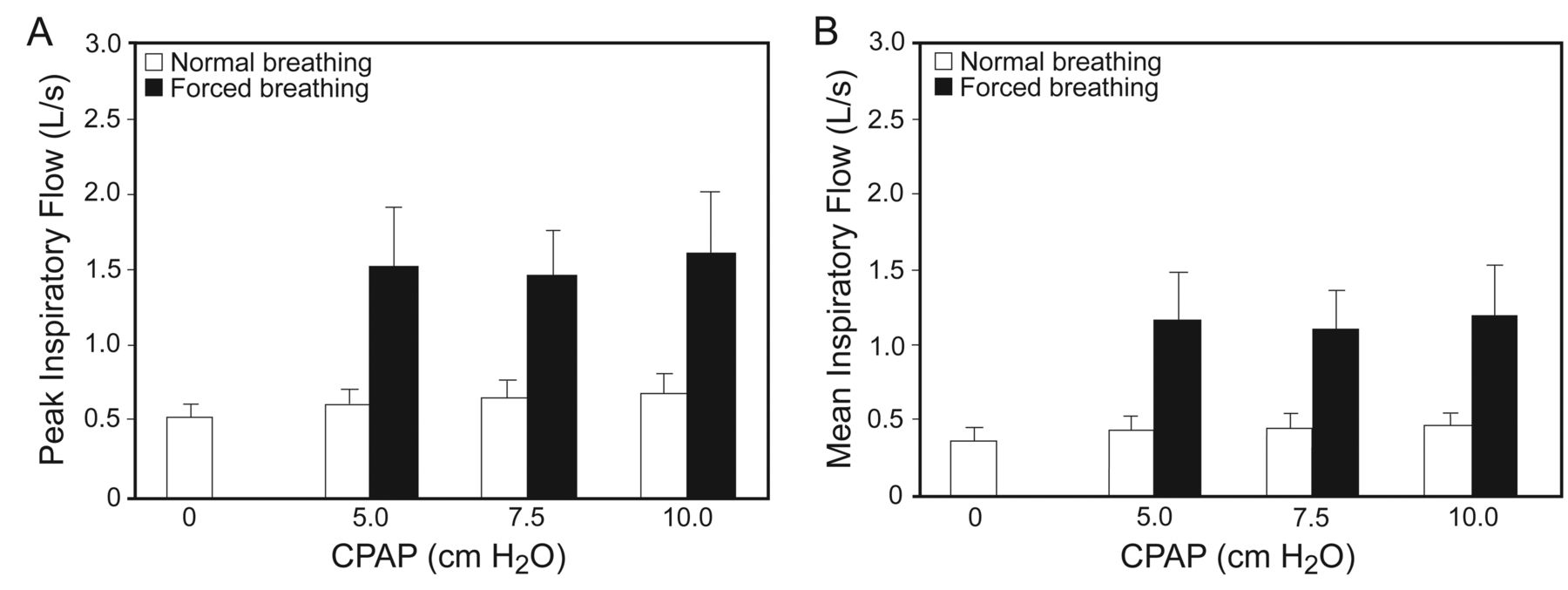
A: Peak inspiratory air flow at 4 continuous positive airway pressure (CPAP) levels, during normal breathing and forced breathing. P = .02 for control versus normal breathing at CPAP of 5 cm H2O. P = .003 for control versus normal breathing at CPAP of 7.5 cm H2O. P = .001 for control versus normal breathing at CPAP of 10 cm H2O. P < .001 for control versus forced breathing, at all CPAP levels. P < .001 for normal breathing versus forced breathing at the corresponding CPAP levels. B: Mean inspiratory air flow. P = .045 for control versus normal breathing at CPAP of 5 cm H2O. P = .03 for control versus normal breathing at CPAP of 7.5 cm H2O. P = .004 for control versus normal breathing at 10 cm H2O. P < .001 for control versus forced breathing, at all CPAP levels. P < .001 for normal breathing versus forced breathing at the corresponding CPAP levels.
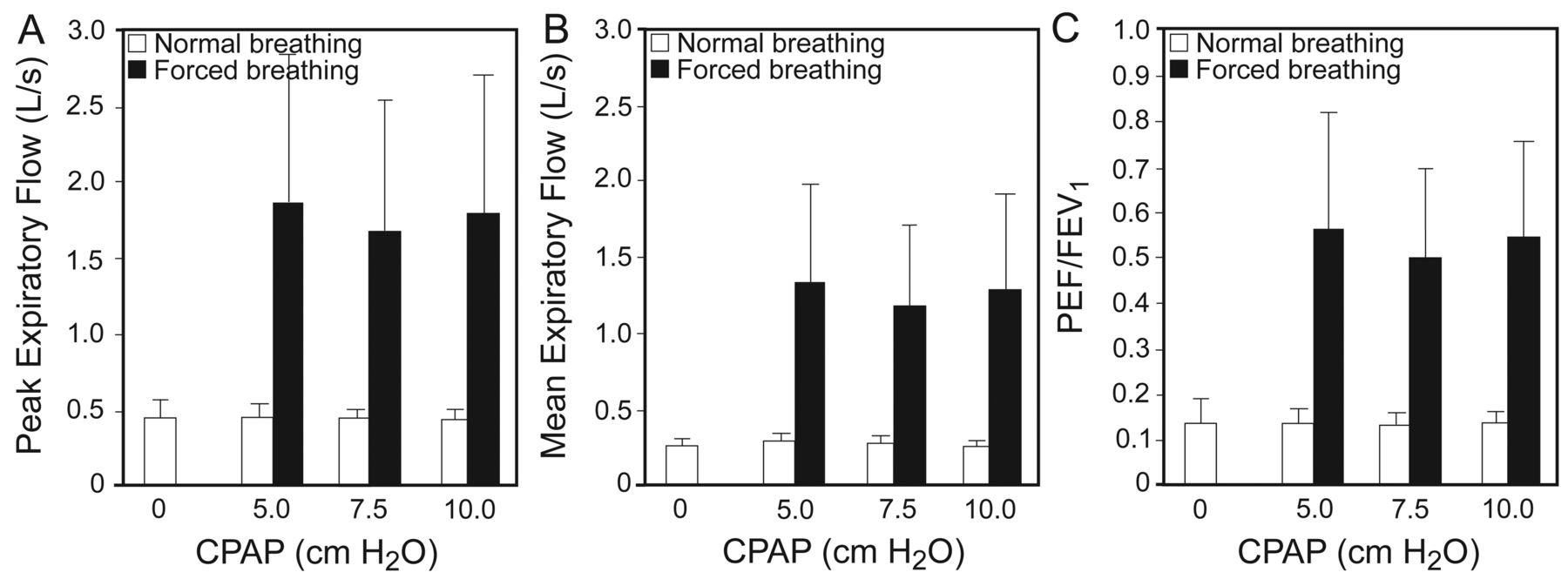
A: Peak expiratory flow at 4 continuous positive airway pressure (CPAP) levels, during normal breathing and forced breathing. P < .001 for control versus forced breathing, at all CPAP levels, and for normal breathing versus forced breathing at the corresponding CPAP levels. B: Mean expiratory flow. P < .001 for control versus forced breathing, at all CPAP levels, and for normal breathing versus forced breathing at the corresponding CPAP levels. C: Ratio of peak expiratory flow to FEV1. P < .001 for control versus forced breathing, at all CPAP levels, and for normal breathing versus forced breathing at the corresponding CPAP levels.
Breathing Pattern
Table 1 shows the inspiratory and expiratory time, respiratory rate, and end-tidal CO2 data. Both inspiratory and expiratory time were longer, at all CPAP levels, during normal breathing than during forced breathing. During normal breathing end-tidal CO2 decreased slightly with increasing CPAP level.
Inspiratory Time, Expiratory Time, Respiratory Rate, Breathing Pattern, and End-Tidal CO2
Figure 9 shows the inhaled volume, exhaled volume, and ratio of exhaled volume to VC data. Both the inhaled and exhaled volumes were higher during forced breathing than during normal breathing, at all CPAP levels. There were no volume differences between the normal breaths or between the forced breaths at any CPAP level. When breathing normally, at all 4 CPAP levels, tidal volume was 20% of VC. During the forced breaths the participants breathed at 38–42% of their VCs.

A: Inhaled volume per breath at 4 continuous positive airway pressure (CPAP) levels, during normal breathing and forced breathing. P < .001 for control versus forced breathing, at all CPAP levels, and for normal breathing versus forced breathing at the corresponding CPAP levels. B: Exhaled volume per breath. P < .001 for control versus forced breathing, at all CPAP levels, and for normal breathing versus forced breathing at the corresponding CPAP levels. C: Ratio of exhaled volume to vital capacity (VC). P < .001 for control versus forced breathing, at all CPAP levels, and for normal breathing versus forced breathing at the corresponding CPAP levels.
Perceived Exertion
The median Borg CR10 scores were 0.7 (range 0–2.5) at 0 cm H2O, 1 (range 0–3) at 5 cm H2O, 2 (range 0–7) at 7.5 cm H2O, and 2.5 (range 1–7) at 10 cm H2O. The participant who interrupted breathing at 10 cm H2O scored the perceived exertion at 7.
Discussion
During 10-min normal breathing periods, when the participants breathed at 20% of VC, with a peak expiratory flow of 14% of FEV1, airway pressure decreased during inspiration and increased slightly during expiration. However, the airway pressure changes were never large enough to reduce airway pressure to below zero, indicating that the Boussignac CPAP system functioned well during normal breathing. However, pressure changes did occur during normal breathing, and these changes increased with increasing CPAP.
During forced breathing, expiratory volume was 38–42% of VC and peak expiratory flow was 49–56% of FEV1. During forced breaths, as air flow increased, both the drop in inspiratory airway pressure and the increase in expiratory airway pressure were more pronounced. The magnitude of these pressure changes was 10–12 cm H2O, resulting in negative airway pressure during inspiration. During expiration, the maximum airway pressure range was 11–16 cm H2O at 5–10 cm H2O.
Pressure changes during breathing with CPAP are associated with increased work of breathing,10,11,22 and it is therefore important that airway pressure is stable during the whole breathing cycle. When a patient's inspiratory air flow exceeds the air flow delivered by the CPAP equipment, airway pressure will fall, which will increase respiratory work and possibly lead to fatigue.10,11,22 Though the Borg CR10 scale is subjective and not a pressure-related measure of WOB, the perceived exertion scores from our subjects were quite low for all CPAP levels. Inter-individual differences in perceived exertion increased at higher CPAP levels. One of our participants interrupted the 10 cm H2O trial due to severe respiratory distress and scored that perceived exertion at 7. We did not measure perceived exertion during forced breathing. The discrepancy between the positive findings obtained in some clinical studies and our observation of inadequate pneumatic performance of the Boussignac CPAP system during forced breathing and the perceived exertion in association with CPAP breathing raises doubts about the clinical relevance of these experimental findings. Thus, further physiological studies in patients with acute respiratory distress are warranted. Such studies should focus on the effective consequences of the observed pneumatic instability of the Boussignac CPAP system during forced breathing when used by patients with increased ventilatory needs.
In a bench study of 4 different Boussignac CPAP systems (one unmodified system and 3 modified systems), Bellani and co-workers10 reported on pressure changes and oxygen concentrations during CPAP breathing. Pressure drop during inspiration correlated to increased air flow. In their model, during expiration, with increased air flow and consequent increased tidal volume, airway pressure increases were enhanced during expiration. Thus, similar to our observations, caution is necessary when air flow is enhanced.
Except for the present study and the study by Bellani and co-workers,10 we are only aware of one other study on airway pressure with the Boussignac CPAP system.13 The main focus of that study was the applicability of the system in prehospital care of patients with acute pulmonary edema. Those authors reported on differences between inspiratory and expiratory pressures. Similar to our data, and data from Bellani and co-workers,10 they reported greater pressure differences at higher CPAP levels.13 None of the other studies we know of (see the Introduction section above) focused on airway pressure.
Some methodological aspects have to be discussed. First, we chose CPAP levels of 5.0, 7.5, and 10.0 cm H2O in concordance with CPAP levels most often used in everyday clinical practice. In our experience, at higher CPAP levels, the risk of air leak around the face mask is increased. With CPAP higher than 10 cm of H2O it is almost impossible to avoid air leak, so we chose 10 cm H2O as the highest CPAP. Further, air leak is an obstacle to accurate measurement, and with one participant the data from the 10 cm H2O session had to be omitted for this reason. One could argue that the progressive impairment of the pneumatic performance of the Boussignac system at higher CPAP is due to increased mask leak, but it was not possible to evaluate the impact of air leaks on the observed changes in airway pressure under the increasing CPAP levels, so a bench study may have better addressed this phenomenon.
Second, we evaluated both normal and forced breathing. The at-rest flow is reported to be 20–30 L/min, and in respiratory failure flow over 100 L/min is often seen.11 To simulate respiratory distress, our participants took 10 deep, forced breaths, and had flows of 88–97 L/min, which is consistent with flows reported during respiratory distress.11 Our instructions to the participants on how to perform the forced breaths can be questioned. Various participants responded very differently to the instructions, with very different breathing patterns. However, all the participants received identical instructions, read from a written instruction sheet. It could be argued that the participants also should have performed forced breaths at the control CPAP level (0 cm H2O), but our aim was to test the Boussignac system during CPAP breathing with air flows similar to respiratory distress: not to measure air flows during forced breathing without CPAP.
Third, since we used healthy volunteers the air flow and volumes could not be standardized, as in a bench study, which made it impractical to report exact pressures during specific air flows. We did not measure blood pressure, so we collected no data on the potential impact of CPAP on cardiovascular variables.
Fourth, we used a different filter for the air flow and airway pressure signals than did Barbini and co-workers20 or Avanzolini and co-workers,21 but we do not think that the small differences in cut-off frequency (3 Hz) or filter type (ie, Hanning instead of Hamming window) affected our results.
Conclusions
Based on our findings, and the results from Bellani and co-workers,10 we conclude that the pneumatic performance of the Boussignac CPAP system is adequate during normal breathing with low air flow, but during forced breathing and high air flow the Boussignac CPAP system is unable to maintain stable airway pressure, which could increase the work of breathing and cause respiratory fatigue. Thus, the Boussignac CPAP system might be less suitable for patients breathing at a higher frequency.
Footnotes
- Correspondence: Maria Sehlin RPT MSC, Department of Surgical and Perioperativ Sciences, Anesthesiology and Intensive Care Medicine, Umeå University Hospital, 90185 Umeå, Sweden. E-mail: maria.sehlin{at}anestesi.umu.se.
-
The study was supported by grants from Västerbotten County Council and the Medical Faculty of Umeå University.
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}