

Introduction
Unexpected and puzzling variations in bronchial anatomy might be discovered during bronchoscopy. The occurrence of congenital tracheobronchial anomaly is estimated to range between 1% and 12% of the overall population.1 We present 2 rare cases of congenital bronchial anomaly that were discovered during bronchoscopy and that emphasize the value of computed tomogram (CT) in diagnosing congenital tracheobronchial anomaly.
Case Summary 1
During bronchoscopy in a 64-year-old man who was sent for evaluation of a left lower lobe mass, trifurcation of the right main bronchus in a linear pattern was discovered (Fig. 1). Bronchus A arose from the lateral wall of the proximal right main bronchus and ran cranially (video of the bronchoscopy is available at http://www.rcjournal.com). Bronchus B originated next to bronchus A and divided into 2 segmental branches. Bronchus C coursed caudally and divided into 2 lobar bronchi as the normal pattern of the bronchus intermedius.

Bronchoscopic view of the right main bronchus in patient 1. See text for details.
Two-dimensional coronal CT revealed the origins and the courses of bronchi A, B, and C (Fig. 2). Bronchus A ran cephalad, supplied the apical segment of the right upper lobe (S1) and was considered to be a displaced right pre-eparterial bronchus. Bronchus B extended horizontally and divided into 2 segmental branches supplying the posterior (S2) and anterior (S3) segments of the right upper lobe. Therefore, we concluded that bronchus B was the right upper lobe bronchus.

Two-dimensional coronal computed tomogram of patient 1, with lung-window setting, shows the locations of the bronchi we refer to as A, B, and C.
Case Summary 2
A 65-year-old woman underwent flexible bronchoscopy for persistent right upper lobe infiltration. Bronchoscopy revealed a normal bronchial tree on the right side. Surprisingly, there was trifurcation of the distal end of the left main bronchus in the inverse triangular pattern (Fig. 3). The course of bronchus A ran cephalad and divided into 2 branches. Bronchus B extended anteriorly and then bifurcated into upper and lower segmental bronchi. The upper one divided into lateral and medial branches, and the lower one bifurcated superiorly and inferiorly. Bronchus C coursed caudally and divided into 4 segmental bronchi, as the normal pattern of the left lower lobe bronchus: superior, anteromedial, lateral, and posterior segmental bronchi.

Bronchoscopic view at the distal end of the left main bronchus in patient 2.
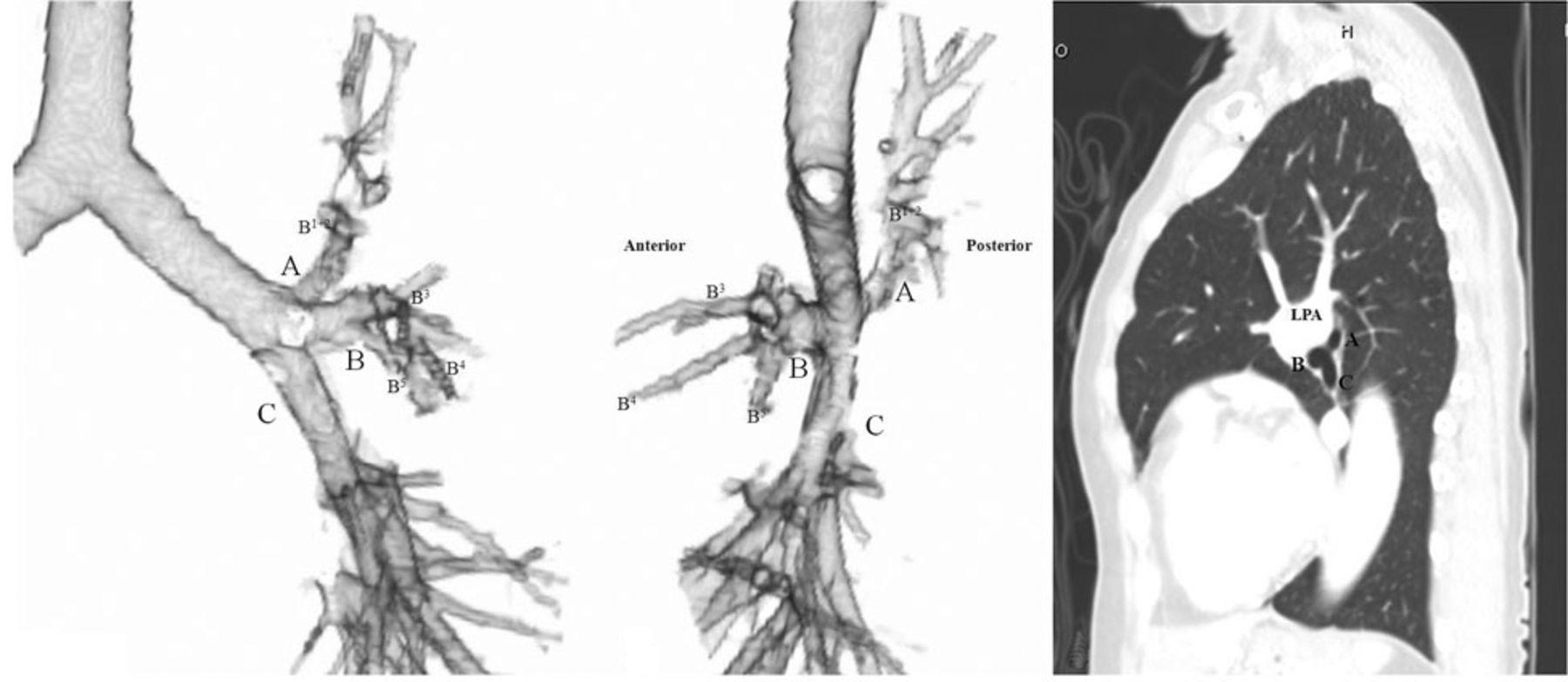
Figure 4 shows 3-dimensional bronchographic images and CT of the left bronchial tree. Bronchus A originated from the posterior aspect of the distal left main bronchus and below the arch of the left pulmonary artery. It ran cephalad and supplied only the apicoposterior segment (S1+2) and was considered to be a displaced pre-hyparterial bronchus. Bronchus B coursed anteriorly and then bifurcated. The upper branch subdivided into lateral, medial, and superior subsegmental bronchi, and supplied the anterior territory of the upper lobe (S3). The lower branch of bronchus B supplied the superior (S4) and inferior (S5) segments of the lingular division. Bronchus B was considered to be the left upper lobe bronchus because its origin was in the hyparterial location and closed to the left lower lobe bronchus. There was also an accessory fissure of the left upper lobe (Fig. 5), which curved anterolaterally to the chest wall, compatible with a type I fissure in Berkmen's CT classification of the accessory fissures of the left upper lobe.2 This fissure separated S1+2 from S3.

Computed tomography bronchography of the left bronchial tree in patient 2. Left: Anterior view. Middle: Lateral view. Right:Sagittal computed tomogram with lung-window setting. The 3 bronchi of the trifurcation of the left main bronchus are labeled A, B, and C. The arch of the left pulmonary artery is above the origin of bronchus A. B1+2 is the apicoposterior segment. B3 is the anterior segment. B4 is the superior segment, lingula. B5 is the inferior segment, lingula. LPA is the left pulmonary artery.

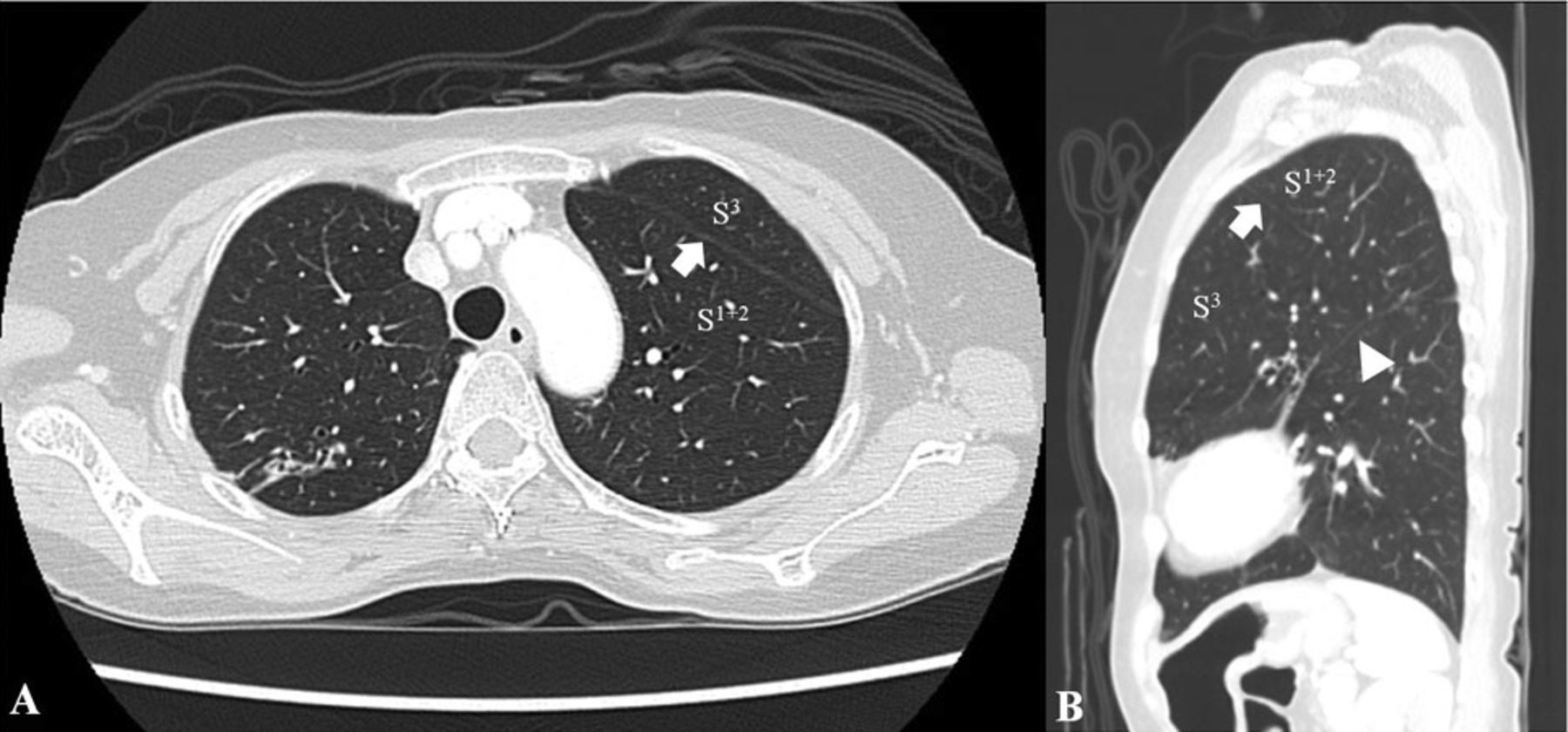
Axial (A) and sagittal (B) computed tomograms of patient 2, with the lung-window setting, show an accessory fissure (arrow) separating S1+2 (apicoposterior segment) from S3 (anterior segment). The arrowhead points to the left major fissure.
Discussion
Tracheal bronchus was first described by Sandifort as a right upper lobe bronchus originating from the trachea. Recently the scope of the tracheal bronchus has encompassed various bronchial anomalies arising either from main bronchi or the trachea and supplying the upper lobe territory.1 A tracheal bronchus arising from the main bronchus is termed according to the position of its origin.1 On the right side, an anomalous bronchus that originates proximal to the origin of an upper lobe bronchus is termed pre-eparterial, whereas an anomalous bronchus that arises distal to the origin of an upper lobe bronchus is termed post-eparterial. On the left side, an anomalous bronchus with an origin above the arch of the left pulmonary artery is termed an eparterial bronchus. For anomalous bronchi that lie below the arch of the left pulmonary artery, a pre-hyparterial bronchus arises proximal, whereas a post-hyparterial bronchus arises distal to the origin of the upper lobe bronchus.
Tracheal bronchus is further subdivided into supernumerary and displaced types.1 The supernumerary type is where there is a normal branching of the upper lobe bronchus. In the absence of normal branching of the upper lobe bronchus, an anomalous bronchus that aerates one or more missing segments of the upper lobe is described as the displaced type.
In patient 1, bronchus A was a displaced right pre-eparterial bronchus because it represented an anomalous right apical segmental bronchus (B1) that originated proximal to the origin of the upper lobe bronchus, whereas B1 was missing from the right upper lobe bronchus.
In patient 2, bronchus A was a displaced left pre-hyparterial bronchus because it represented an anomalous left apicoposterior segmental bronchus (B1+2) that originated above the origin of the left upper lobe bronchus and below the arch of the left pulmonary artery, whereas B1+2 was missing from the left upper lobe bronchus.
Normally, B1+2 and the anterior segmental bronchus of the left upper lobe (B3) coexist from the left upper divisional bronchus. Although trifurcation of the left main bronchus was previously described by Beder et al3 and Doshi and Mehta,4 they gave no additional detail on the segmental divisions of both bronchi that supplied the left upper lobe. However, in all cases having the displaced left pre-hyparterial bronchus, Ghaye et al1 found that this bronchus supplied only the S1+2, while the B3 and lingular bronchus originated from a common trunk, as in the present case.
Accessory fissures of the left upper lobe are occasionally found on CT. The so-called left minor fissure, which separates S3 from S4, is the most common. The fissure that separates S1+2 from S3 (as in patient 1) was found only in 2 cases in the series reported by Berkmen et al.2 That fissure ran convex laterally to the chest wall.
Because the lung portion supplied by each branch of the left main bronchial trifurcation was separated from each other by the accessory fissure and the left major fissure, it would be described as a lobe. In patient 2, according to the origin and supply, we prefer to name these 3 lobes the pre-hyparterial lobe, the hyparterial lobe, and the left lower lobe, to avoid confusion with the normal left lung. To our knowledge, these coexisting variations have been briefly described only by Desir and Ghaye.5 Nevertheless, we speculate that all such anomalies always coexist and are unique to the left main bronchial trifurcation. CT is helpful in studying these anomalies.
There are 3 theories for the development of anomalous bronchi: reduction, migration, and selection.6 In our cases, the aberrant bronchi were displaced bronchi directing to the right S1 and the left S1+2 that missed from the upper lobe bronchi. Therefore, the migration theory would be appropriate to explain their origin. The subsidiary branches can migrate from their initial loci to new points of origin of a bronchus.1 Like a normal right upper lobe bronchus that migrates from its hyparterial position to its eparterial location on the right main bronchus, the right B1 might migrate from its position to the lateral aspect of the right main bronchus proximal to the origin of the right upper lobe bronchus. Likewise, the left B1+2 might migrate from its position to the posterior aspect of the distal left main bronchus close to the origin of the left upper lobe bronchus, which results in the trifurcation of the left main bronchus.
Teaching Points
Congenital variations in bronchial anatomy are not uncommon and may be discovered during bronchoscopy. Knowledge of and familiarity with bronchoscopic views and CT images of normal and abnormal bronchi are necessary for bronchoscopists to perform bronchoscopy perspicaciously.
A 2-mm CT slice interval can provide the required details of the branching and courses of bronchi. Recognition of anomalies on CT before bronchoscopy is important to avoid confusion during bronchoscopy, to provide an accurate “road map,” and to guide the planning of interventions.
The scope of the tracheal bronchus encompasses various bronchial anomalies arising from either main bronchi or the trachea and supplying the upper lobe territory. A tracheal bronchus arising from the main bronchus is designated according to the position of its origin and is further subdivided into supernumerary and displaced types, in relation to the presence of normal branching of the upper lobe bronchus.
Acknowledgments
We thank Pensupa Raweelert MD and Amnuay Thithapandha PhD for constructive suggestions and editing.
Footnotes
- Correspondence: Viboon Boonsarngsuk MD, Division of Pulmonary and Critical Care Medicine, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Rama VI Road, Phayathai, Bangkok 10400, Thailand. E-mail: bss-vb{at}hotmail.com.
-
The authors have disclosed no conflicts of interest.
-
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}