

Introduction
Acute pulmonary edema resulting from a rapidly expanded collapsed lung is termed reexpansion pulmonary edema (RPE). The onset of RPE can occur within less than 1 hour after the removal of air or fluid. Management strategies include oxygen supplementation, diuresis if hemodynamically stable, and ventilatory support in severe cases until the pulmonary edema has resolved.1 We report a case of RPE following video-assisted thoracoscopic surgery (VATS). The computed tomography (CT) findings in this case are unique and to our knowledge are the first to be reported in the medical literature.
Case Summary
A 87-year-old female with a history of breast cancer underwent right-sided VATS, pleural biopsy, and mechanical pleurodesis for evaluation of a large, recurrent pleural effusion (Figs. 1 and 2). During the procedure, 2.1 L of straw-colored fluid were removed. Twelve hours after the procedure the patient's chest radiograph revealed dense right lung consolidation (Fig. 3) with worsening PaO2/FIO2. The patient was noted to have pink frothy sputum production from the endotracheal tube. Vital signs were as follows: temperature 37°C, blood pressure 136/75 mm Hg, heart rate 80 beats/min, respiratory rate 16 breaths/min, and oxygen saturation of 97% with FIO2 of 0.80. The patient was sedated on the ventilator and in no apparent distress. Chest examination revealed rhonchi on the right lung, with clear breath sounds on the left lung. Cardiovascular, neck, abdominal, and extremities examination results were normal. The patient's arterial blood gas results showed pH 7.41, PaCO2 33 mm Hg, PaO2 73 mm Hg on ventilator settings of FIO2 0.80 and PEEP 5 cm H2O. Blood tests showed hemoglobin concentration of 13 g/dL, normal white blood cell and platelet count. Her basic metabolic profile was normal, brain natriuretic peptide was 498 pg/mL (normal < 100 pg/mL), and serum C-reactive protein was 11.3 mg/dL (normal < 0.5 mg/dL). Pleural fluid analysis revealed an exudative effusion, with lactase dehydrogenase concentration of 94 U/L and total protein concentration of 4.1 g/L. Pleural fluid pH was 7.60. Cytology of pleural biopsy was positive for metastatic adenocarcinoma consistent with mammary origin. CT scan of the chest was obtained to further evaluate this consolidation (Fig. 4). The patient also underwent fiberoptic bronchoscopy with normal endobronchial examination. Right mainstem bronchial washings revealed no organisms. The clinical history and presentation of acute, unilateral pulmonary edema with no evidence of infection supported the diagnosis of RPE. Patient management consisted of diuresis and ventilatory support until resolution of right lung pulmonary edema (Fig. 5). The patient was extubated on postoperative day 3. The remainder of her hospital course was uneventful. The patient was discharged home on hospice because of the extent of disease and poor functional status.

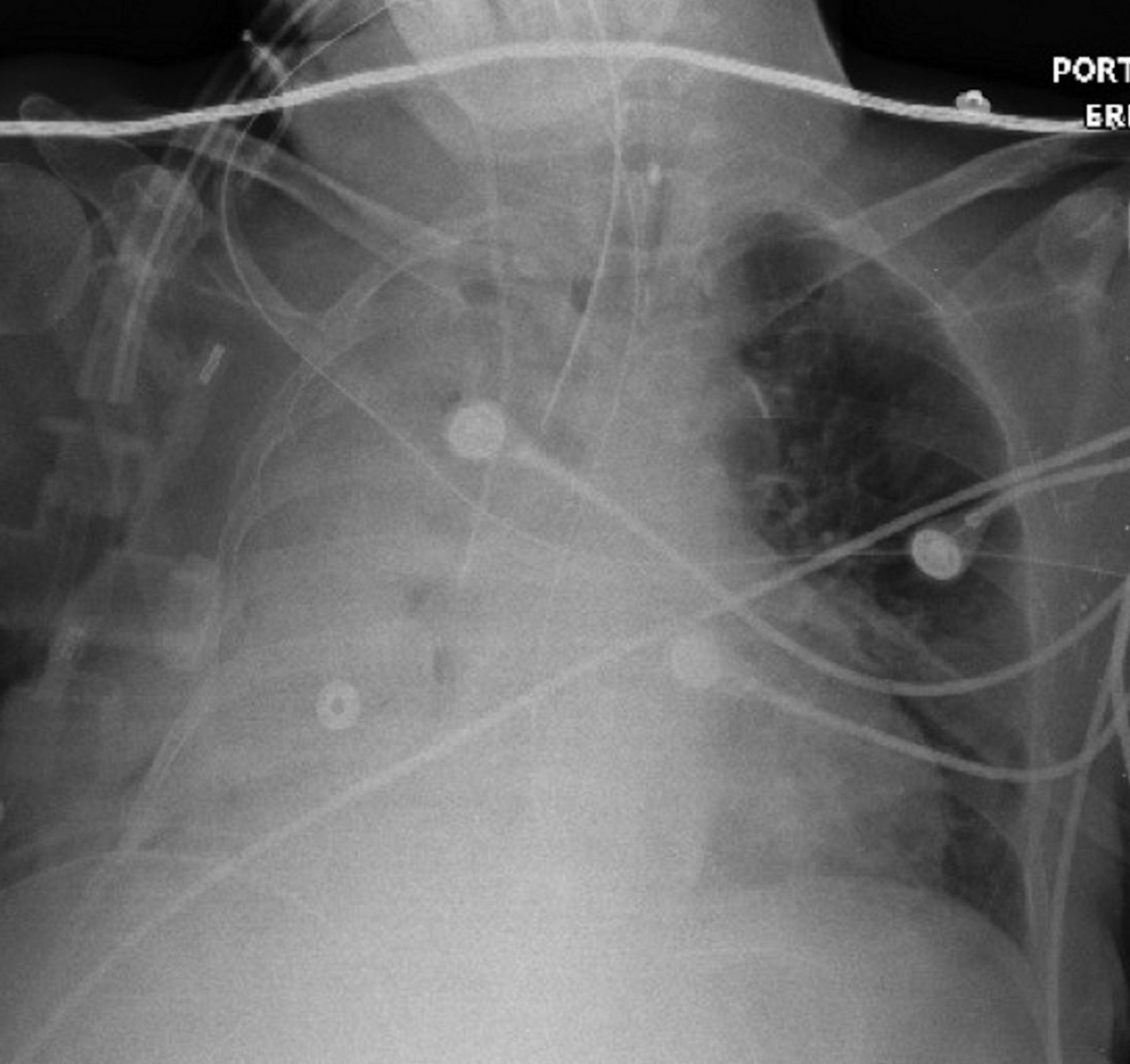
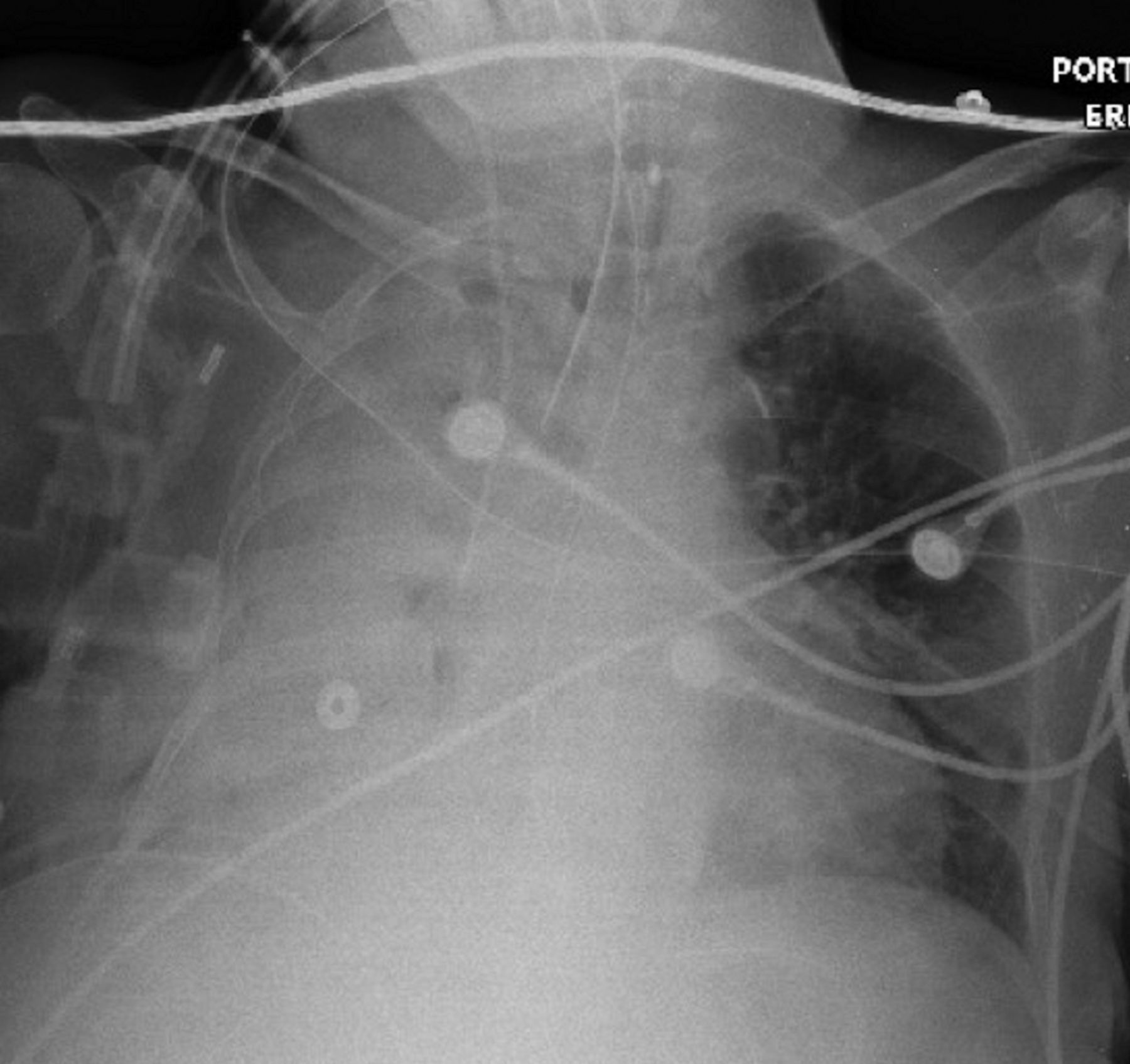
Chest radiograph showing a massive right pleural effusion.

Chest computed tomogram showing large right pleural effusion with entrapped lung.
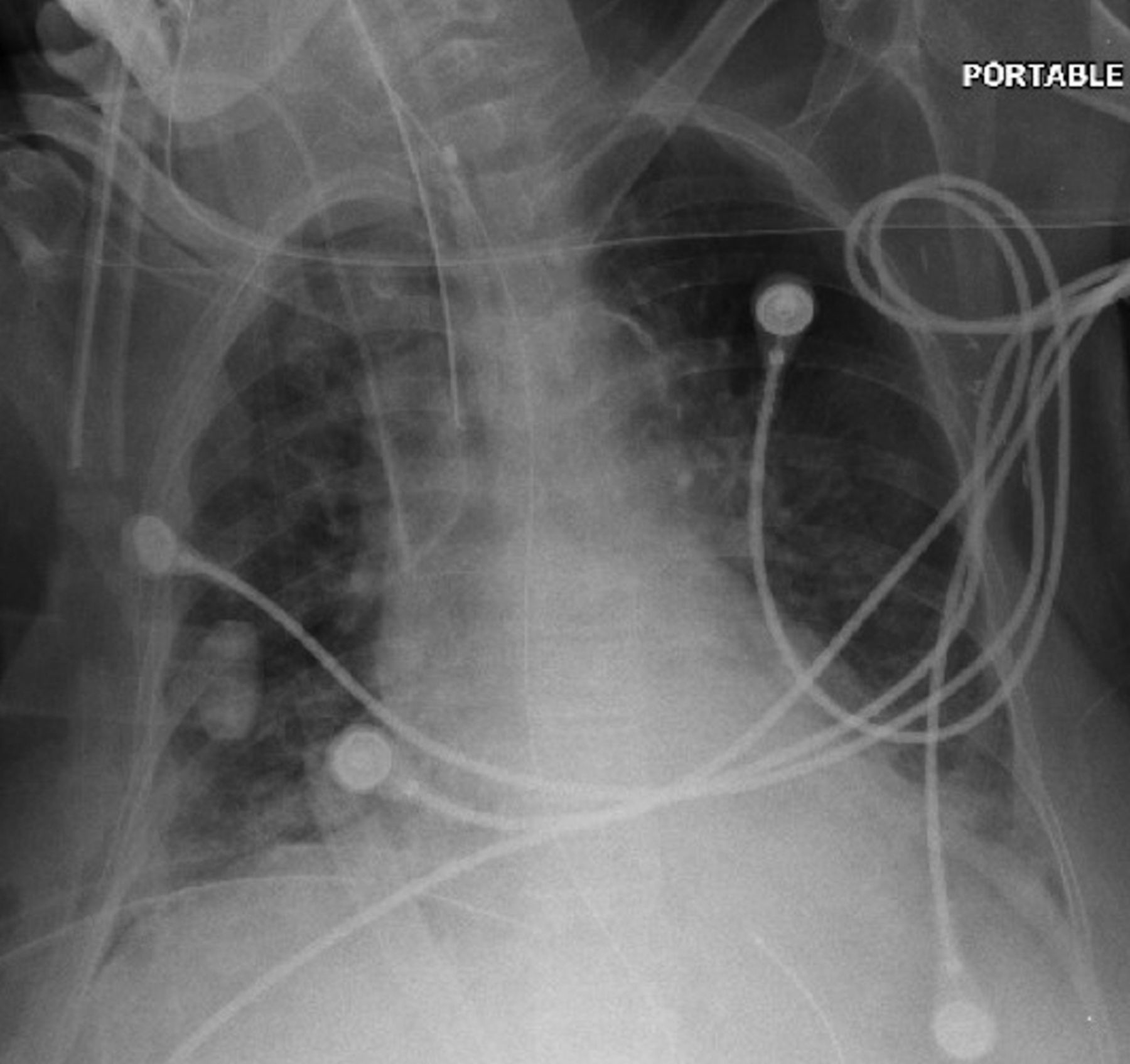
Postoperative day 1 chest radiograph showing dense right consolidation.
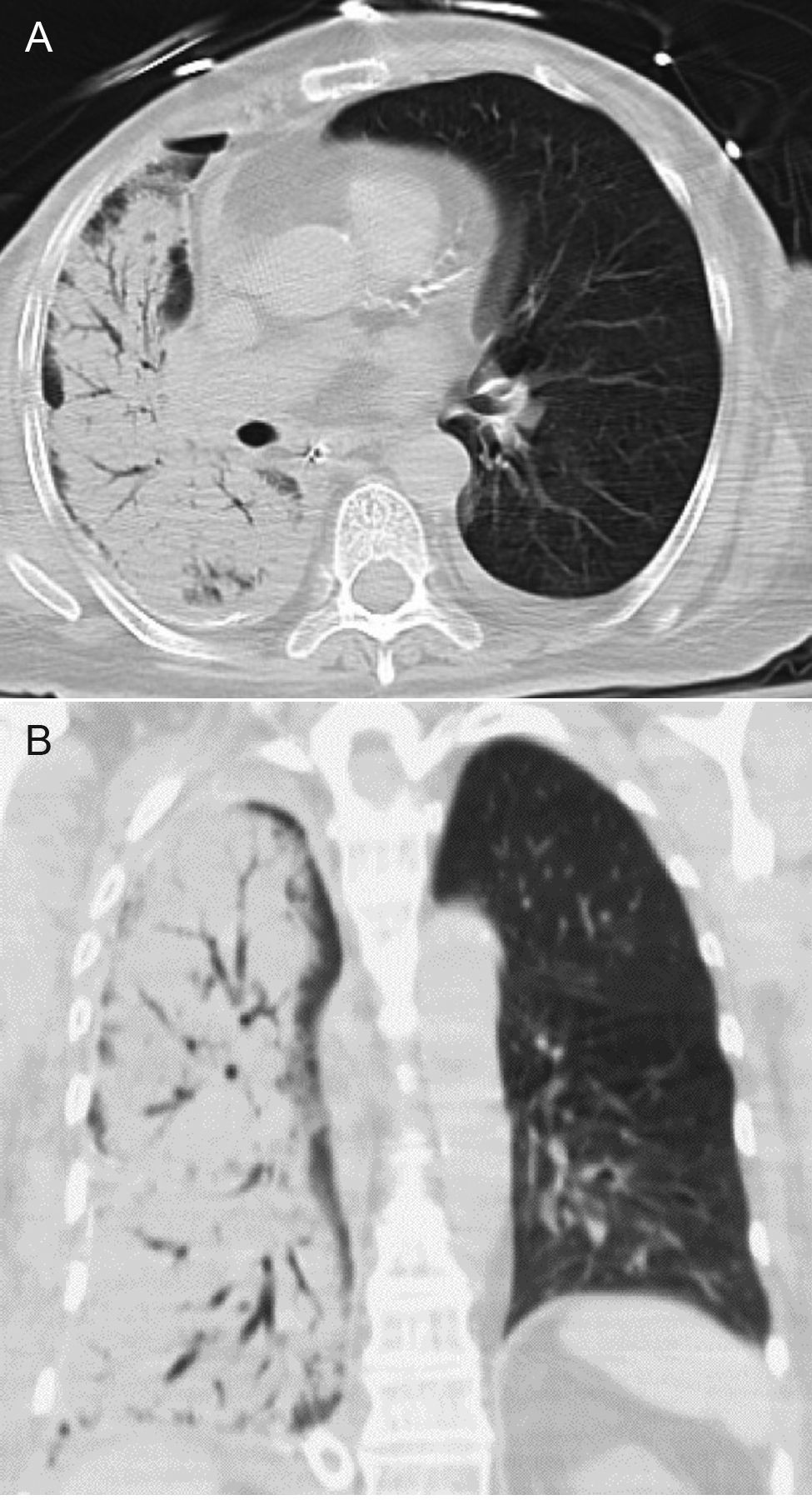
A. Chest computed tomogram showing dense right consolidation with numerous air-bronchograms. B: Chest computed tomogram with coronal views demonstrating diffuse right lung alveolar infiltrate.
Chest radiograph showing resolution of right lung edema.
Discussion
RPE was first described by Pinault in 1853, after the removal of pleural fluid.2 Since then many cases have been reported in the literature, describing reexpansion of the collapsed lung following drainage of fluid or air. The incidence of RPE following pleural effusion or pneumothorax is between 0 and 1%.3 Risk factors for development of RPE include duration of lung collapse > 3 days, removal of over 2,000 mL of fluid, age in the fourth decade of life, and an onset within 24 hours from reexpansion of the collapsed lung.1
The etiology of RPE is not fully appreciated. Current evidence suggests RPE is the result of increased permeability of the pulmonary capillaries due to alterations in lymph flow, protein concentration, and colloid pressure following reexpansion. Koike et al, in their study with 14 unanaesthetized sheep, demonstrated increased caudal mediastinal lymph flow post reexpansion after 24 hours of lung collapse.4 Clinical studies by Buczko et al and Sprung et al measured protein concentration and colloid pressure of airway fluid, and demonstrated an increase in these parameters in RPE.5,6 The combination of mechanical stress of the stretching pulmonary microvasculature, in addition to changes in lymph flow, suggests that the reexpanding lung is vulnerable to capillary leakage, resulting in pulmonary edema.1 The clinical findings of hypoxemia, respiratory distress, pink frothy sputum, and cardiovascular instability can occur within 2 hours after drainage.
CT findings range from ground-glass opacities with septal thickening to consolidation with air bronchograms.7 To date, only 4 cases of RPE after VATS have been reported. None of these cases are supported by CT findings.8–10 In a recent retrospective review by Gleeson et al, CT findings in 22 cases of RPE were analyzed, of which 14 cases were due to drainage of pleural effusion, and 8 after drainage of pneumothorax. In this series, consolidation involving the entire ipsilateral lung was seen in 5/22 (23%) of cases.7 In contrast to our case report, none of the reported cases demonstrated complete consolidation of the ipsilateral lung after a VATS procedure on an entrapped lung.
Treatment is mainly supportive. Management strategies for RPE include oxygen supplementation to maintain adequate tissue oxygenation. Mechanical ventilation may be required in severe cases. Administration of diuretics should be considered in hemodynamically stable patients.1 Negative pressure applied to the pleural space should be stopped in cases where a chest drain is still in place.9 In a recent clinical study, Feller et al showed that large volume thoracentesis could safely be performed as long as end-expiratory pleural pressures remain less than −20 cm H2O.11
Teaching Points
Risk factors for development of RPE include duration of lung collapse > 3 days, removal of over 2,000 mL of fluid, age in the fourth decade of life, and an onset within 24 hours from re-expansion of the collapsed lung.
Current evidence suggests RPE is the result of increased permeability of the pulmonary capillaries due to alterations in lymph flow, protein concentration, and colloid pressure.
Negative pressure applied to the pleural space should be discontinued in cases where a chest drain is still in place.
Management strategies include oxygen supplementation, diuresis if hemodynamically stable, and ventilatory support in severe cases until the pulmonary edema has resolved.
Footnotes
- Correspondence: Joseph Demidovich DO, Division of Pulmonary, Critical Care, and Sleep Medicine, Department of Internal Medicine, School of Osteopathic Medicine, University of Medicine and Dentistry of New Jersey, 42 East Laurel Road, Suite 3100, Stratford NJ 08084. E-mail: demidojs{at}umdnj.edu.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}