

Introduction
Difficult intubation can be found in 11% of emergency tracheal intubations.1 Predictors of difficult tracheal intubation have been described, such as mouth opening, Mallampati classification, atlanto-occipital joint extension, mandibulohyoid distance, inter-incisor distance, thyromental distance, sternomental distance, obesity, and a previous history of difficult intubation.2 The occurrence of difficult intubation is associated with morbidity and mortality.1 Here we present an elderly obese patient who developed massive subcutaneous and mediastinal emphysema after difficult emergency intubation.
Case Summary
An 82-year-old woman presented at the emergency department of a suburban hospital with alteration of consciousness, which was proved later to be due to cerebrovascular accident. She had a history of hypertension and dyslipidemia. Her body weight and height were 63 kg and 125 cm, resulting in a body mass index 40.3 kg/m2. At presentation the physician decided to insert an endotracheal tube (ETT) to protect the airway, on account of her unconscious state. Multiple attempts of intubation using a 7.5-mm diameter single lumen tube were performed before successful intubation. She was then transferred to the ICU and put on a mechanical ventilator for respiratory support. Six hours after intubation, subcutaneous emphysema was recognized over her chest, neck, and face. A chest radiograph was obtained and revealed subcutaneous and mediastinal emphysema. The operation of right thoracostomy intubation and subxiphoid pericardial window was performed; however, there was no improvement in the subcutaneous emphysema. The patient was then referred to our hospital for evaluation and further management of progressive subcutaneous emphysema.
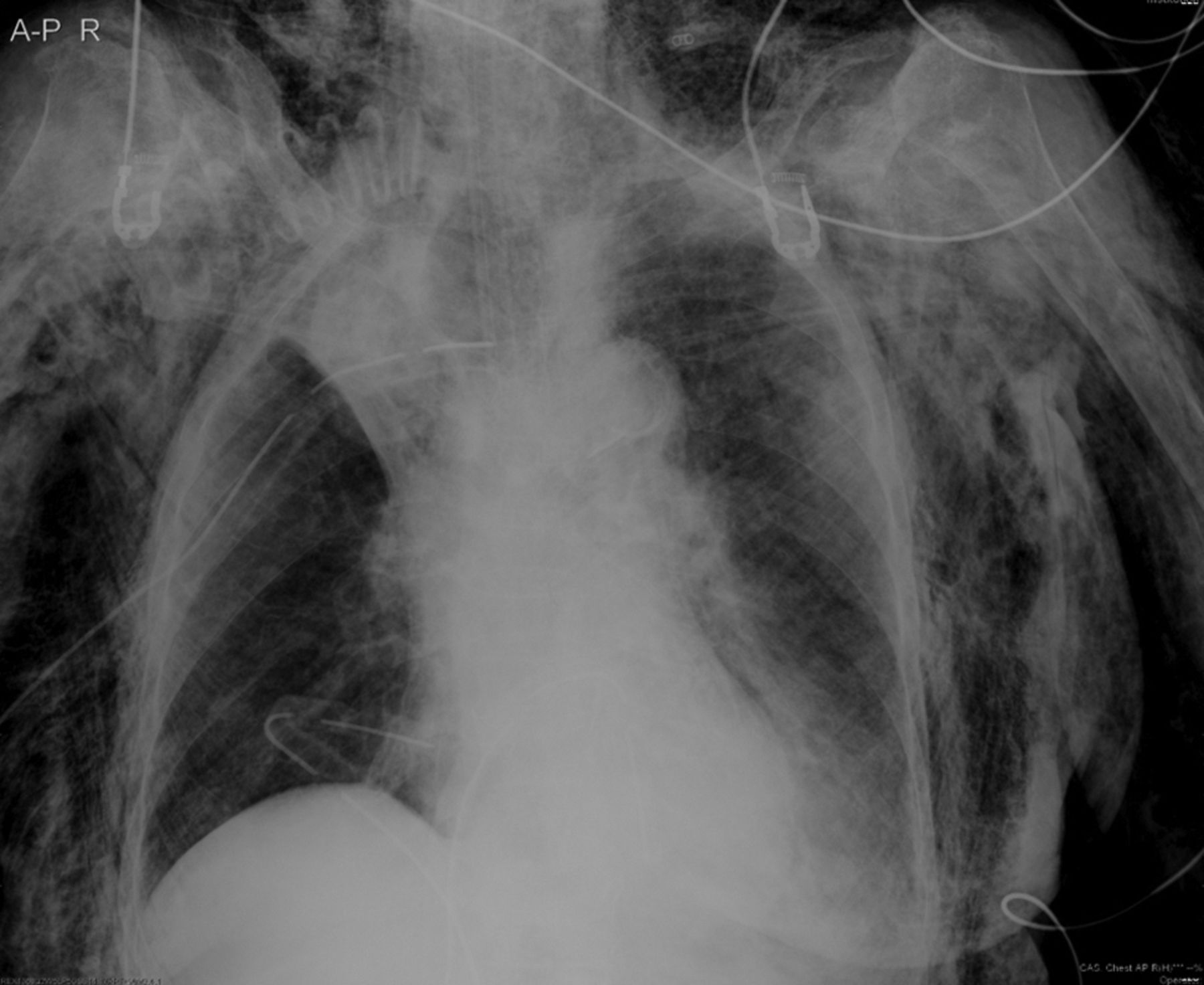
At our hospital the patient was continuously ventilated with a mechanical ventilator in pressure control mode at PEEP of 5 cm H2O. Her vital signs showed blood pressure 90/60 mm Hg, pulse rate 120 beats/min, body temperature 35.8°C, respiratory rate 32 breaths/min, and SpO2 of 100% with 100% oxygen supplementation. Physical examination revealed massive subcutaneous emphysema throughout the whole body. The follow-up chest radiograph is shown in Figure 1.
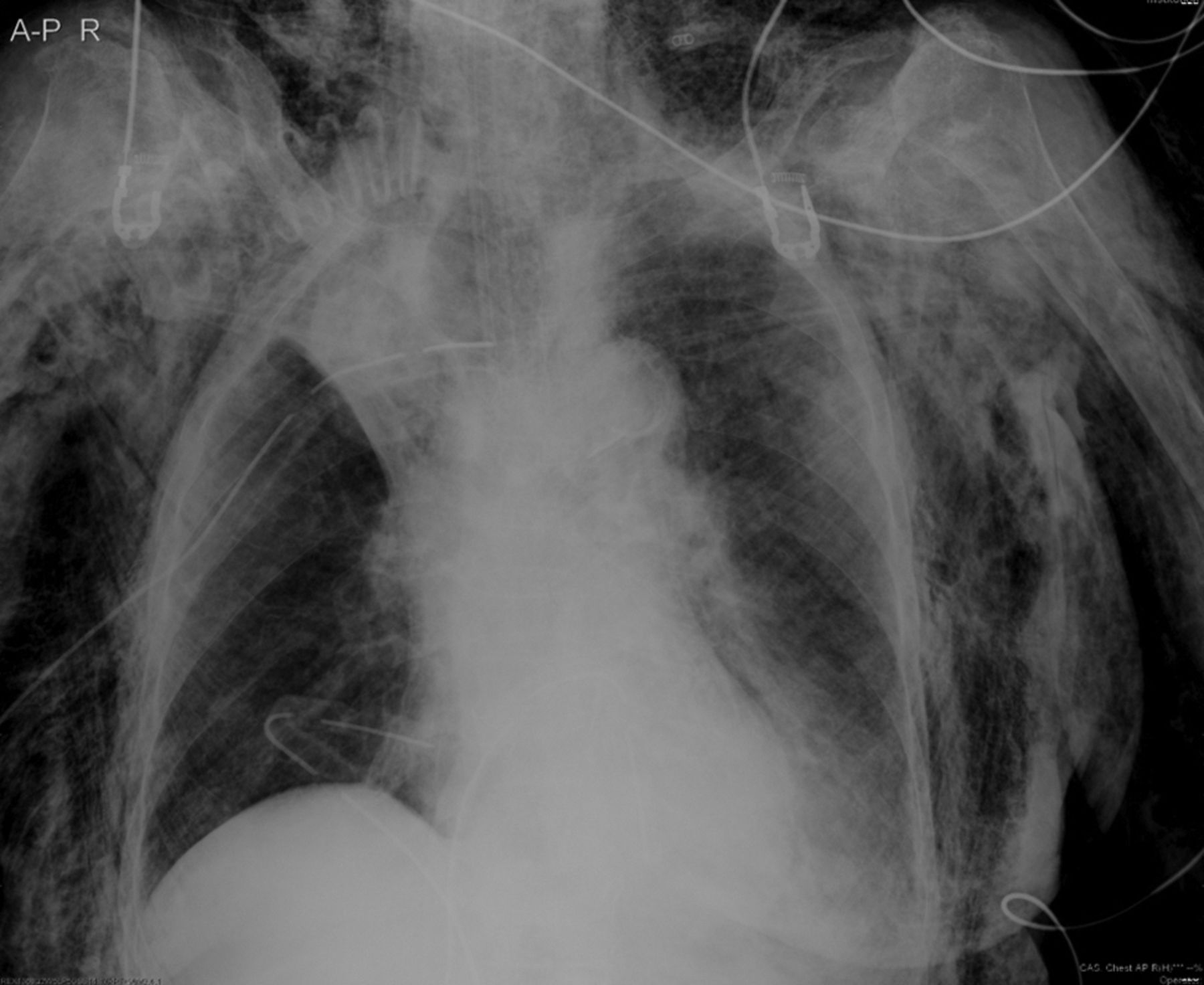
Chest radiograph at admission reveals subcutaneous and mediastinal emphysema, overdistention of the balloon cuff, and distal extension of the balloon toward the endotracheal tube tip.
In addition to subcutaneous and mediastinal emphysema, chest radiograph also displayed overdistention of the balloon cuff and distal extension of the balloon toward the ETT tip. These findings raised the suspicion of tracheal rupture, which was proved by computed tomography (CT) scan of the chest, demonstrating a large defect along the posterior tracheal membrane (Fig. 2A). Bronchoscopy was subsequently performed under general anesthesia and confirmed a large rupture of the posterior membranous wall at the mid to lower trachea (5.0 cm in length, and the intact trachea of 2.8 cm above the carina) (see Fig. 2B).
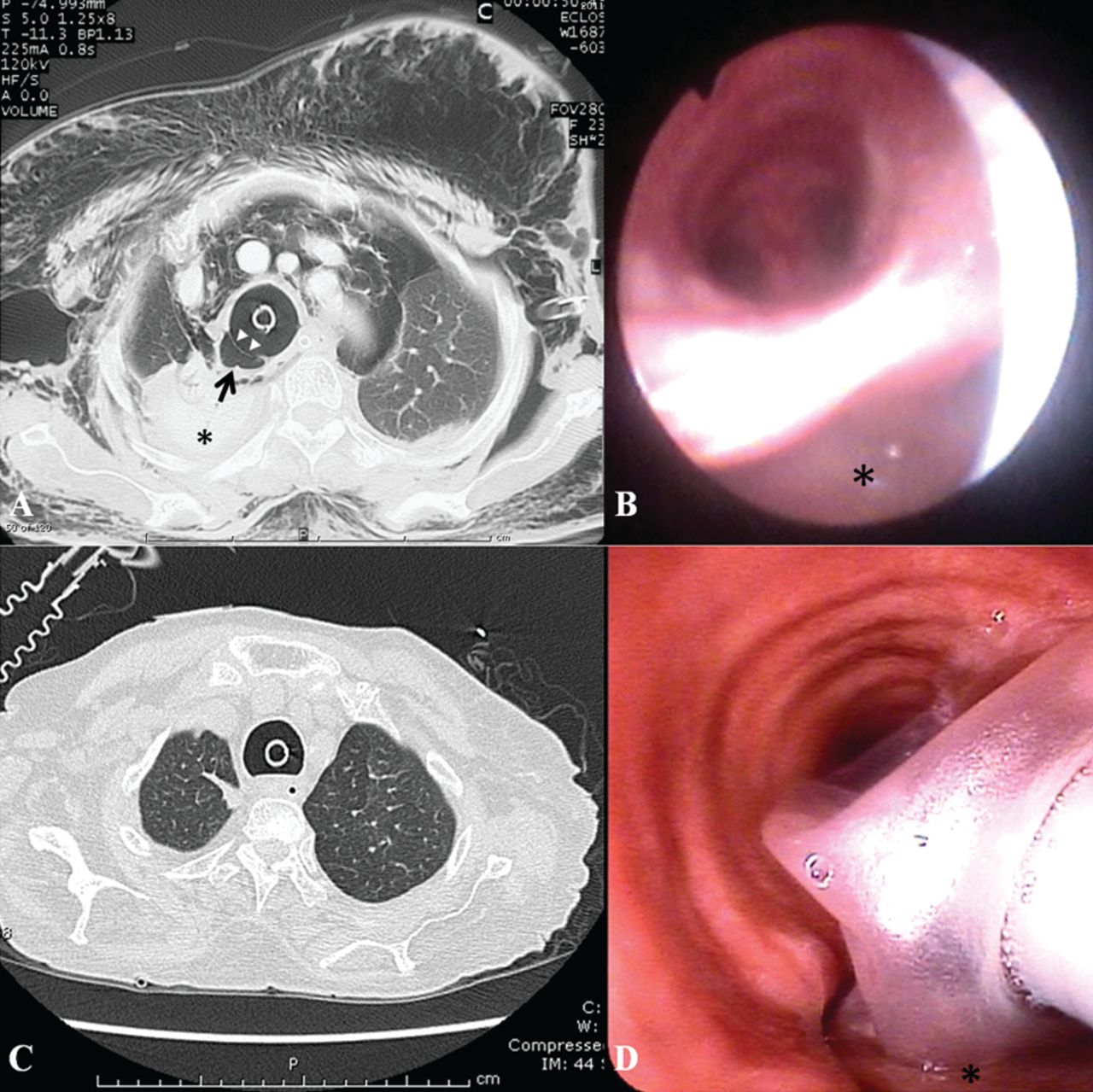
A: Axial chest computed tomogram (CT) image with lung-window setting reveals overdistention of the endotracheal tube (arrow head) and a large defect of the membranous part of the trachea (arrow) with air tracking into the mediastinum, causing mediastinal and subcutaneous emphysema. A collapsed right upper lobe (*) is also noted. B: Bronchoscopy shows a large laceration and a false tract (*) in the posterior tracheal wall (picture was taken at 4 cm above the carina). C: A follow-up axial CT scan on day 22 at the same level as Figure 2A shows improvement of the ruptured site, with complete resolution of the mediastinal and subcutaneous emphysema. Re-expansion of the right upper lobe is shown. D: A follow-up bronchoscopy on day 20, after deflating the cuff, shows healing of the ruptured site (*) (picture was taken at 4.5 cm above the carina).
After discussion with the patient's relatives about the risk of surgical repair and the prognosis of neurological condition, conservative treatment was considered. Tracheostomy was performed using an 8-mm cuffed adjustable flange tracheostomy tube (Portex, Keene, New Hampshire). The distal end of the tube was placed as distally as possible to the rupture site, under bronchoscopic guidance. She was continually on a mechanical ventilator and started on empiric antibiotics with piperacillin/tazobactam. One week after admission, subcutaneous emphysema significantly decreased, so thoracostomy tube and subxiphoid drainage were finally removed. Repeated bronchoscopy on day 20 post-admission revealed healing of the rupture site, and CT scan on day 22 also confirmed this successful conservative treatment (see Fig. 2C and 2D). The patient was taken off the mechanical ventilator on day 22. However, tracheostomy remained in place as a consequence of her depressed level of consciousness, resulting in problems of secretion clearance and upper airway protection. Finally, she was transferred back to the primary care hospital for long-term care.
Discussion
The differential diagnoses of subcutaneous emphysema following intubation are summarized3–7 in the Table. However, the trachea is the most common site of injury. Chest radiograph can render some clues to raise the suspicion of tracheal rupture: deviation of the tip of the ETT to the right, overdistention of the balloon cuff, and balloon migration toward the ETT tip.8 When tracheal rupture is suspected, further investigations should be promptly carried out to establish the definite diagnosis.
Differential Diagnoses of Post-Intubation Subcutaneous Emphysema
Chest CT scan has a sensitivity of 85% for the diagnosis of tracheal rupture.9 Specific CT findings include overdistention of the ETT balloon or herniation of the deformed ETT balloon beyond the trachea, the extraluminal position of the ETT, a focal tracheal wall defect or discontinuity, and a contour deformity or fracture of the trachea.9 Bronchoscopy is the gold standard to establish the correct diagnosis, as it can provide details of location and extension of the lesion. Besides, it helps to place the proper position of the ETT as well as follow-up wound healing.10
Theoretically, surgical management is the treatment of choice for post-intubation tracheal rupture. However, case reports, case series, and meta-analysis over the last decade have demonstrated a high success rate of nonoperative treatment, especially in patients requiring positive-pressure ventilation.10 Consequently, nonoperative treatment is suggested in patients having superficial and short tracheal tears (< 4 cm in length), stable emphysema, and no evidence of sepsis. Nevertheless, successful conservative treatment in a large tracheal tear has been reported.11,12 Mullan et al have suggested that the length of intact trachea > 3 cm above the carina is the important predictor of successful conservative treatment.12 Since ETT or tracheostomy tube is needed while applying positive-pressure ventilation, there should be enough space to place the tube and inflate the cuff, with or without minimal further injury to the lesion, and to keep the lesion under zero pressure. It is reasonable to use an adjustable flange tracheostomy tube in case of having intact trachea > 3 cm above the carina, in view of the fact that it is approximately 3 cm in length from the balloon of the tube to its tip. If there is not enough space, such as with a lesion involving the lower trachea, carina, or proximal main bronchus, selective bilateral mainstem bronchial intubation should be considered.11
In this case we preferred conservative management because of the patient's substantial comorbidities. Although the intact length of the lesion to the carina was < 3 cm, an adjustable flange tracheotomy tube was applied because of lack of experience in bilateral bronchial intubation in our institute. In addition to upper airway management, lower airway pressure strategy, broad spectrum antibiotics to prevent mediastinitis, cough suppressant, and chest tube decompression were also provided.10 Finally, we achieved a favorable result.
In conclusion, we demonstrated a case of subcutaneous emphysema due to tracheal rupture following difficult intubation. Since tracheal rupture is associated with high morbidity and mortality, physicians should have an in-depth knowledge of radiographic signs, diagnostic methods, and treatments of this condition.
Teaching Points
Mouth opening, Mallampati classification, atlanto-occipital joint extension, mandibulohyoid distance, inter-incisor distance, thyromental distance, sternomental distance, obesity, and a previous history of difficult intubation are predictors of difficult endotracheal intubation.
There are some clues on chest radiographs raising the suspicion of tracheal rupture: deviation of the tip of ETT to the right, overdistention of balloon cuff, and balloon migration toward the ETT tip.
Chest CT scan can provide specific findings of tracheal rupture, including overdistention of the ETT balloon or herniation of the deformed ETT balloon beyond the trachea, the extraluminal position of the ETT, a focal tracheal wall defect or discontinuity, and a contour deformity or fracture of the trachea.
Bronchoscopy is the gold standard to establish the diagnosis, and renders invaluable information for planning treatment and follow-up, as it provides details of location and extension of the lesion, guiding a proper position to place an ETT as well as evaluating wound healing.
Nonoperative treatment might be considered in cases of superficial and short length of tracheal tear (< 4 cm.), intact tracheal length above carinal angle > 3 cm, stable emphysema, and no clinical signs of sepsis. If lesions attack the proximal main bronchi or carina, or are < 3 cm above the carina, selective bilateral mainstem bronchial intubation should be considered.
Footnotes
- Correspondence: Viboon Boonsarngsuk MD, Division of Pulmonary and Critical Care Medicine, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand, E-mail address: bss-vb{at}hotmail.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}