

Abstract
BACKGROUND: Mechanical ventilation technology has evolved rapidly over the last 30 years. One consequence is the creation of an unmanageable number of names to describe modes of ventilation. The proliferation of names makes education of end users difficult, potentially compromising the quality of patient care.
OBJECTIVE: To determine if stakeholders are familiar enough with published constructs related to modes of mechanical ventilation to form a basis for a consensus, by surveying the medical, education, and business communities. The hypotheses tested were: there is concordance (> 50%) on 10 basic constructs related to modes; concordance with the basic constructs varies among stakeholders according to professional training and professional activity; and concordance varies among the set of constructs.
METHODS: The survey was distributed through an Internet-based tool to 2,994 physicians, respiratory therapists, nurses, engineers, and others involved with mechanical ventilation. Hypotheses were tested with chi-square, with P < .05 considered significant.
RESULTS: The response rate was 15%. Respondents were 55% respiratory therapists, 35% physicians, 3% nurses, 1% engineers, and 5% other professionals. There was an 82% concordance with the 10 constructs (P < .001). Respiratory therapists showed the highest degree of concordance (84%) and “other profession” showed the lowest (79%) (P = .006). No significant difference (P = .07) in concordance was observed when data were grouped by professional activity. Concordance differed significantly among the survey questions (P < .001).
CONCLUSIONS: Survey results indicate that respondents were either familiar with or amenable to the previously published literature that the survey constructs represented. The degree of familiarity and concordance with these constructs represents a sufficient basis for attempting to formalize a taxonomy. Further analysis of the pattern of concordance among the constructs will inform future educational and consensus building efforts.
Introduction
In the profession of respiratory care, the most important knowledge and skills center on the assessment and management of life support. These cognitive and psychomotor skills are extensive and involve interventions ranging from cardiopulmonary resuscitation to mechanical ventilation management. In particular, initiating and managing mechanical ventilation is a skill that is not integrated into the medical school curriculum (at least in the United States). Therefore, medical students and physicians learn on the job, primarily from their respiratory therapy colleagues. Conversely, respiratory therapists have to undergo formal didactic and clinical training in mechanical ventilation.1 National credentialing examinations2 and state licensure agencies (eg, http://respiratorycare.ohio.gov) assess a respiratory therapist's competency in employing ventilatory strategies to achieve adequate support, evaluate the patient's response to therapy, and recommend changes to or independently modify the respiratory plan of care.
Like many other professions, respiratory care has experienced a remarkable increase in technological complexity in the last 30 years. Unfortunately, systems of formal education have not evolved rapidly enough to keep pace, particularly in the area of mechanical ventilation. A mechanical ventilator is an automatic machine designed to replace some or all of the work the body must produce to move air into and out of the lungs.3 In the most general terms, a “mode of ventilation” is a predetermined pattern of interaction between the ventilator and the patient. Thirty years ago, the average mechanical ventilator offered 2 or 3 mode selections. Today, state-of-the-art mechanical ventilators offer about 2 dozen unique modes, some of which even employ computerized artificial intelligence. In the course of one human generation, mechanical ventilators have evolved perhaps 5 generations. What has not evolved is a standardized classification system, or taxonomy, sufficient to describe this technological complexity. On the contrary, manufacturers have exacerbated the problem by coining a plethora of names for modes, in an effort to create product differential and increase sales.
As a result of not having a formal taxonomy, 4 major problems accrue:
Published studies of mechanical ventilation are hard to compare, and thus appropriate evidence for clinical practice is difficult to assemble and describe.
There is little consistency among educational programs regarding nomenclature and descriptions of how ventilators work.
Clinicians practicing in institutions with mechanical ventilators supplied by several different manufacturers (a very common situation) do not have the time or educational resources to receive adequate training and experience with all modes on all ventilators, making optimal ventilator management unattainable.
Manufacturers can no longer easily communicate with prospective clients regarding the detailed operation of their products in relation to competitive devices, thus limiting the effectiveness of both sales and training, which, in turn, exacerbates the other problems.
The lack of a taxonomy is not due to a lack of a peer reviewed foundation for one. Indeed, several papers and book chapters have been available for years, and some of it has been incorporated into the mainstream textbooks used by respiratory therapy educational programs. A recent paper summarizes the basic constructs and the outline of a taxonomy based on these previous publications.4 The online supplemental text (at http://www.rcjournal.com) provides a detailed review of these resources.
The purpose of this study was to determine if stakeholders are familiar enough with published constructs related to modes of mechanical ventilation to form a basis for a consensus, by surveying the medical, education, and business communities. Specifically, we sought to measure agreement on the part of the healthcare community (ie, including thought leaders in medicine, education, and business) with 10 fundamental constructs that could potentially form the basis of a ventilator mode taxonomy. Hereafter, “agreement” will be referred to as concordance, for reasons that will be explained in the Methods section. These constructs are derived from previous published works on mode classification in major textbooks and peer reviewed medical journals (see online supplemental text). The results of this study may inform future efforts to establish an international standard.
The specific hypotheses tested were as follows.
Among thought leaders in healthcare, there is sufficient concordance on 10 fundamental constructs related to mechanical ventilation modes to form the basis for a formal taxonomy. “Sufficient” in this context will be an average concordance across constructs of > 50%. The value of 50% was chosen as representing equipoise regarding the constructs.
Concordance with the basic constructs will vary among stakeholders, according to their professional training and professional activity.
The degree of concordance will vary among the set of constructs describing modes of mechanical ventilation.
QUICK LOOK
Current knowledge
Terminology to describe the modes of mechanical ventilation is inconsistent, leading to difficulty in communication and incomplete understanding of function by practitioners. Both consequences may reduce patient safety.
What this paper contributes to our knowledge
A formal taxonomy for mechanical ventilation is desirable and possible, based on the knowledge of the respiratory care community. Establishment of a formal taxonomy could reduce medical errors.
Methods
Study Design
This study was designed as a survey of stakeholders in a taxonomy of mechanical ventilation. The survey was based on 10 fundamental constructs (see the survey instrument in the supplemental text) derived from previous published works, as noted in the Discussion. Briefly, the constructs were as follows
Definition of a breath
Definition of an assisted breath
Definitions of pressure control (PC) and volume control (VC)
Definitions of trigger and cycle (ie, starting and stopping inspiration)
Machine versus patient triggering and cycling
Definition of spontaneous versus mandatory breaths
Breath sequences: continuous mandatory ventilation (CMV), intermittent mandatory ventilation (IMV), and continuous spontaneous ventilation (CSV)
Ventilatory patterns defined as control variable and breath sequence combinations, like VC-CMV or PC-IMV
Adding detail to ventilatory patterns using targeting (ie, feedback control) schemes
Using the above constructs to define “mode”
There were 10 questions for the 10 constructs; one question regarding the goal of a mode taxonomy; 3 questions regarding professional training, activity, and years of experience; and a final item for free-text comments.
The survey was based on the assumption that astute readers of the relevant literature have already formed mental concepts similar to these constructs. Thus, such people would be likely to agree with the constructs when they were formulated as specific, concise statements.
Population
A sample of healthcare professionals from around the world was surveyed, with representation from the medical, education, and business communities. We selected the sample from our personal contacts, and other sources as follows. Educators were identified from published lists of respiratory therapy program directors, such as that provided by the Committee on Accreditation for Respiratory Care. Clinician thought leaders were selected from published papers on mechanical ventilation in peer reviewed medical journals and from among the authors of textbooks on mechanical ventilation. Authors of published papers were identified using a PubMed search on the key words “mechanical ventilation” encompassing a period of 5 years from 2004 to 2009. Business leaders were selected from among our professional contacts in the ventilator manufacturing industry, and included engineers, clinical specialists, and marketing managers.
Inclusion Criteria
The following criteria were used in selecting the study population.
Professional training as a physician, respiratory therapist, nurse, engineer, or other medical professional, and familiarity with the topic of mechanical ventilation
Recognized thought leader, as determined by contributions to the published literature (clinicians), directing or instructing in a respiratory care program (educators), or designing ventilators or marketing materials (business leaders)
Exclusion Criteria
No exclusion criteria were imposed after selecting for the inclusion criteria. E-mails that were returned as “undeliverable” were of course not included.
Survey Instrument
The survey instrument was validated by a pilot study. This pilot study was conducted with a sample of volunteer respondents obtained from respiratory therapist members of the American Association for Respiratory Care educational specialty section electronic mailing list. The survey was returned by 8 respondents. The concordance with individual constructs ranged from 37.5% to 100%. The overall concordance was 84%. The results of this pilot study were presented as a poster at the 2009 International Respiratory Congress in San Antonio, Texas, and published in abstract form in the November issue of Respiratory Care.5 The encouraging results of this pilot study prompted the survey of a larger sample of stakeholders.
The final survey, incorporating slight changes in wording suggested by the pilot study, comprised 15 questions, 10 of which related to the constructs framed such that the respondent could respond on a 5 point scale from “strongly agree” to “strongly disagree” (see survey instrument in online supplemental text. The “correct” answers are indicated in bold.). The meaning of correct, in this case, is that the respondent agrees with a statement that supports a construct (or disagrees with a statement that negates a construct) derived from published papers and chapters on mode classification. Questions were designed so that the “correct” answers include both “strongly agree” and “strongly disagree” answers, in order to allow calculation of a kappa statistic. (Using only “strongly agree” answers would not allow the creation of a 2 × 2 matrix to calculate the statistic, as shown in Fig. 1).

Matrix used to calculate the kappa statistic. A = sum of concordant responses for positively worded survey questions 1, 3, 6, 7, 9 and 10. B = sum of discordant responses for negatively worded survey questions 4, 5, and 8. C = sum of discordant responses for questions 1–3, 6, 7, 9, and 10. D = sum of concordant responses for questions 4, 5, and 8. The numbers below the letters represent number of responses.
One additional question was designed to distinguish whether the primary goal of a taxonomy for mechanical ventilation is to serve clinicians or business. Three more questions were designed to help stratify results according to respondent training and primary professional activity (ie, patient care, education, or business). These data may prove helpful in designing and disseminating subsequent educational materials.
Participants were recruited through e-mail. Informed consent was implied and incorporated in the introduction to the survey (see survey instrument in online supplemental text). The survey was administered using the Internet service SurveyMonkey.com. The survey was reviewed by the institutional review board at Youngstown State University, and the research proposal was granted exempt status.
Invitations to participate in the survey were e-mailed internationally, to 385 educators, 112 authors of ventilation articles, 160 manufacturers' representatives, and 2,337 other people identified as respiratory therapists having involvement with mechanical ventilation. A total of 2,994 survey invitations were sent worldwide.
Outcome Measures
The survey was worded such that the respondents were asked whether they agreed or disagreed with 10 theoretical constructs. Because acceptance of the underlying construct of a given question could be represented either as “agree” or “disagree,” depending on the wording of the question, the primary outcome measure was defined as average concordance of survey respondents. A secondary outcome was calculation of the kappa statistic to quantify the overall concordance.
Data Analysis
There were 5 possible responses (ie, an ordinal scale from strongly disagree to strongly agree). Responses to the questions were counted as concordant if they supported the underlying construct. For example, question 2 stated that an assisted breath is one for which the ventilator does work on the patient. All the “strongly agree” and “agree” responses to this question were counted as concordant responses, while all the “neutral,” “disagree,” and “strongly disagree” responses were counted as discordant.
Questions 4, 5, and 8 were worded such that disagreement supported the underlying construct, and thus responses of “disagree” and “strongly disagree” were counted as concordant. For example, question 5 was “Knowing what actions start (trigger) and stop (cycle) inspiration has little clinical importance.” The underlying construct is that trigger and cycle actions do have clinical importance. Therefore, all responses of “disagree” and “strongly disagree” were counted as concordant, while responses of “neutral,” “agree,” and “strongly agree” were counted as discordant for this item. Concordance for the set of 10 questions was calculated as the sum of the concordant responses divided by the total number of responses (ie, the percent of responses that supported or agreed with the underlying constructs).
Hypothesis 1.
To test the hypothesis that sufficient concordance exists to establish a consensus, the overall concordance percentage was compared to the arbitrary value of 50% using a chi-square test.
Hypothesis 2.
To test the hypotheses that concordance varies among stakeholders stratified by profession and professional activity, percent concordances were compared using chi-square tests.
Hypothesis 3.
To test the hypothesis that concordance differs among constructs, percent concordance was compared using a chi-square test.
For all hypotheses tests, differences associated with P values < .05 were considered significant. Qualitative ranking of the degree of agreement based on the kappa statistic was done using the system of Landis and Koch,6 as described by Feinstein,7 as shown in Table 1.
Qualitative Ranking of the Degree of Agreement Based on the Kappa Statistic
Results
Description of Subjects
Of the 2,994 surveys e-mailed to potential respondents, 185 were returned as “undeliverable.” Thus, the sample size for the survey was estimated to be 2,809 people, although it was probably smaller due to some e-mails never being delivered or read. We received survey responses from 432 individuals (15.4% response rate) between May 8, 2009, and October 9, 2009. The total response grouped by primary professional training is shown in Table 2.
Professional Training
The years of experience for the professional groups are shown in Table 3. The total response grouped by primary professional activity is shown in Table 4. Five respondents skipped question number 1.
Professional Experience
Professional Activity
Data Analysis for Hypothesis 1
The concordance for all responses was calculated as the total number of concordant responses divided by the total number of responses. The overall concordance was 82.4%, which was significantly larger than the postulated 50% (P < .001). The data support the first hypothesis that sufficient (ie, > 50%) concordance exists to establish a consensus.
The kappa statistic was evaluated with an online calculator8 for the 2 × 2 matrix shown in Figure 1. The kappa statistic was 0.617 (95% CI 0.592–0.642). This value for kappa corresponds to a quantitative level of “substantial” agreement.7
Data Analysis for Hypothesis 2
When the data were grouped by profession, respiratory therapists showed the highest degree of concordance (84.3%) and “other profession” showed the lowest (79.1%), as shown in Figure 2 (P = .006).
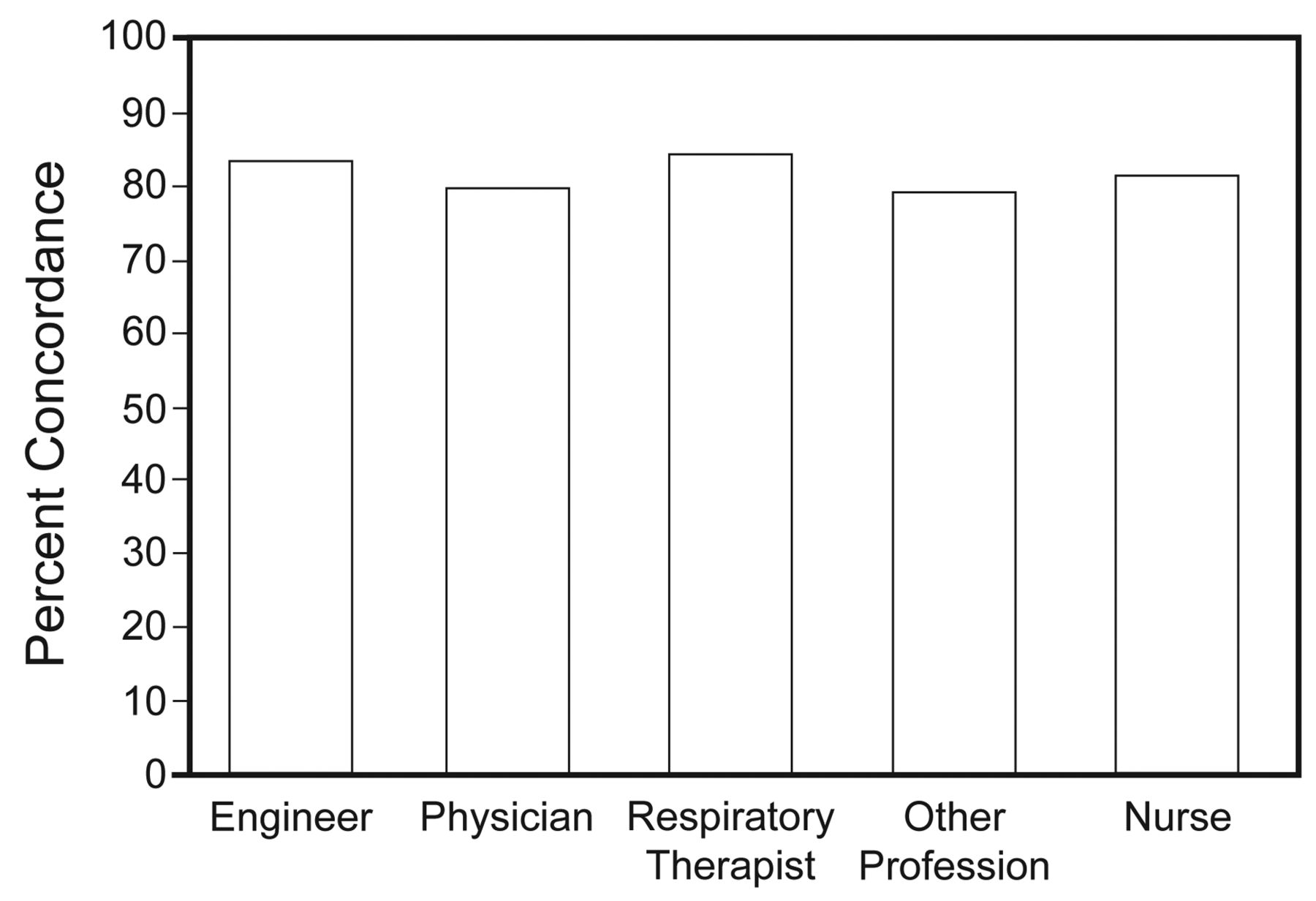
Concordance when data were grouped by profession.
Figure 3 shows a closer look at how the different professional groups answered individual survey questions. All groups tended to show lower concordance on question 3, but particularly so for engineers.

Response to survey questions by different professional groups.
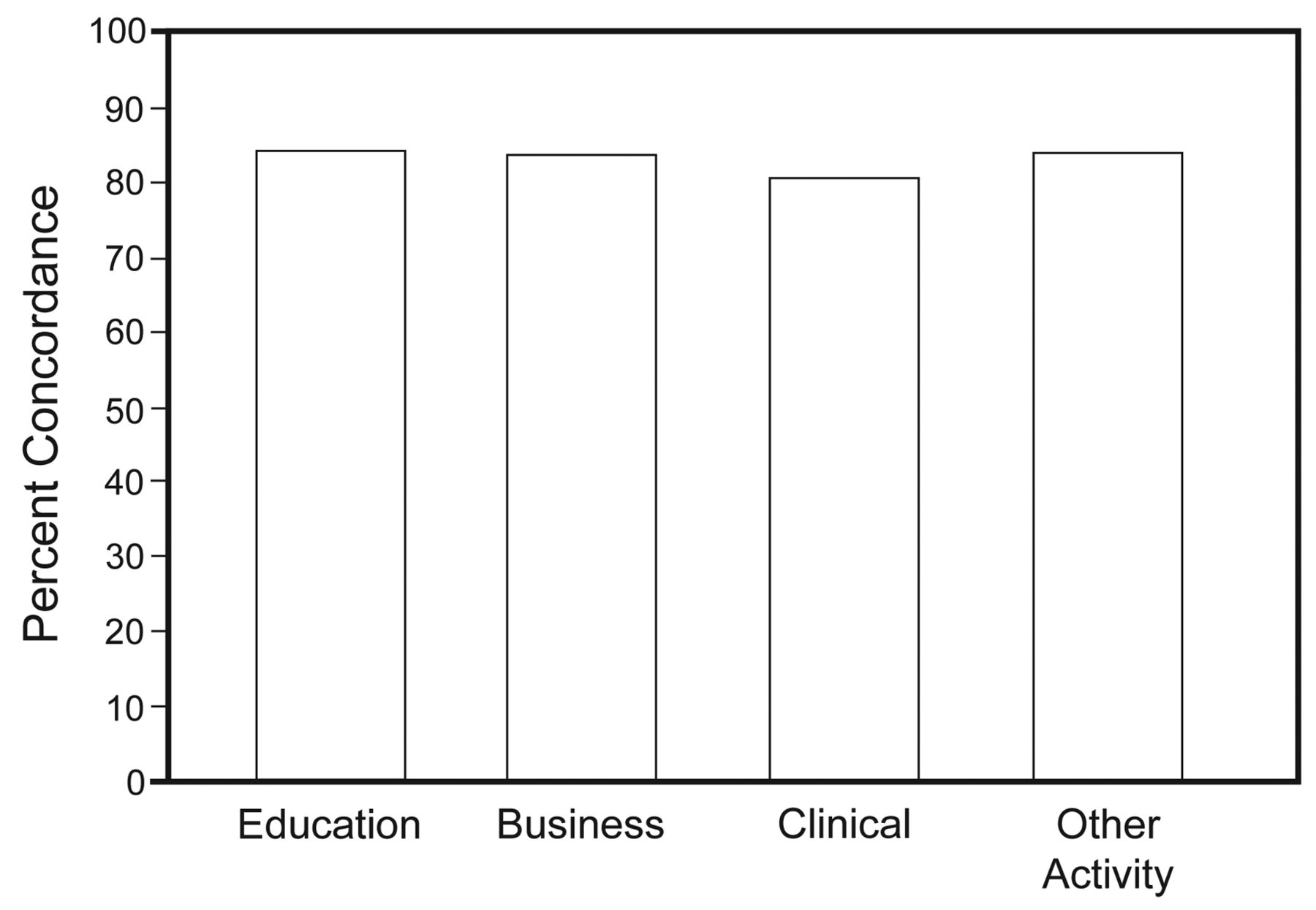
When the data were grouped by professional activity, there was no significant difference in concordance, as shown in Figure 4 (P = .07).

Concordance when data were grouped by professional activity.
Figure 5 shows a closer look at how the different professional activity groups compared on individual survey questions. Of note, the “other activity” group scored lowest on questions 1 and 2, while the business group scored lowest on question 8.
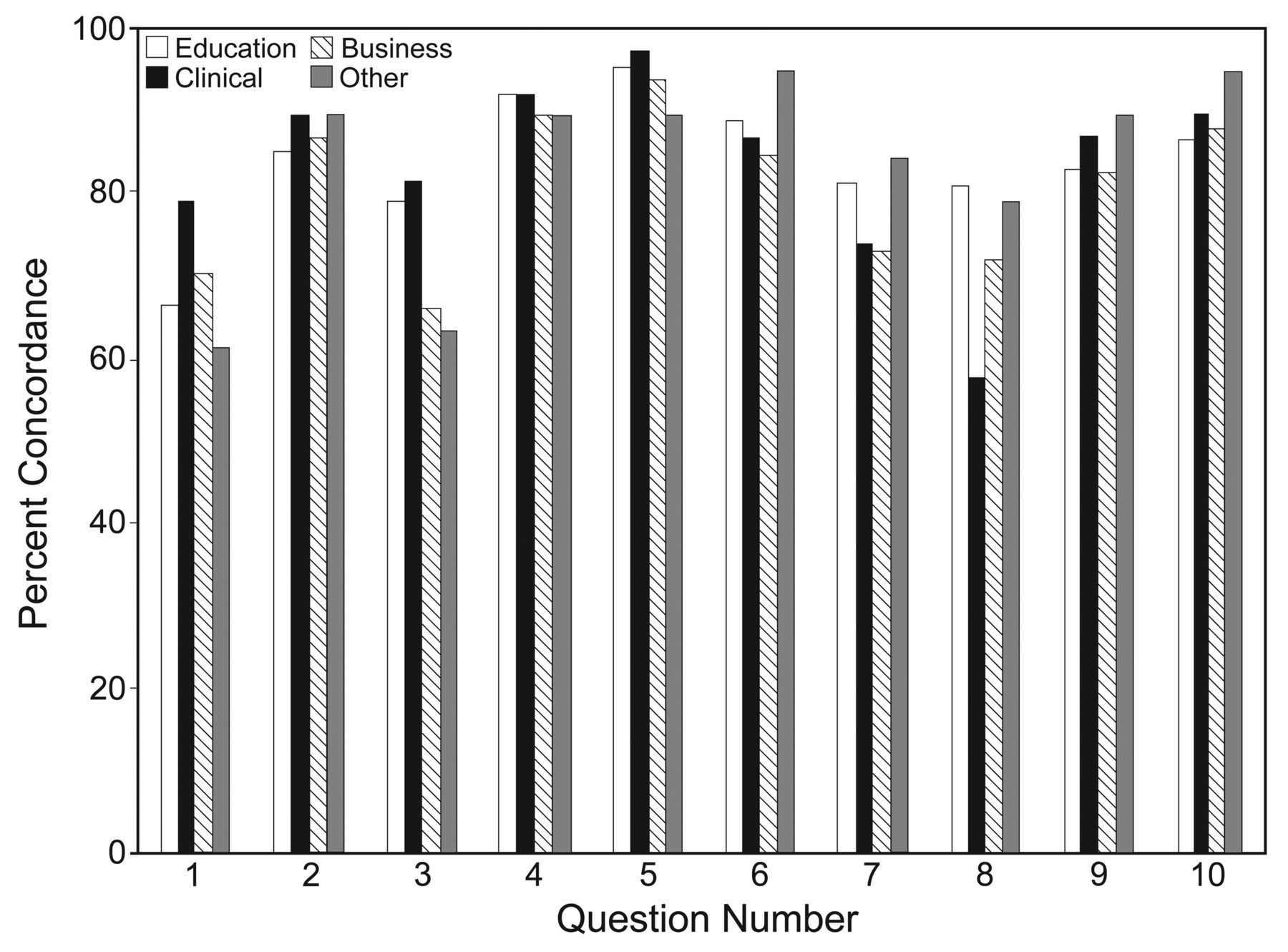
Response to survey questions grouped by professional activity.
Data Analysis for Hypothesis 3
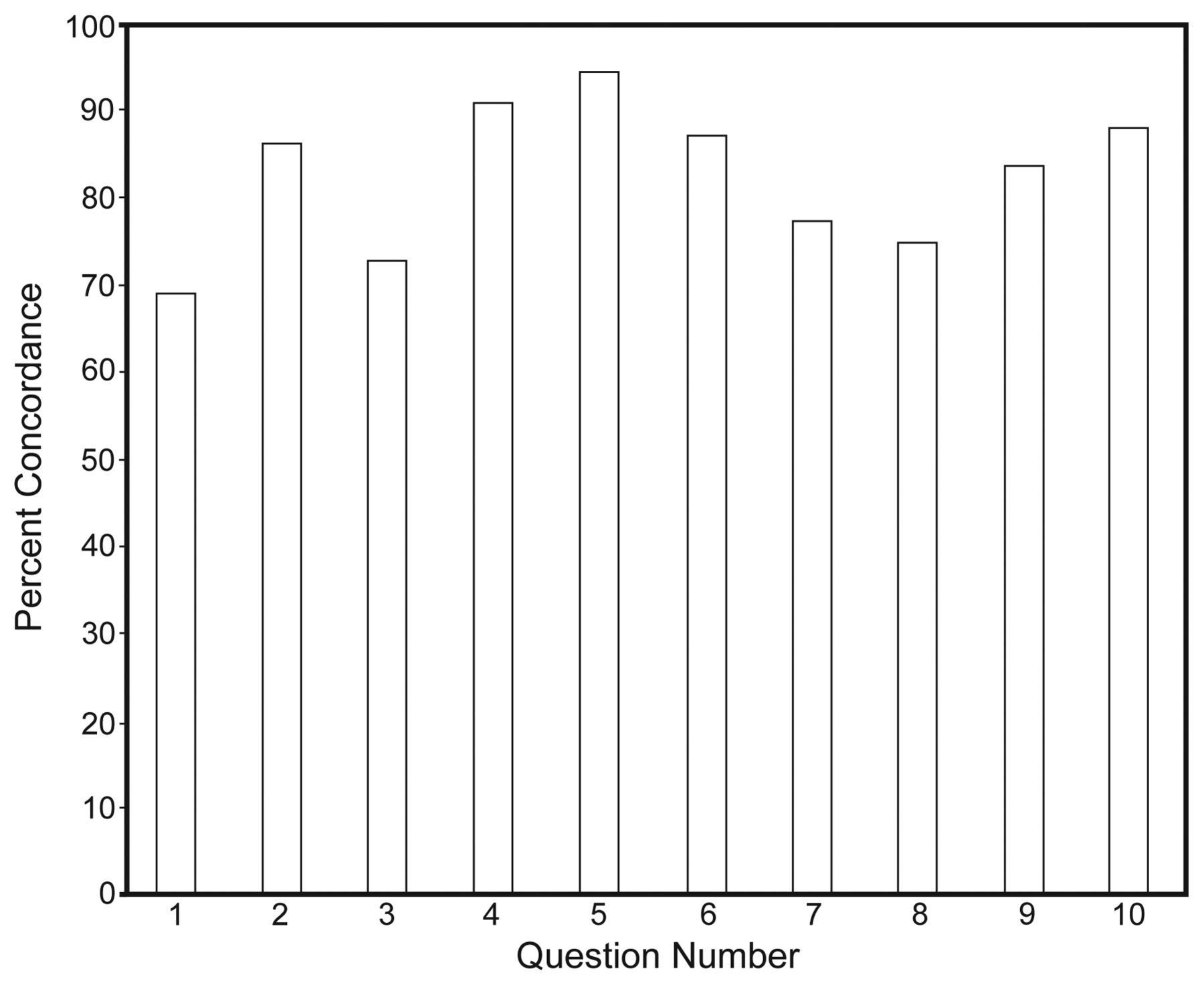
Concordance differed significantly among the survey questions, as shown in Figure 6 (P < .001). Concordance was highest for question 5 (94%) and lowest for question 1 (69%).
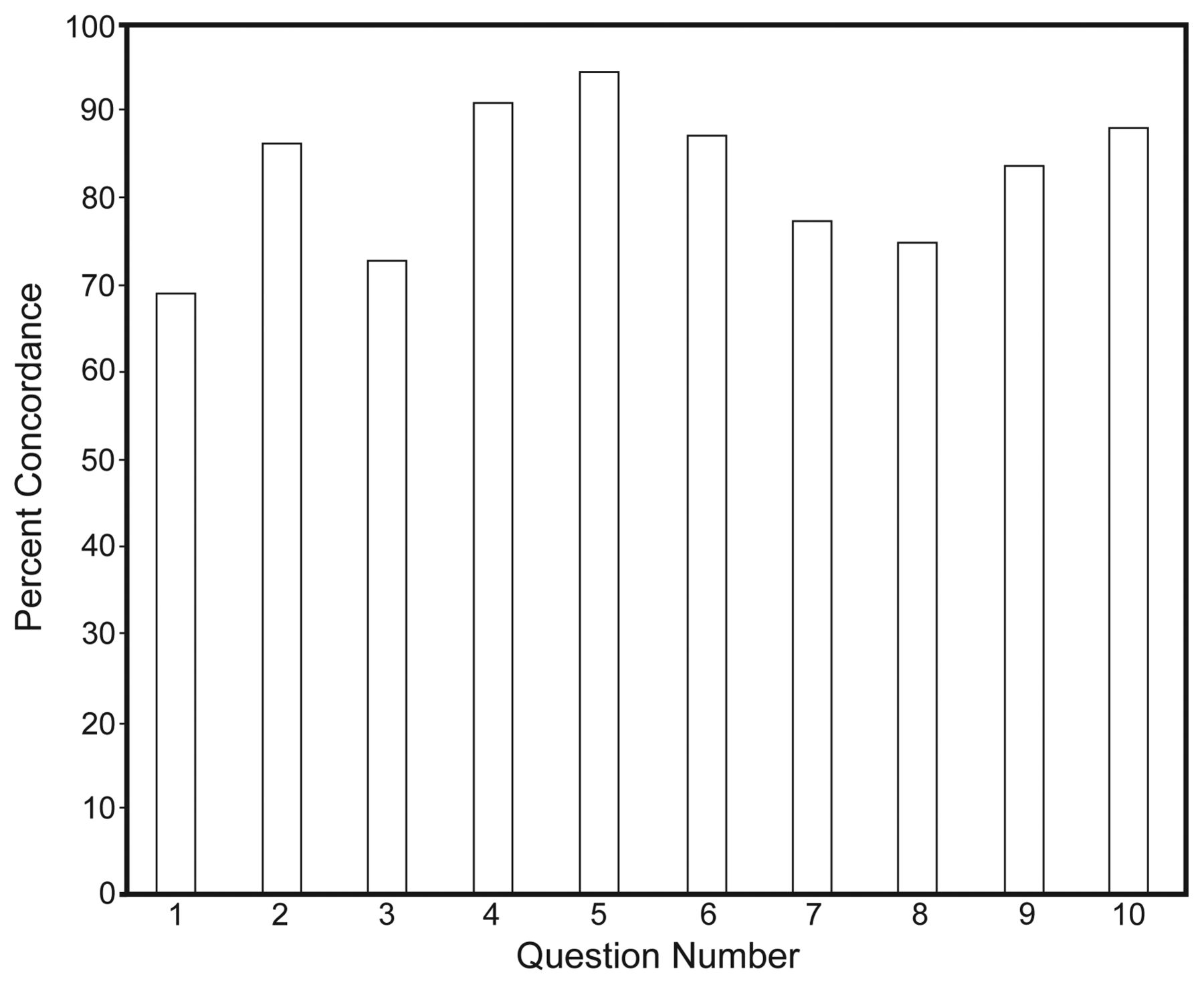
Comparison of concordance among survey questions.
Analysis of Motivation Question
Survey question number 11 was aimed at identifying the motivation for creating a taxonomy of ventilator modes. It was phrased as follows: “The primary goal of a ventilator mode taxonomy is to minimize changes required of manufacturers rather than to improve clinicians' understanding.” This question was included to determine if any bias might exist either for or against manufacturers' interests. The overall response was 86% discordance (ie, strongly disagree or disagree or neutral). At first thought we might interpret this to be due to the overwhelming majority of responders being outside the business arena. However, the respondents who identified themselves as being in the business group responded with 79% discordance. This discordance was demonstrated by all other groups as well: clinicians 84%, educators 88%, and other 100%.
Analysis of Comments
Of the free text comments (question 15) that expressed a bias, 50 were positive and 43 were negative. Representative comments are shown in Table 5. Our favorite positive comment was “Marketing people are going to have a cow over this. They want differentiators, not consensus.” Our favorite negative comment was “I am not sure of the intent of this survey; however, the questions are ambiguous at best, confusing at most, and too wordy. Looks like someone completing a master's or doctoral thesis who has limited experience.” There were 14 comments stating that question 1 was ambiguous or confusing.
Representative Free Text Comments From Survey Question 15
Discussion
Over the last 30 years there has been a rapid evolution of the technologic capabilities of mechanical ventilators. These capabilities have motivated the creation of dozens of names to describe modes of ventilation. This proliferation of names has become counterproductive, making education of end users very difficult and potentially affecting the quality of patient care. Recognizing this dilemma, the International Standards Organization is attempting to create a controlled vocabulary of mechanical ventilation to standardize mode descriptions among manufacturers. That effort has led to the appreciation of the larger need to create a taxonomy, and even an ontology, of mechanical ventilation to support future developments in the semantic web (see the Art and Science of Taxonomy in the online supplemental text). This study was conceived to support such endeavors. Specifically, we sought to determine whether prior publications describing mode terminology and classification were sufficiently disseminated to suggest that an informal consensus currently exists, at least in principle. That consensus was hypothesized to exist among stakeholders in the international respiratory care community, including physicians, nurses, engineers, and manufacturers' representatives working in clinical, educational, and business environments.
This study generated survey results that indicated a significant level of concordance with 10 basic constructs of mechanical ventilation among stakeholders. Not surprisingly, the level of concordance was highest among respiratory therapists, presumably because they are more familiar with the prior art as it was published in journals and textbooks aimed at their profession. Of note was the fact that engineers had the lowest level of agreement with the construct that ventilatory assistance can be achieved “by only 2 means: control of the inspiratory volume/flow waveform, or control of the inspiratory pressure waveform.” Possible explanations for this result include the fact that these engineers were not aware of the construct because it appeared almost exclusively in clinically oriented journals (as opposed to engineering journals) and because engineers typically recoil at the idea of there being “only” a set number of ways to control a system. Hence, the engineers, as well as many others who responded, may not have appreciated the larger context of the survey questions (ie, creating a universal taxonomy) and tended to interpret them within their own narrow perspective.
The fact that there were no differences among responses when grouped according to professional activity is perhaps not surprising. Biases are held by people, not abstract professions. In addition, each professional activity has a mixture of professionals, so any potential differences would tend to be canceled out.
The finding that concordance varied among constructs invites discussion. The least concordant construct was represented by question 1: “A breath is defined as an inspiration paired with an expiration, where the 2 are matched by size or timing, thus allowing small fast breaths on top of large slow breaths during mechanical ventilation.” The comments indicated that the low concordance with this construct was due, in part, to the perceived complexity/ambiguity of the question. Part of the problem is the compound nature of the construct. But simply postulating that a breath is an inspiration paired with an expiration would have been trivial. The issue of matching of size is relevant in the context of some modes that first impose a large machine initiated inspiration, then allow the patient to breathe relatively smaller breaths for a short period, followed by a large machine initiated expiration (eg, airway pressure release ventilation). There is also the alternative possibility that the ventilator imposes small, rapid breaths upon slower, larger, patient initiated breaths (eg, high frequency oscillatory ventilation). Clearly there was no way to explain the full context of the question, yet it had to be asked. Confusion resulted because respondents were not familiar with thinking about the larger context. Nevertheless, if the survey were repeated, this question would have to be better worded.
The question with the second lowest concordance was number 2: “A ventilator can assist a breath by only 2 means: control of the inspiratory volume/flow waveform (ie, volume control), or control of the inspiratory pressure waveform (ie, pressure control).” The lower concordance for this construct may be a direct result of the confusion in the industry about the word “assist.” Some authors and manufacturers have promulgated the notion that any patient-initiated breath is an “assisted” breath. On the contrary, physiologists and physicists tell us that the word assist has nothing to do with what the patient does but rather relies on whether or not the ventilator performs work on the respiratory system. This misunderstanding is tied to a much larger issue affecting the formation of a taxonomy: there is a fundamental disagreement among stakeholders who view the ventilator in terms of how it is used clinically (ie, from the patient's point of view) and those who view it in terms of what it does mechanically (ie, from the operator's point of view). For example, the term “assist/control” has been very popular for decades to name a mode wherein either the patient triggers the breath (assist) or the ventilator triggers the breath (control). Some authors even go so far as to divide ventilatory support into 2 groups: “assisted” modes and “controlled” modes, where “assisted” means “the patient interacts in some way with the ventilator,” and “controlled” means “the machine determines the rate, the inspiratory time, and the tidal volume, so the patient does no work.”9 This viewpoint is anachronistic and dates to decades ago when patient initiation of inspiration was a novelty. And this is fundamentally a patient-centric view, because those who use the term “assist/control” are only interested in whether the ventilator responds to the patient's inspiratory effort or whether the breath is imposed on the patient. From the point of view of creating a taxonomy, the term assist/control is less than useless because it elevates a very low level system feature (the trigger variable) to the most important hierarchical position. Indeed, the terms assist and control as used in this fashion relate to no other constructs in a hierarchical way and are in fact names rather than tags (ie, taxonomic attribute groupings). Worse, they conflict with more important meanings of the word assist and control that do relate to fundamental constructs. Thus, we may conclude that the low concordance with construct number 2 indicates where more education needs to be directed. In fact, we could argue that this particular construct indicates the key issue: getting people to stop thinking in terms of names promulgated by manufacturers and start thinking about general terms of classification (when appropriate of course, as in educational programs and operator manuals).
The construct with the next lowest concordance was associated with question number 8: “Being able to identify any mode as one of these 5 basic ventilatory patterns has little practical value: 1. VC-CMV, 2. VC-IMV, 3. PC-CMV, 4. PC-IMV, 5. PC-CSV. VC = volume control. PC = pressure control.” In order to agree with this construct, the respondent would have to be aware of the expanded definitions of the terms CMV, IMV, and CSV. Despite the fact that question 7 (the next higher concordance level) defined these terms, most people probably have a more restricted understanding of them and associate them with specific mode names on specific ventilators rather than viewing them as more generic categories of mode characteristics. Again, this bias was expected, and, indeed, the fact that the majority of responses were concordant is encouraging.
The application of the 10 constructs described in this study to the development of a formal taxonomy of mechanical ventilation is beyond the scope of this paper. However, the confusion surrounding terms related to modes of ventilation has been acknowledged by the editorial board of Respiratory Care. As a result, the Journal publicly endorsed the adoption of standard vocabulary to describe ventilator modes. Preferred nomenclature and a glossary of terms used to describe ventilator modes (consistent with the constructs described in this study) are included in the guidelines for manuscript preparation and published in the Journal and on its Web site (Table 6).10
Preferred Nomenclature for Mechanical Ventilation for Manuscripts Submitted to Respiratory Care*
Recently, the American Association for Respiratory Care assembled a task force to identify potential new roles and responsibilities for respiratory therapists and to suggest the elements of education, training, and competency-documentation needed to assure safe and effective execution of those roles and responsibilities within the next 5 years and beyond.11 The group identified the important role education and competency assessment in mechanical ventilation will play in our profession's future.12 Education and competency assessment of the modes and principles of invasive and noninvasive mechanical ventilation are being required by physician-based organizations as well. A multi-society task force identified and defined modes and principles of invasive and noninvasive mechanical ventilation as one of the essential competencies to be addressed for internal medicine-based critical care and pulmonary medicine.13
To safely and effectively manage a mechanical ventilator, the respiratory therapist must thoroughly understand ventilator design, classification, and operation in order to properly match ventilator capability with physiologic need. The proliferation of names for modes of ventilation and lack of a standardized nomenclature may contribute to confusion and inappropriate clinical application of ventilatory modes. The effects may impair gas exchange and compromise pulmonary mechanics and patient safety. Lack of understanding of ventilator design can contribute to documentation issues.14 Documentation errors in the medical record increase the propensity of medical decision errors and adverse patient outcomes.15,16
Conclusions
In conclusion, the results of this survey indicate that the respondents were apparently familiar with the previously published literature upon which the survey constructs were based. Furthermore, the degree of familiarity and concordance with these constructs may represent a sufficient basis for attempting to formalize a taxonomy of mechanical ventilation and developing educational materials targeted for key stakeholders.
Footnotes
- Correspondence: Robert L Chatburn MHHS RRT-NPS FAARC, Respiratory Therapy, M-56, The Cleveland Clinic, 9500 Euclid Avenue, Cleveland OH 44195. E-mail: chatbur{at}ccf.org.
Mr Chatburn presented preliminary data from this paper at the the Open Forum of the International Respiratory Congress, December 5-8, 2009, in San Antonio, Texas.
Mr Chatburn has disclosed relationships with Dräger, Hamilton, CareFusion, Covidien, Newport, IngMar, Radiometer America, Breathe Technologies, and the Alpha-1 Antitrypsin Foundation.
The other authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
See the Related Editorial on Page 653
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}