

Abstract
Co-existence of catamenial pneumothorax and hemoptysis is rare. We present a case of catamenial pneumothorax due to bilateral pulmonary endometriosis in a 45-year-old woman. The patient presented with a 3-year history of intermittent productive cough with blood-tinged sputum, chronic anemia, loss of appetite, and general weakness associated with menstruation. Three years prior to this presentation the patient had undergone a sigmoidectomy as treatment for endometriosis of the sigmoid colon with bleeding. Chest radiographs and computed tomography (CT) scan revealed multiple nodules in both lung parenchyma and recurrent pneumothorax. CT-guided biopsy revealed chronic inflammation of those pulmonary nodules, and laboratory studies disclosed elevated serum levels of carbohydrate antigen 19–9 (CA 19–9) and CA 125. Thoracoscopic wedge resection of the pulmonary nodules was performed, and histopathological examination of the resected nodules revealed endometriosis. At one-year follow-up there was no evidence of recurrence of gastrointestinal bleeding or pneumothorax.
Introduction
Catamenial pneumothorax was first reported in the 1950s.1–2 Although uterine endometriosis is thought to affect 5–15% of women of reproductive age, it is rare to find endometriosis in the thorax, especially bilaterally.3 Thoracic endometriosis is normally located in the pleural cavity, diaphragm, or peripheral lung. Clinically, it often presents with pneumothorax or hemothorax. Thoracic endometriosis combined with pneumothorax and hemoptysis is very rare, and only a few cases have been reported.4–6 The mechanisms governing thoracic endometriosis are not well understood, and different theories have been proposed. Herein we report a case of thoracic endometriosis manifesting as multiple pulmonary nodules in a patient with a history of endometriosis in the sigmoid colon.
Case Report
A 45-year-old woman presented with a 3-year history of intermittent productive cough with blood-tinged sputum, chronic anemia, loss of appetite, and general weakness associated with menstruation. Three years prior to this presentation a colonoscopy examination revealed a bleeding ulcerated polyp arising from the sigmoid colon (Fig. 1) Laparoscopic resection of the sigmoid colon was performed, and histologic examination of the resected specimen revealed endometriosis. The patient had experienced several episodes of pneumothorax during the past 2 years.

Colon fibroscopy shows an ulcerative polyp in the sigmoid colon.
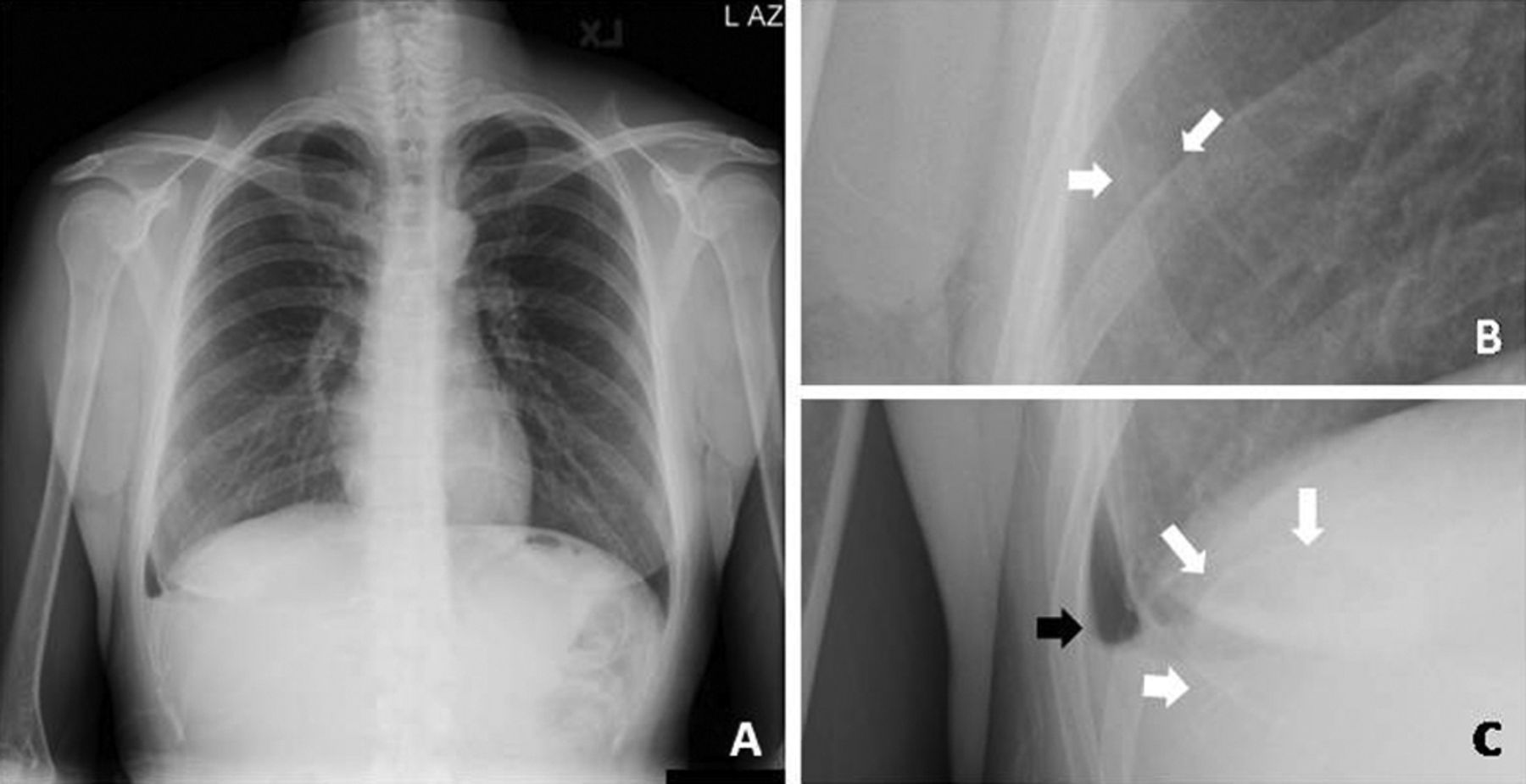
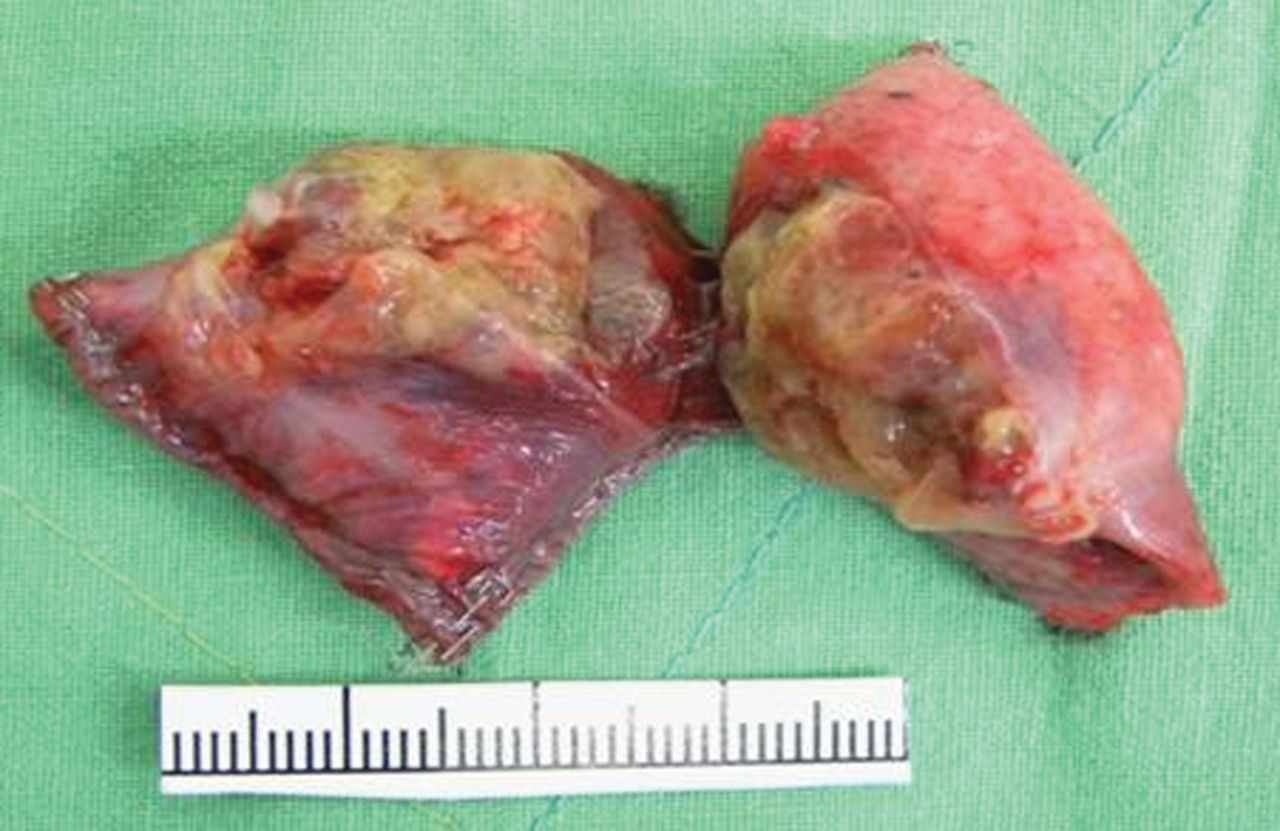
A chest radiograph (Fig. 2) and computer tomography (CT) scan (Fig. 3) showed multiple cystic shadows, nodules, and right minimal pneumothorax with pleural effusion. Several small round nodules were located in the lung parenchyma, and cystic lesions with consolidation were noted in bilateral lower lung fields behind the diaphragm. A CT-guided biopsy of the pulmonary nodules revealed chronic inflammation. Laboratory studies disclosed the following values: serum carcinoembryonic antigen 0.97 ng/mL (reference value < 3.0 ng/mL), carbohydrate antigen 19–9 (CA 19–9) 256.5 U/mL (reference value < 40 U/mL), and carbohydrate antigen 125 (CA 125), 188.5 U/mL (reference value < 35 U/mL). Thoracoscopic wedge resection of the pulmonary lesions was performed because the possibility of malignancy could not be ruled out (Fig. 4). During the operation we noticed that the parietal pleura and diaphragm were intact. The lesions had a hypervascular appearance, were violet in color, and bled easily on palpation. After resection the color of the nodules changed from violet to yellow. Histologic examination of the resected specimens revealed pulmonary endometriomsis (Fig. 5).

Chest plain film. A: Multiple cystic shadows, nodules, and right minimal pneumothorax with pleural effusion. B: A 0.8-cm round nodule located in the right middle lung field (white arrows). C: A 3.5-cm cystic lesion with consolidation in the right lower lung field behind the diaphragm (white arrows), and a right side minimal pneumothorax with pleural effusion (black arrow).

Computed tomogram of the thorax shows left side pneumothorax and multiple cavity-like lesions with consolidation in the bilateral lungs.

Thoracoscopic wedge resection of the right lower lobe of the lung.

Gross pathological specimen of the nodule.
Microscopically, numerous endometrial glands and stroma formed a relatively well circumscribed lesion in the lung parenchyma (Fig. 6A and 6B). The endometrial glands were characterized by the presence of ciliated cells with a cuboid morphology and decidual-like stroma. Immunohistochemical staining for CD10 revealed positive staining in the stromal cells (see Fig. 6C and 6D). Micrographs demonstrating the histological appearance of the sigmoid colon that had been resected 3 years earlier showed evidence of intramucosal endometriosis, characterized by a lack of mucin-producing goblet cells in the endometrial glandular lining cells, and atrophic endometriotic glands lined by flat to cuboid cells with focal ciliation (see Fig. 6E and 6F) Immunophenotyping of positive cytokeratin 7, lack of luminal carcinoembryonic antigen, and negative cytokeratin 20 staining support the finding that the atrophic glands were of endometrial origin (Fig. 6G, 6H, and 6I) At one-year follow-up there was no evidence of recurrence of gastrointestinal bleeding or pneumothorax.

A: Low power view (40×) of endometriosis in lung. Numerous endometrial glands and stroma form a relatively well circumscribed lesion in the lung parenchyma. B: High power view (400×) shows the details of the endometrial gland, with cuboid, ciliated, lined cells, and decidual-like stroma (C and D). E: Low power view (40×) of CD10 immunostaining in stromal cells of intramucosal endometriosis in the sigmoid colon of the same patient. Note the lack of mucin-producing goblet cells in the endometrial glandular lining cells. F: High power view (400×) of CD10 immunostaining in stromal cells exhibits an atrophic endometriotic gland lined by flat to cuboid cells, with focal ciliation, compared to adjacent colonic glands, no goblet cells are noted. G, H, and I: Immunophenotyping of positive cytokeratin 7, lack of luminal carcinoembryonic antigen, and negative cytokeratin 20 staining supports the atrophic gland to be of endometrial origin (40×).
Discussion
Thoracic endometriosis syndrome includes 4 well recognized clinical entities, namely, catamenial pneumothorax, catamenial hemothorax, catamenial hemoptysis, and lung nodules. Thoracic endometriosis manifests as catamenial pneumothorax in about 73% of patients. Catamenial hemothorax and pulmonary nodules are less common manifestations, and occur in about 14% and 6% of patients, respectively.1 The etiological mechanisms governing catamenial pneumothorax are not well understood, and 4 theories have been proposed:
It can be caused by spontaneous rupture of blebs, in a manner similar to spontaneous pneumothorax.
The condition can be caused by sloughing of endometrial implants from visceral pleura, leading to alveolar damage and subsequent pneumothorax.
Increased secretion of prostaglandin-Fα from endometrial tissue during menses can cause constriction of vessels in the terminal airway, resulting in pneumothorax.
Pneumothorax can be caused by air that has entered the peritoneum through the genital tract during menstruation, which then passes through congenital perforations in the diaphragm.4
Three theories have been proposed to explain the presence of intrathoracic endometrial implants: coelomic metaplasia; lymphatic or hematogenous embolization from the uterus or pelvis; and retrograde menstruation with subsequent transperitoneal-transdiaphragmatic migration of endometrial tissue.4 Peritoneal fluid circulates in a clockwise direction and finally passes through the right side of the diaphragm.7 This might explain why there is a right side predominance of pleural endometriosis. In our patient, both the lung and colon were involved. There was no evidence of diaphragmatic defects or endometrial implants in the pleural cavity. In addition, the majority of the lesions were located in the lower lung field, and all of the lesions in that field were larger than those in the upper lung field. We believe that the only way to explain the source of endometriosis in this patient is hematogenous embolization of endometrial tissue.
Studies have shown that increased levels of CA 125 and CA 19–9 are useful in diagnosis of endometriosis.8,9 In our patient, the levels of both markers were elevated.
Thoracic endometriosis syndrome normally occurs in women between the ages of 25 and 35 years.1 Management of thoracic endometriosis includes observation, hormone therapy with GnRH agonists, and surgical treatment.10 In the case reported herein, pulmonary lesions were removed by thoracoscopic surgery because the possibility of malignancy could not be ruled out. We did not employ preoperative CT-guided marking because the pulmonary lesions were peripheral.
Diaphragmatic defects, apical bulla or blebs, and nodules are the most frequent findings during surgical procedures. The size of endometrial implants can range from several micrometers to as large as 1 cm, and the color of the nodules can range from brown to violet, according to the period of the menstrual cycle.4 In our patient the thoracic cavity was examined in detail during the thorascopic surgery, and there was no evidence of endometrial implants in the parietal or visceral pleura. We believed that removal of the pulmonary lesions would be sufficient. In fact, at one-year follow-up there was no radiographic evidence of recurrence.
Endometriosis in the lumen of the sigmoid colon is also rare. Most cases of intestinal endometriosis are due to direct implantation of endometrial tissue from the adventitia,11 and segmental resection of the affected region of the small intestine or colon using minimally invasive surgery is recommended.12 In our patient, laparoscopic resection of the sigmoid colon was performed. Follow-up colonoscopy performed 3 years after surgery showed no recurrence.
The development of pulmonary endometriosis following successful treatment of intestinal endometriosis is rare. This condition can be adequately managed using a minimally invasive surgical approach. When dealing with spontaneous pneumothorax in a productive female with pulmonary nodules, catamenial pneumothorax should be always kept in mind. Pulmonary endometriosis is a differential diagnosis. The tumor markers CA 125 and CA 19–9 can aid the clinician in establishing a diagnosis of thoracic endometriosis.
Footnotes
- Correspondence: William Tzu-Liang Chen MD, Department of Surgery, China Medical University Hospital, China Medical University, 2 Yude Road, Taichung, 404 Taiwan. E-mail: wtchen{at}mail.cmuh.org.tw.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}