

Abstract
BACKGROUND: Dynamic hyperinflation (DH) and exercise limitation develop in patients with COPD; however, there is lack of knowledge about their long-term clinical consequences. We aimed to assess the impact of DH and exercise capacity in predicting mortality and also morbidity, as evaluated by emergency visits and hospital admissions in COPD patients during a 4-year period.
METHODS: We recruited 73 stable COPD patients. The relationships of different respiratory parameters (FEV1%, body mass index, 6 min walk test distance [6MWD], static hyperinflation as measured by the ratio of inspiratory capacity to total lung capacity (IC/TLC) at rest, DH as measured by the change between the post- and pre-exercise values of IC/TLC [ΔIC/TLC], PaO2, and PaCO2) with emergency visits and hospital admissions because of exacerbations and also with respiratory and all-cause mortality were assessed.
RESULTS: The median follow-up period was 47 months (IQR 45–48 months, n = 73). During the follow-up there were 8 (11%) deaths. The ΔIC/TLC value was 3.9 ± 4.6%. The Kaplan-Meier survival curve showed that the cumulative survival rate was significantly lower in the patients with ΔIC/TLC > 4 and with 6MWD ≤ 439.56 m, using these values as thresholds. (The rates for sensitivity were 100% and 87.5%, and for specificity were 56.92% and 87.69%, respectively). The Cox proportional hazards model showed that DH (hazard ratio = 1.4, 95% CI = 1.09–1.84, P = .009) and 6MWD (hazard ratio = 0.98, 95% CI = 0.97–0.99, P = .006) were independent predictors of all-cause and respiratory mortality. 6MWD, FEV1%, IC/TLC, and ΔIC/TLC were found to be significantly related to emergency visits (r = −0.28, r = −0.41, r = −0.24, and r = 0.38, respectively) and hospital admissions (r = −0.41, r = −0.45, r = −0.36, and r = 0.28, respectively).
CONCLUSIONS: DH and exercise capacity are reliable and independent predictors for mortality and morbidity in COPD patients. We propose that DH and exercise capacity be considered in the assessment of long-term clinical consequences of COPD patients.
Introduction
COPD is an important cause of chronic morbidity and mortality worldwide. Many people suffer from this disease for years and die prematurely from it or its complications. It is the fourth leading cause of death in the world, and further increases in mortality of COPD are expected in the coming decades.1,2
Several studies have shown that the FEV1 and diminished FEV1, hypoxemia, exercise capacity, body mass index (BMI), dyspnea index, and physical activity predict morbidity and mortality in COPD patients.3–7 Celli et al reported excellent predictive value of the multidimensional BODE (BMI, air-flow obstruction, dyspnea, exercise performance) index, which incorporates these variables into a single score.7 Identification and amelioration of predictors for COPD morbidity and mortality may improve long-term outcomes.
Pulmonary hyperinflation is usually defined as an abnormal increase of lung volume at the end of tidal expiration. The reduced elastic lung recoil, increased airways resistance, and development of expiratory flow limitation promote progressive air trapping, with an increase in the end-expiratory lung volume and a decrease in inspiratory capacity (IC). The resting IC is accepted as a reflection of end-expiratory lung volume.8 Static hyperinflation can be determined by measuring IC and/or the ratio of IC to total lung capacity (IC/TLC).8–10 Its increase during exercise is defined as dynamic hyperinflation (DH). During exercise, as ventilatory demand increases in flow-limited patients, progressive air trapping and further DH above the already increased resting value is inevitable.11 As the 6-min walk test (6MWT) is a reliable and more practical test to assess the fictional status of patients with COPD, it has become a popular alternative tool to the more formal cardiopulmonary exercise test. Some studies have demonstrated that DH can be assessed during a 6MWT.9,12,13
Static and dynamic lung hyperinflation have been associated with limitation in the functional capacity of COPD patients.4,8,9,11–13 It has been shown that dynamic lung hyperinflation has important clinical consequences in patients with COPD, such as dyspnea, pulmonary gas exchange impairment, increased ventilatory demand, expiratory muscle weakness, reduced exercise performance, daily physical activity, and impaired quality of life.11,14–16 A few longitudinal studies have assessed the impact of pulmonary hyperinflation on the prognosis of COPD. Recently, 2 studies assessed the impact of static hyperinflation on mortality in COPD patients and found that it was an independent predictor of mortality8,10; however, the possible value of DH in predicting survival has not been adequately evaluated.
We aimed to assess the impact of DH and exercise capacity in predicting mortality and also morbidity, as evaluated by emergency visits and hospital admissions because of exacerbations in patients with COPD during a 4 year period.
QUICK LOOK
Current knowledge
Dynamic hyperinflation in patients with COPD leads to exercise limitation and exercise intolerance. The relationship of exercise limitation to outcome is not well described.
What this paper contributes to our knowledge
Dynamic hyperinflation, measured by the ratio of the change in inspiratory capacity to total lung capacity (ΔIC/TLC), and exercise capacity, measured by the 6-min walk test, are reliable and independent predictors for mortality and morbidity in COPD patients.
Methods
A prospective cohort study of COPD patients was undertaken at the Chest Disease Department of Mersin University, Mersin, Turkey. The study protocol was approved by the ethical committee of the Mersin University School of Medicine. Written informed consent was obtained from all subjects before enrollment into the study.
We recruited 73 stable COPD patients, diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2003 criteria,17 from October 2004 to June 2005. Criteria for participation included a diagnosis of COPD, an age of 40 years or more, a smoking history of at least 10 pack-years, a post-bronchodilator FEV1/FVC of < 70%, and reversibility of < 200 mL or < 12% in FEV1 after inhalation of 200 μg salbutamol. Patients who were stable in the last 6 weeks before entering the study, with moderate to very severe disease (post-bronchodilator FEV1 < 80%) and taking optimal medical therapy, were included in the study. All subjects were assessed clinically and with a chest radiograph to ensure the absence of other important respiratory disease. Patients with an exacerbation or a recent respiratory-tract infection within the last 6 weeks, clinical history of asthma, atopy, allergic disease, bronchiectasis or other pulmonary disease, uncontrolled comorbidities likely to affect mortality, (such as malignant disorders, cardiovascular disease, or history of systemic disease); patients requiring long-term oxygen therapy or mechanical ventilation for respiratory failure; and patients with pulmonary rehabilitation history were excluded.
Pulmonary function tests, including spirometry and lung volumes measurements, were performed using computer-assisted spirometry (Vmax 22D, SensorMedics, Yorba Linda, California), in accordance with the European Respiratory Society's recommendations.18 Lung volumes were measured by multiple-breath nitrogen washout technique.19 The multiple-breath nitrogen washout technique was performed by a medical doctor after the procedure had been fully explained to each patient. A waiting period of 1 hour was recommended between lung volumes measured in patients with severe obstructive disease.19 Thus, we performed 6MWT after 1 hour of pre-exercise pulmonary function tests. Then, lung volume measurements were repeated immediately after the 6MWT. Static hyperinflation was measured by the IC/TLC at rest, and DH was measured by the change between post- and pre-exercise value of IC/TLC (ΔIC/TLC).8
Exercise capacity was evaluated with 6-min walk test, according to American Thoracic Society criteria.20 Arterial blood gas (PaO2 and PaCO2) samples were taken at rest while breathing room air, then measured immediately using a blood gas analyzer (AVL Omni, Roche Diagnostic, Basel, Switzerland).21 Dyspnea was evaluated by baseline dyspnea index.22 Combined Charlson comorbidity index was used to determine the degree of comorbidity.23
Subjects were seen every 3–6 months or until death. The follow-up ended in January 2009. Respiratory and all-cause mortality, emergency visits because of exacerbations, and the number of hospitalizations were recorded during the follow-up period. Information was obtained by reviewing medical records and from family members. An exacerbation was defined as sustained worsening of the subject's condition from the stable state and beyond normal day-to-day variation and necessitating any change in medication.24 The relationships of different respiratory parameters (FEV1%, BMI, 6-min walk distance [6MWD], static hyperinflation, DH, PaO2, and PaCO2) with emergency visits and hospital admissions because of exacerbations, and also with respiratory and all-cause mortality, were assessed.
Statistical Analysis
Statistical analyses were performed using statistics software (SPSS 11.5, SPSS, Chicago, Illinois, and MedCalc 9.6.4, clinical calculators at http://www.medcalc.com). Data are presented as mean ± SD. The baseline characteristics of the study subjects who died and those who remained alive were compared by using the unpaired Student t test for continuous variables. Emergency visits and exacerbation-related hospital admissions of the patients were compared with the Mann-Whitney U test.
A receiver operating characteristic type II analysis, with mortality as the gold standard reference, was used to determine the better cutoff point for ΔIC/TLC.25 Kaplan-Meier analysis for survival due to all and respiratory causes was performed with a ΔIC/TLC and 6MWD cutoff value according to the model of comparison between 2 sample groups, and the differences between curves were evaluated by the log-rank tests. We performed Cox proportional hazard regression analyses under the proportional hazards assumption to evaluate the cutoff value for ΔIC/TLC, 6MWD, and integrated index (combined ΔIC/TLC and 6MWD) to predict the risk of death. Multivariable regression analysis (Cox regression proportional hazards model) was used to determine the independent predictors of all-cause and respiratory mortality. Additionally, we computed the C statistic by means of a Cox model, as either dying or surviving. The null value for the C statistic is 0.5, with a maximum of 1.0 (with higher values being better). The association of emergency visits and hospital admissions with clinical and functional parameters was determined using Spearman rank correlation analysis. Statistical significance was considered at P < .05 level.
Results
Demographic, clinical and spirometric characteristics are presented in Table 1. The median follow-up period was 47 months (IQR 45–48, n = 73). During the follow-up there were 8 (11%) deaths (Fig. 1), due to respiratory illness in 6 (75%) patients, non-respiratory illness in 1 (12.5%), and not identified in 1 (12.5%).
Characteristics of Subjects With COPD (n = 73)

Cumulative mortality. During the follow-up there were 8 (11%) deaths.
The mean emergency visit frequency of patients was 2.75 ± 1.75 visits during the follow-up period in the deceased COPD group versus 0.72 ± 1.32 during the follow-up period in the alive COPD group during the follow-up period (P < .001), and 17.8% of the patients had been hospitalized because of exacerbation. The frequency of hospitalization was 75% in the deceased COPD group, versus 11% in the alive COPD group. Median hospital stay was 13 days (IQR 10–16 d, n = 10) in the deceased COPD group, versus 7 days (IQR 5–8 d, n = 11) in the alive COPD group. Invasive mechanical ventilation was performed in 3 patients (4.1%), who were in the deceased subjects group.
Clinical and functional characteristics of the subjects with COPD according to survival are shown in Table 2. Subjects who died had lower FEV1 levels, more DH, and less 6MWD than those who survived.
Clinical and Functional Characteristics of the Subjects With COPD According to Survival
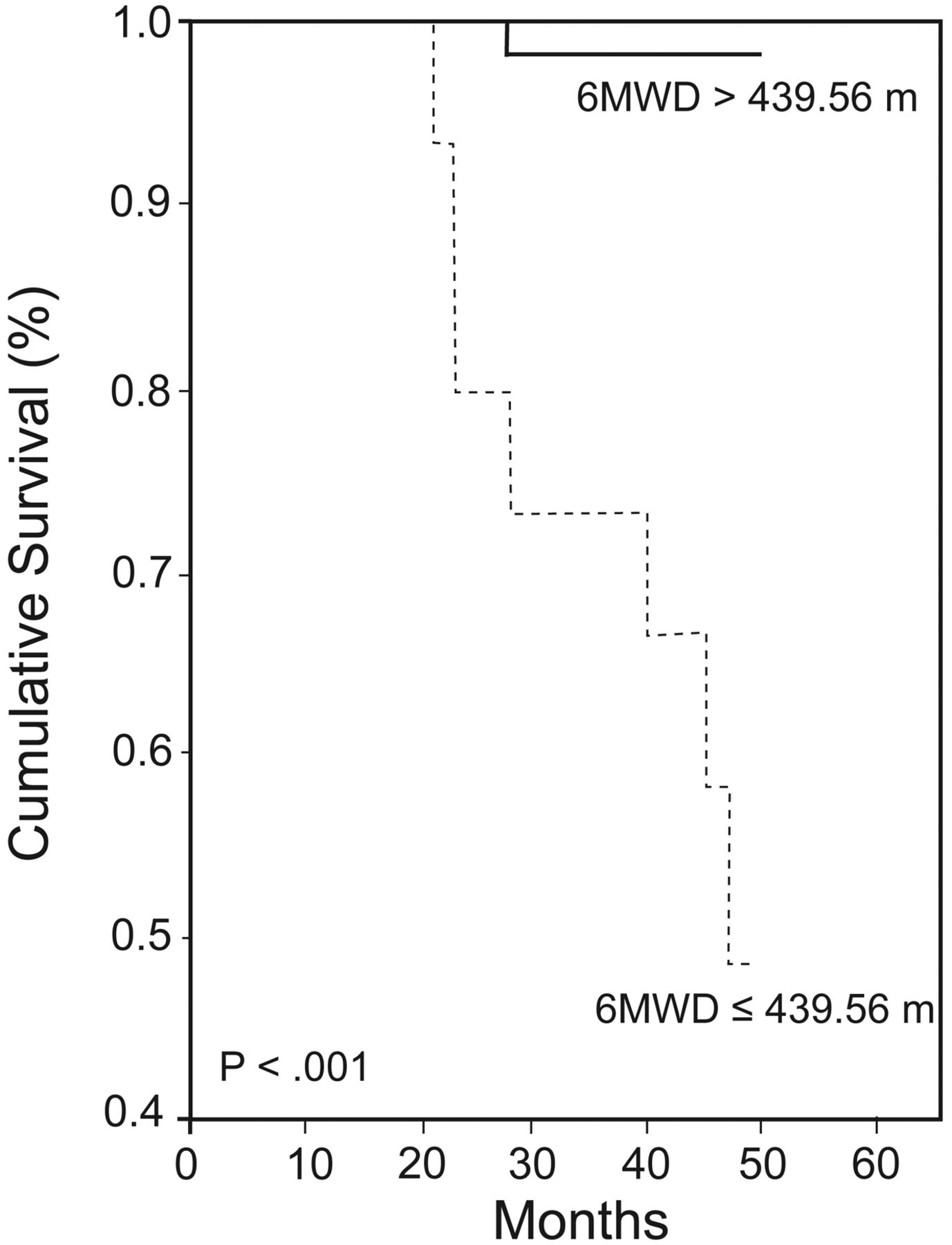
According to the receiver operating characteristic curve analysis, cutoff points for ΔIC/TLC and 6MWD were obtained as > 4 and ≤ 439.56 m, respectively. The Kaplan-Meier survival curve for all-cause mortality related to ΔIC/TLC, using the 4 value as threshold, is shown in Figure 2. The cumulative survival rate was significantly lower in the COPD patients with ΔIC/TLC > 4. The sensitivity and specificity rates of ΔIC/TLC are 100% (95% CI 62.9–100.0%) and 56.92% (95% CI 44.0–69.1%), respectively. The Kaplan-Meier survival curve for all-cause mortality shows that mortality rate was also related to 6MWD, using the value of 439.56 m as the threshold (Fig. 3). The sensitivity and specificity rates of 6MWD were 87.5% (95% CI 47.4–97.9%) and 87.69% (95% CI 77.2–94.5%), respectively.

Mortality rate according to dynamic hyperinflation. The Kaplan-Meier survival curve for all-cause mortality related to the change in the ratio of inspiratory capacity to total lung capacity (ΔIC/TLC), using the 4 value as the threshold, is shown. A P value for ΔIC/TLC could not be computed, since all the patients in the ΔIC/TLC ≤ 4 group survived.
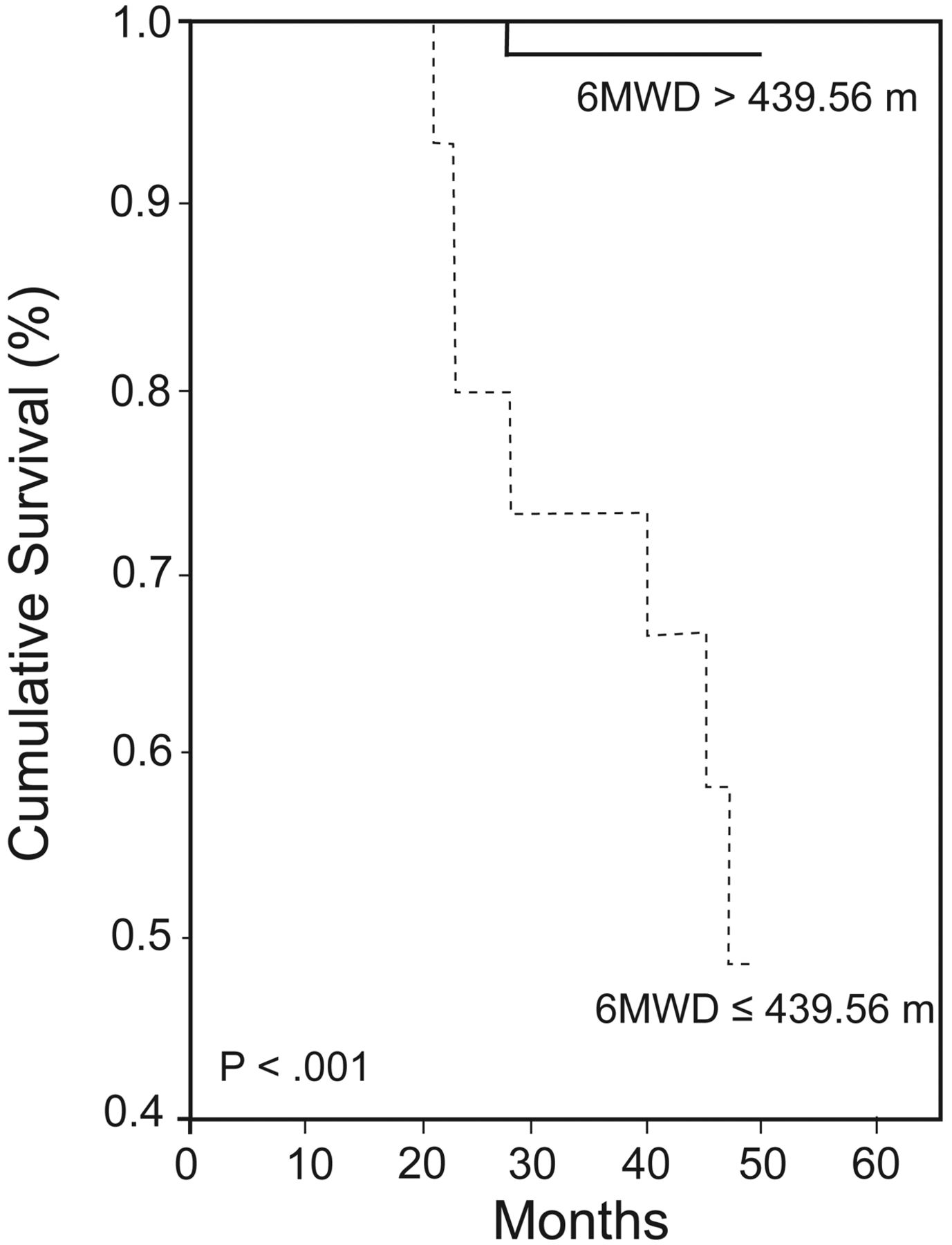
Mortality rate according to 6-min walk distance (6MWD). The Kaplan-Meier survival curve for all-cause mortality related to 6MWD, using the 439.56 m value as the threshold, is shown. Using the log rank P value to compare these curves, there was a significant difference between the 2 groups in terms of survival.
Additionally, we used an integrated index that combined DH and exercise capacity to predict exacerbations and survival. This integrated index was found to be more specific to predict for mortality, as compared to DH or exercise capacity alone (Fig. 4, Table 3). The sensitivity and specificity rates of this integrated index were 87.5% (95% CI 47.38–97.93%) and 96.9% (95% CI 89.30–99.54%), respectively. The C statistic for the ability of the our integrated index to predict the risk of death was 0.92 as compared with a value of 0.79 with the use of DH alone, and with a value of 0.88 with the use of 6MWD alone.

Mortality rate according to our integrated index that combines DH and exercise capacity. The Kaplan-Meier survival curve for all-cause mortality related to our integrated index is shown. Using the log rank P value to compare these curves, the cumulative survival rate was significantly lower in the COPD patients whose change in the ratio of inspiratory capacity to total lung capacity (ΔIC/TLC) was > 4 and whose 6-min walk distance (6MWD) was ≤ 439.56 m, compared to the other COPD patients.
Mean Survival Time and 95% Confidence Interval Estimations for Dynamic Hyperinflation, 6MWT, and Integrated Index
On the basis of multivariable regression analysis (Cox regression proportional hazards model), DH (hazard ratio = 1.4, 95% CI = 1.09–1.84, P = .009) and 6MWD (hazard ratio = 0.98, 95% CI = 0.97–0.99, P = .006) were found to be independent predictors of all-cause and respiratory mortality (Table 4). Compared to the patient group with ΔIC/TLC ≤ 4, the patients with ΔIC/TLC > 4 were more likely to have a shorter time to death (see Table 3).
Independent Predictors of All-Cause (and Respiratory) Mortality*
6MWD, FEV1%, PaCO2, IC/TLC, and ΔIC/TLC were found to be significantly related to morbidity and emergency visits. In addition, 6MWD, BMI, FEV1%, IC/TLC, and ΔIC/TLC were found to be significantly associated with exacerbation-related hospital admissions (Table 5).
Predictors of Morbidity
Discussion
In this study, different clinical and physiologic parameters (FEV1%, BMI, 6MWD, baseline dyspnea index, PaO2, PaCO2, static and DH) were assessed. FEV1, walk distance, and DH were found to be significant risk factors for mortality, emergency visits, and hospital admissions related to exacerbations. On the other hand, static hyperinflation was found to be correlated with emergency visits and hospital admissions because of exacerbations; however, this was not found to be a statistically significant risk factor for mortality.
It was assumed that DH was related to poor dyspnea, exercise capacity, daily physical activity, and quality of life11,14–16; however, no study has evaluated the effects of DH on COPD prognosis. Garcia-Rio et al identified DH and distance walked during 6 min as significant predictors of physical activity in moderate to very severe patients. The development of DH makes patients breathe at larger operational volumes, which results in an increase in respiratory effort, greater neuromechanical dissociation, and a greater perception of dyspnea.13,26 At the same time, DH contributes to the weakness and fatigue of the respiratory muscles26 and promotes deconditioning. Additionally, much pulmonary pathophysiological impairment occurs due to the inactivity, and patients therefore enter into a vicious circle. This configures a cycle of inactivity, deconditioning, and dyspnea that can cause the disease to worsen and progress.13
To best of our knowledge, this is the first study reporting that DH is an independent predictor of all-cause and respiratory mortality in patients with COPD. This study also shows that DH is related to emergency visits and hospital admissions because of COPD exacerbations. Indeed, these findings are not surprising. Static hyperinflation has been recently shown as an important mortality and morbidity predictor in the 2 large cohorts of COPD patients.8,10 Tantucci et al found that IC (percent of predicted) was a powerful functional predictor of all-cause and respiratory mortality, and of exacerbation-related hospital admissions in COPD patients. They concluded that parameters reflecting changes in lung volume (IC and IC/TLC) were more sensitive and specific in predicting mortality in COPD patients than those reflecting air-flow obstruction (FEV1 and FEV1/FVC).10 Casanova et al also showed that static hyperinflation measured as IC/TLC was an independent predictor of mortality in COPD.8
Our results also show that FEV1, when assessed alone, is a significant risk factor for mortality in COPD. However, FEV1 was not a significant risk factor for mortality when assessed with other clinical and functional parameters (BMI, 6MWD, baseline dyspnea index, PaO2, PaCO2, or static or dynamic hyperinflation). These findings support the reports of recent studies on this issue. In classical studies, FEV1 was the strongest factor in predicting mortality, compared with other variables (such as blood gases, pulmonary artery pressure).27,28 However, recent studies suggest that other parameters not explored previously (BMI, dyspnea, walk distance, health-related quality of life) independently predict outcome in COPD, and some are better predictors of this outcome than FEV1.5,7,29–32
This study also shows that 6MWD is an independent predictor for mortality in COPD patients when assessed alone in the univariate analysis, and with other clinical and functional parameters in the multivariable regression analysis. Recent studies reported that 6MWD could be used to predict outcome in COPD,7,29,30 and that it was a better predictor of mortality than FEV1.30 The present results are in agreement with the findings of Pinto et al.30
Combining other health measures with FEV1 provides a more complete view of COPD patients' clinical situation and prognosis. This was the rationale for the development of the BODE index,7 which has gained widespread acceptance in the medical community. Since then, several research groups have attempted to improve upon the BODE index with multidimensional instruments with greater predictive capacities. These include the Health, Activity, Dyspnea, Obstruction (HADO) score33 and the Age, Dyspnea, Obstruction (ADO) index.34 In this study we also evaluated an integrated index that combined DH and exercise capacity to predict morbidity and mortality, and we found that this integrated index was more specific to predict mortality, as compared to DH or exercise capacity alone. Accordingly, we thought that the assessment of this integrated index may be more useful than a single parameter to predict the outcome of COPD patients. Compared to other multidimensional COPD prognostic indexes, our integrated index predicts mortality better than the BODE index (C statistic 0.92 vs 0.74)7 and HADO index (C statistic 0.92 vs 0.68).33 However, the predictive capacity of this integrated index for mortality is not directly comparable with other multidimensional prognostic indexes in the literature, because the integrated index defined in this study includes different variables, such as DH and exercise capacity, and we had a limited sample.
The relationship between pulmonary DH and a higher risk of mortality in COPD patients is yet unknown, and further investigations are needed. Some hypothetic mechanisms, such as more frequent exacerbations and systemic involvement, are suggested in exploring the link between static hyperinflation and mortality.10 We believe that the same mechanisms could be related for DH and mortality, because COPD treatments that have been shown to reduce DH are also effective in decreasing exacerbations.35,36 There is also a decrease in morbidity and mortality with COPD treatments that reduce DH, such as lung-volume-reduction surgery and long-acting anticholinergics.35,37 The critical expiratory air-flow limitation with consequent DH seems to be the basic pathophysiology in COPD exacerbation. These changes lead to further derangement in ventilatory reserve, including mechanics, muscle function, and gas exchange. Increased DH is associated with lower ventilatory tolerance, and these patients cannot tolerate the ventilatory overload during exacerbations. Thus, COPD patients develop respiratory failure that is highly associated with the need for mechanical ventilation and with mortality.38
Our study had some advantages, as compared with similar studies, including long-term (mean 4 years) and close follow-up of the patients and, therefore, fuller knowledge of the causes of mortality. On the other hand, our study had some limitations. First, the total number of patients with at least stage III COPD was relatively low. Because of the relatively small sample in this study, we used select optimal cut points on a receiver operating characteristic curve for exercise capacity and DH data in the methodology, and these are subject to poor generalizability. Therefore, we propose that further validation of these cut points should be performed prior to clinical use. The second limitation was the use of multiple-breath nitrogen washout technique in the measurement of lung volumes. It was shown that plethysmographic lung volume measurement includes non-ventilated, as well as ventilated, lung compartments, and, thus, yields higher results than the gas-dilution or washout methods. In patients with severe air-flow obstruction the true value of lung volumes is underestimated by the gas-dilution or washout methods.19 DH was measured in this study by means of consecutive IC recordings at the end of the exercise. Moreover, since DH decrease rapidly after the end of exercise9 and the multiple-breath nitrogen technique takes about 7 min, our measurements probably underestimated the end-expiratory lung volumes. Maybe not only the magnitude of the augmentation in end-expiratory lung volume during the exercise, but also the normalization rate post-exercise contributed to the IC/TLC values observed.
Conclusions
In conclusion, DH and exercise capacity are reliable and independent predictors for mortality and are also related to morbidity in COPD patients. We propose that our integrated index that combines DH and exercise capacity should be considered in addition to other clinical and physiologic parameters in the assessment of long-term clinical course of patients with COPD.
Footnotes
- Correspondence: Eylem Sercan Ozgur MD, Mersin Universitesi Tıp Fakültesi, Göğüs Hastalıkları AD, 33079, Mersin, Turkey. E-mail: eylemozgur{at}yahoo.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}