

Abstract
BACKGROUND: There is an urgent need to develop new outcome measures for respiratory therapy, to evaluate its effectiveness. Adventitious sounds generated from the lungs (crackles and wheezes), can now be quantified and characterized objectively with computer technology. To our knowledge, this is the first reported study designed to assess any change in lung crackles before and after a single session of airway clearance therapy.
METHODS: Twenty-three stable bronchiectasis patients were recruited from United Kingdom out-patient clinics and treated with a single session of airway clearance therapy, using the active cycle of breathing technique. Sound recordings were made before and after the session at 7 anatomical chest locations. Computerized lung sound analysis was used to measure crackle parameters: 2-cycle deflection width (2CD), and crackle number per breath cycle (nBC). Perceived breathlessness, lung function, and oxygen saturation data were also recorded.
RESULTS: Crackle mean 2CD and mean nBC increased post intervention. Sixteen participants (70%) showed a statistically significant difference in mean crackle 2CD before and after the session at ≥ 1 chest location. Thirteen (57%) participants had a difference between mean crackle 2CD before and after the intervention > 1 Smallest Real Difference (SRD, mean SRD = 2.23 ms) at ≥ 1 chest location. Differences in mean crackle nBC before and after the intervention did not exceed the SRD (mean SRD = 32 crackles per breath cycle) in any participant. Perceived breathlessness was significantly reduced post intervention; no significant changes were observed in either lung function or oxygen saturation.
CONCLUSIONS: Crackle duration (2CD) was found to change after a single session of airway clearance therapy, and shows promise as a new outcome measure for respiratory therapy interventions.
- airway clearance therapy
- crackles
- lung sounds
- outcome measure
- respiratory therapy
- physical therapy
- physiotherapy
Introduction
Respiratory therapy is used routinely in clinical practice to manage respiratory problems such as breathlessness, excess lung secretions, reduced lung volumes, and low exercise tolerance. However, little is known about the effectiveness of the individual respiratory interventions applied, partly due to the lack of available reliable, valid, sensitive, and specific outcome measures. The outcome measures currently used to assess the effectiveness of respiratory therapy interventions are generally flawed and have been discussed in detail elsewhere.1 To our knowledge, this is the first reported study designed to assess any change in lung sounds before and after a single session of airway clearance therapy.
Sounds generated from the lungs have the potential to provide useful clinical information, as they relate directly to movement of air, changes within lung tissue and morphology, and secretions.2 Research into the acoustic properties of lung sounds has suggested that different parts of the airways produce adventitious lung sounds (such as crackles and wheezes3) with different characteristics (ie, central airways produce coarser crackles while peripheral airways produce finer crackles4–6). The technique of computer aided lung sounds analysis (CALSA), applying expanded time and spectral analysis techniques to crackle and wheeze parameters,4 has been used to detect and characterize the severity of lung disease,5,6 but it has yet to be evaluated as an outcome measure for respiratory therapy. The use of CALSA to characterize crackles over short periods has been shown to provide an objective and reliable measure in a clinical setting.7 However, before crackle analysis can be recommended as an outcome measure for respiratory clinical practice, it is necessary to demonstrate that crackle parameters change after an intervention.
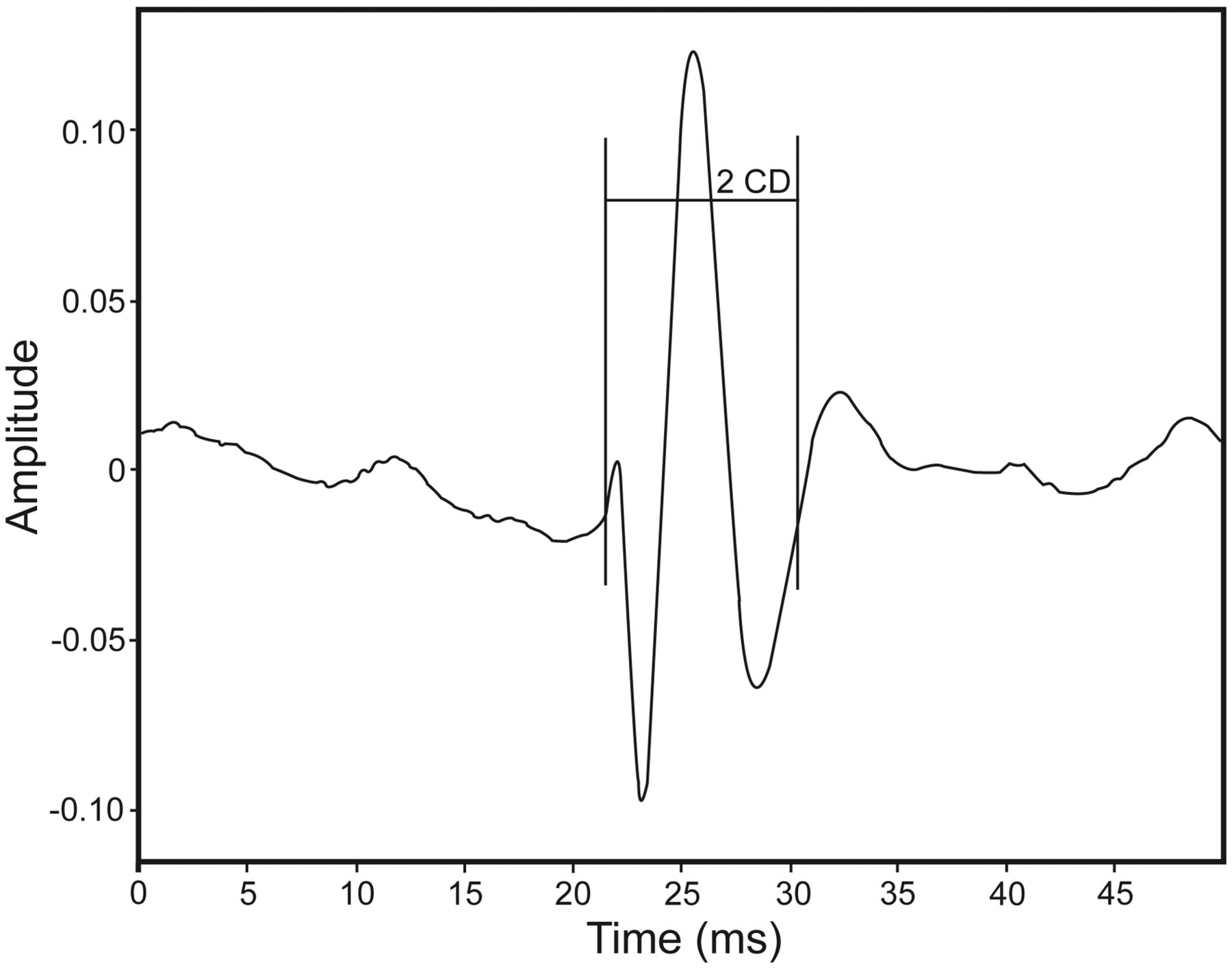
Respiratory clinicians describe crackles as many or few, early or late, coarse or fine. Using CALSA, crackles can be objectively characterized based on their number per breath cycle (nBC, Fig. 1) or their duration. The 2-cycle deflection width (2CD) is the duration of the first 2 cycles of a crackle, in milliseconds (Fig. 2). Crackle 2CD has been shown to be a more stable and reliable measure than another parameter measuring crackle duration, the initial deflection width.7
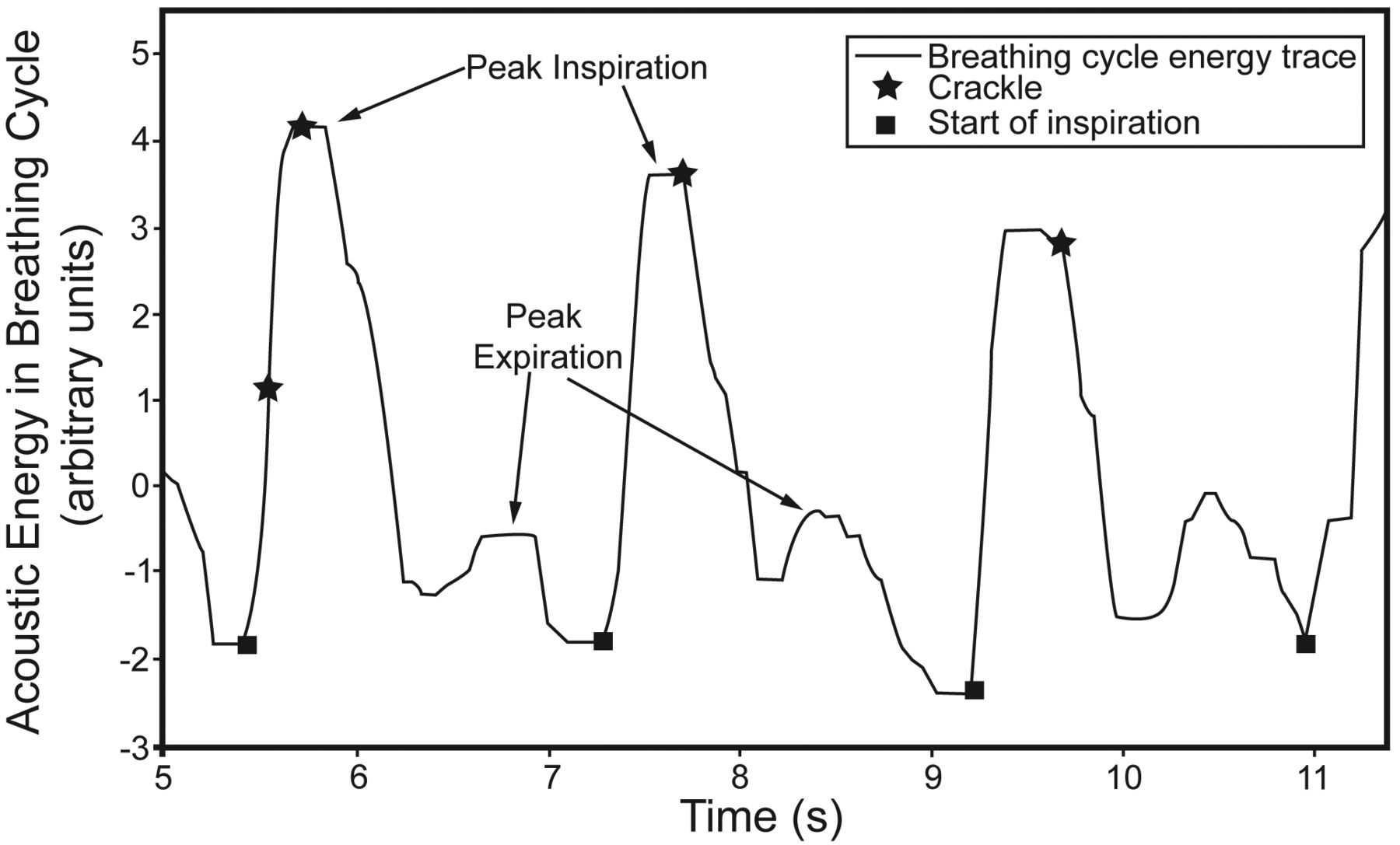
The solid line show the acoustic energy due to the flow noise during the breathing cycle. Each cycle starts at the point marked with a black square. The first, larger peak in each cycle relates to inspiration, and the second, smaller peak to expiration. The stars are the locations of identified crackles within the breathing cycle. The crackle number per breath cycle (nBC) is the mean number of crackles in each breath cycle in the record. This is calculated by counting the number of crackles in each cycle in the record and averaging over the total number of cycles. In the example shown there are, respectively, 2, 1, and 1 crackles per sample, so for this extract of the signal nBC = 1.33.

Representation of crackle 2-cycle deflection width (2CD).
The aim of this study was to explore whether crackle parameters are appropriate for use as an outcome measure in respiratory practice, with 2 specific objectives:
To investigate whether crackle 2CD or crackle nBC is affected by the application of a single session of an airway clearance intervention.
To assess the expected effect size for crackle 2CD and crackle nBC by calculating the smallest real difference (SRD).8
QUICK LOOK
Current knowledge
Breath sounds determined using traditional auscultation are frequently used to evaluate the success of airway clearance maneuvers. The subjective nature of breath sounds and variations related to technique render these evaluations suboptimal.
What this paper contributes to our knowledge
Computer aided lung sound analysis represents an objective measure for monitoring respiratory therapy, including airway clearance maneuvers. The measurement of the 2-cycle detection width and the duration of crackles (in milliseconds) appear to be stable and reliable measurements.
Methods
This study was conducted in the Faculty of Health Sciences, University of Southampton, Highfield, Southampton, United Kingdom.
Design
A single group, repeated measures design was used, in which sets of lung sound recordings were made from the same participants twice on the same day, 3 before and 3 after a single airway clearance intervention.
Participants, Centers
The study received full approval from the Southampton and South West Hampshire Research Ethics Committee (A). Twenty-three participants were recruited for this study via bronchiectasis out-patient clinics held at Queen Alexandra Hospital, Portsmouth, on the south coast of the United Kingdom. Participants were eligible if they were able to give and sign informed consent; had a documented medical diagnosis of bronchiectasis, made by a consultant respiratory physician; were ≥ 18 years of age; and had been clinically stable for one month prior to the study (defined as no hospital admissions, no exacerbations/infections, and no change in prescribed medication). Patients were excluded from the study if they had co-existing lung pathologies.
Sample Size
A convenience sample was recruited since no prior information on expected sample variance in crackle parameters was available to permit a power calculation to determine sample size.
Intervention
A standard airway clearance technique (active cycle of breathing technique) was performed with each participant, by the same experienced respiratory physiotherapist, for a single treatment session in an out-patient setting. Active cycle of breathing technique is the most frequently used airway clearance technique in the United Kingdom.9 Cycles were repeated until the participant felt his or her chest to be clear. On average, each session lasted 24 min, with a range between 15 and 30 min. Typically, airway clearance treatment sessions last from 20–30 min.10
Outcome Measures
The modified Borg Scale11 was used to collect perceived breathlessness data. FEV1, FVC, and peak expiratory flow (PEF) were recorded using a spirometer (Microlab 3500, Micro Medical/Carefusion, San Diego, California), which was calibrated daily; and oxygen saturation data were collected with a pulse oximeter (Pneupac, Sims, Luton, United Kingdom). Lung sound recordings were performed with an electronic stethoscope (Master Elite, Welch Allyn, Skaneateles Falls, New York). The output from the stethoscope was connected via an integral amplifier to the sound card of a laptop with customized software suitable for data acquisition, written in Matlab 7.1 (Mathworks, Natick, Massachusetts). Lung sounds were recorded with a sampling frequency of 44.1 kHz and a quantization of 16 bits for all recordings.
Demographic and basic anthropometric data (height and weight) were recorded first. Breathlessness and oxygen saturation levels were then registered. Baseline lung sound recordings were performed with the electronic stethoscope held by hand over each location (previously marked in pen on the patient's chest to ensure that the stethoscope was placed on the same location) for 25 seconds per recording. Three recordings per location were made at baseline to provide data for a reliability study published elsewhere.7 For this before-after study, one of the 3 baseline recordings was selected at random for analysis. Lung sound recordings followed the guidelines for short-term acquisition from the Computerized Respiratory Sound Analysis (CORSA) project group.12 Although the trachea is one of the 7 recording sites recommended in the CORSA guidelines, Gavriely and Cugell13 have reported that lung sounds from the trachea are differently filtered than those from other sites. In addition, clinicians rarely use this site for assessing crackles. It was therefore decided not to include tracheal data for this study. Spirometry was performed in accordance with published guidelines,14 after the lung sound recordings. After the intervention, lung sound recordings, breathlessness, oxygen saturation, and lung function tests were repeated, using the same procedure as at baseline. Lung function tests were performed after the lung sounds recordings (approximately 15 min after the intervention), because forced expiratory maneuvers could affect lung sounds.
Data Analysis
All tests for statistical significance were at the 95% level.
Analysis of Demographic and Anthropometric Data
Body mass index (BMI), in kg/m2, was calculated using the formula BMI = weight/(height)2. Descriptive statistics were used to summarize the sample.
Analysis of Breathlessness, Oxygen Saturation and Lung Function
Analysis was based on data collected at baseline and immediately post intervention. The predicted values used for lung function were based on the European Respiratory Society reference values,15 and the highest of the 3 spirometric measures performed at baseline and post intervention was used for analysis. The comparisons (at baseline and post intervention) for the lung function and oxygen saturation variables were made using a paired sample t test. Breathlessness comparisons were made using the non-parametric Wilcoxon signed rank test. Any statistically significant results were explored further by examining for changes exceeding the published minimally clinically important difference.16
Lung Sound Analysis
All sound files were processed using algorithms written in Matlab. Crackles were detected based on an algorithm developed by Vannuccini et al,17 which has been validated for sensitivity (84%) and specificity (89%) against clinical data. The reasons for this choice have been discussed elsewhere.7
Breathing Cycle Detection
A method analogous to that reported by Que et al18 was used to detect the breath cycles automatically. However, since a fully automated breath cycle detection process was not found to be reliable in the presence of substantial numbers of crackles, manual adjustment of the detection thresholds was permitted. Threshold adjustment was based on visual inspection of the plotted signal, and aural extraction of the breath cycle phases by a physiotherapist familiar with auscultation techniques.
Crackle Parameter Analysis
A database was created for the data (at both baseline and post intervention) at each chest location, per participant, for crackle 2CD and crackle nBC. Mean nBC was calculated by averaging nBC across all complete breath cycles in the recorded signal for a given participant and chest location. Mean 2CD was calculated by averaging across all crackles in the recorded signal for a given participant and chest location. For each participant and each chest location the difference in mean nBC and in mean 2CD pre and post intervention was compared by a paired t test.
The group mean 2CD and group mean nBC detected pre intervention in each of the 6 chest locations were compared to the corresponding post intervention group means using a 2-way analysis of variance, where the participant was considered a random factor and the time (pre/post intervention) was a fixed, repeated measures factor.
For crackle parameters, the minimally clinically important difference has yet to be determined, so the SRD was chosen to explore the size of any effect. The SRD represents the smallest change that can be interpreted as a real difference in excess of measurement “noise”8 and is estimated by SRD = 1.96√2(SEM). The standard error of measurement (SEM) was obtained from the baseline data by calculating the square root of the within participant mean square values from the analysis of variance table generated by comparing the mean dependent variable (2CD, nBC for a given location across all participants) in 2 sets of pre intervention data selected at random for the 3 data sets recorded for each subject. The difference between the pre and post intervention means of the crackle 2CD for each chest location for each participant was obtained by subtracting the mean 2CD after treatment from the mean 2CD before treatment. The corresponding calculation was also made for the mean nBC. Participants with a difference at any chest location greater than ± 1 SRD were identified.
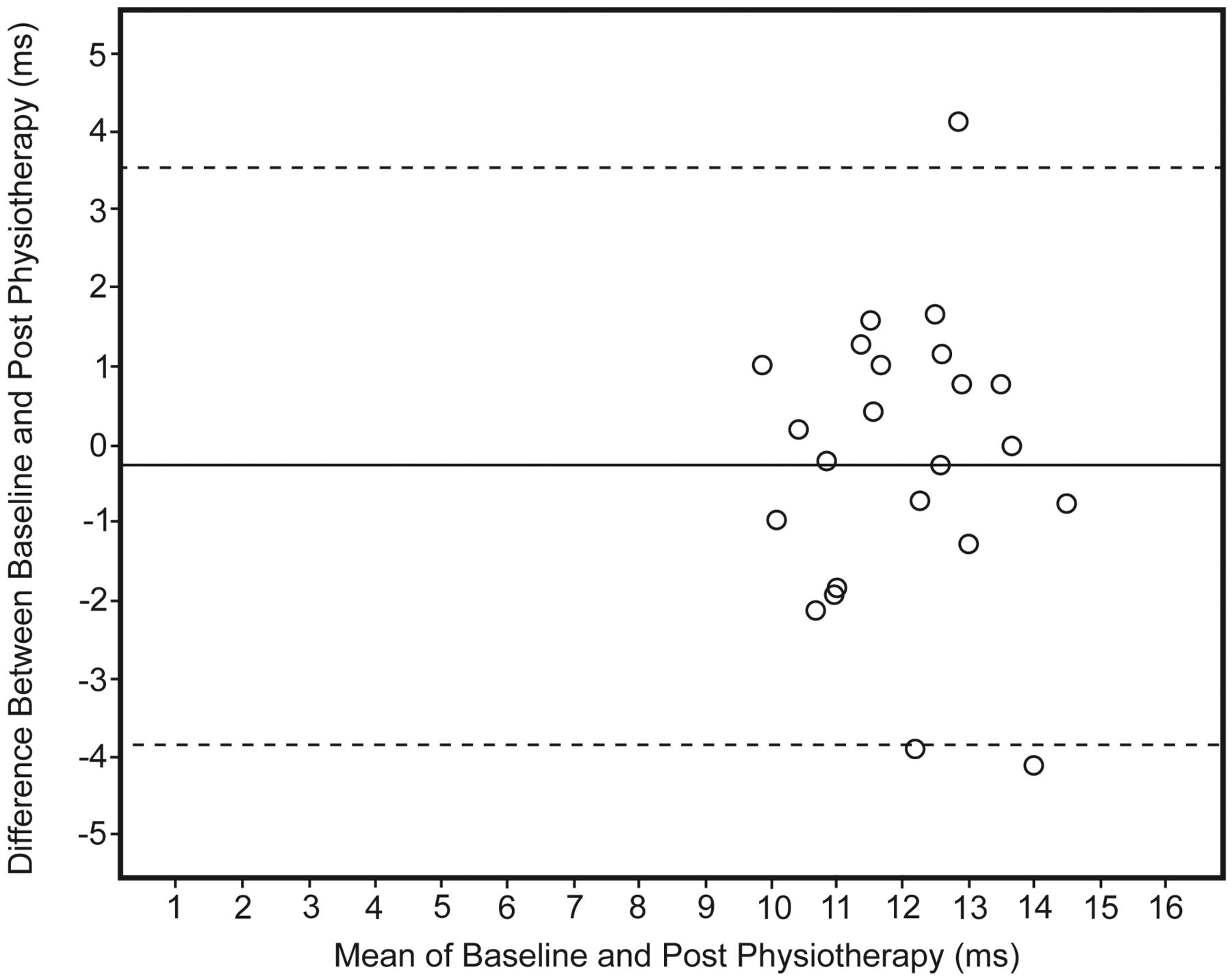
Finally, any systematic bias in the difference of the pre and post intervention means was sought using Bland-Altman plots.18 These plots provide a visual representation of agreement, with easy identification of systematic bias, outliers, and any relationship between the variance in measures with the size of the mean.
Results
Twenty-three participants (14 female, 61%) of 61.2 ± 9.6 years old (age range 25–73 years old), were recruited. The average BMI of the sample (28.3 ± 5.6 kg/m2) was higher than deemed “normal.” The majority of crackles were coarse (2CD > 10 ms) and occurred early in the breathing cycle, which is compatible with previously published data from patients with bronchiectasis.19
Breathlessness, Oxygen Saturation, and Lung Function
The group mean breathlessness score was statistically significantly lower after the airway clearance intervention (P = .02). Twelve out of the 23 participants (52%) perceived themselves to be less breathless, in comparison to their baseline perception, and in 10 of these the difference was equal to or exceeded the published minimally clinically important difference for the modified Borg score (1 unit).16 Post hoc Cohen's d was calculated as 0.4, with an effect size r of 0.2, which indicates a small to medium effect.20
The group means at baseline and post airway clearance intervention for the oxygen saturation levels and each lung function variable were similar, and no statistically significant differences were found (Table 1 and Table 2).
Descriptive Statistics for Breathlessness Data (Modified Borg Scale) Before and After Intervention With Wilcoxon Signed Rank Test Results (n = 23)
Descriptive Statistics for Oxygen Saturation and Spirometry Data Before and After Intervention With Paired t Test Results and 95% Confidence Intervals for the Difference Between the Means (n = 23)
Crackle 2CD and nBC
Pre intervention an average across all chest locations and all participants of 4.14 ± 2.31 crackles per BC was detected, with a 2CD of 11.8 ± 1.50 ms. Post intervention an average across all chest locations and all participants of 4.18 ± 2.25 crackles per BC was detected, with a 2CD of 11.9 ± 1.54 ms. Neither the group mean 2CD nor the group mean nBC showed statistically significant change from pre to post intervention at any chest location.
The results above relate to average changes across the group; however, in this study our main interest was in exploring any changes that occurred within individuals from before to after the intervention. We therefore quantified these individual changes. When the individual data were analyzed, there were statistically significant changes in mean 2CD within 16 participants (70%). The direction of change was inconsistent, although there were twice as many cases of significant mean 2CD increase (coarser crackles) as there were cases of significant mean 2CD decrease. The significant changes recorded at the posterior right location were uniformly in the direction of an increase in mean 2CD after the airway clearance intervention (this was seen in 5 participants). Seven participants (30%) showed no significant change in mean 2CD at any location. When mean nBC data were analyzed in the same way, there were statistically significant changes in mean nBC within 10 participants (43%). The direction of change was inconsistent, but there were twice as many cases of significant mean nBC decrease (fewer crackles) as there were cases of significant mean nBC increase. Nine of the 19 examples (47%) of significant changes were seen in the posterior locations.
Smallest Real Difference
Table 3 shows that the baseline SRD values varied across chest locations for the mean 2CD and mean nBC. The same table also shows the number of participants who presented a change > 1 SRD in mean 2CD or nBC from pre to post intervention. At the 95% level it would be expected that from a sample of 23 people, approximately one participant would show such change by chance. It is evident that mean 2CD showed a change > 1 SRD at all chest locations (except the posterior right) in more participants than would be anticipated by chance at the 95% level, but mean nBC did not. Of the 23 participants, 13 (57%) had changes in mean 2CD > 1 SRD at a minimum of one location. The lateral locations recorded the majority of changes > 1 SRD, with the left lateral location recording changes > 1 SRD in 7 participants (30%). None of the participants had a change in mean nBC > 1 SRD at any location.
Smallest Real Difference Values Obtained From the Analysis of Mean Crackle 2CD and Mean nBC at Baseline, and the Number of Participants With a Difference Before and After Treatment > 1 SRD, at Each of the 6 Chest Locations
Bland-Altman Plots
Bland-Altman plots revealed the existence of some systematic bias between pre and post intervention for mean 2CD, but not for mean nBC. Figure 3 shows a typical example using the mean 2CD data.

Bland-Altman plot showing 95% limits of agreement for the crackle 2-cycle deflection width (n = 23) at the anterior right of the chest, using data at baseline and post airway clearance intervention.
Discussion
This research has shown that in stable bronchiectasis no statistically significant change at the 95% level was seen in group means for crackle 2CD and nBC from before to after a single session of airway clearance. However, individual participants frequently had statistically significant changes in one or both parameters. For each anatomical chest location, more participants showed a change in mean 2CD > 1 SRD (derived from the baseline data) than would be expected through chance alone, although the direction of this change was not consistent across participants. The left lateral recording location produced the largest number of changes in 2CD > 1 SRD. No corresponding pattern was found relating to the mean nBC.
The intervention was standardized by ensuring that the same physiotherapist performed all maneuvers and used a standard airway clearance technique (active cycle of breathing technique). However, in accordance with normal clinical practice, the physiotherapist had some flexibility in terms of the duration of the single treatment session, continuing until the participants felt their chest to be “clear.”
There is no gold standard to determine effectiveness of airway clearance, so the effectiveness of the intervention provided in this study is uncertain. It is possible that the observed changes in each individual for the mean crackle 2CD and mean crackle nBC occurred by chance, as this was an exploratory study and no control group was included. However, this is unlikely, as statistically significant changes were observed in 16/23 patients for the mean crackle 2CD, and in 10/23 patients for the mean crackle nBC. The fact that the direction of change was inconsistent and that in some patients no change was observed also supports this argument, as the session of airway clearance might not have cleared the patient's chest or might not have been sufficient to produce a measurable effect in some patients.
In this study air flow was not standardized, which might have affected the results. However, of all the methods to measure flow, the pneumotachograph has been considered the gold standard,21 but the patient has to breathe using a mouthpiece or a face mask. This causes patient discomfort, is not practical, and changes the breathing pattern and therefore is rarely used clinically.22,23 Furthermore, gathering breathing cycle data from non-acoustic means (eg, from pneumotachographs) may be difficult or impossible in some populations and pathologies. These aspects have also been acknowledged by other researchers.24 Breathing cycle detection without air flow measurements has been successfully achieved.24–26 However, these researchers used 6 simultaneous microphones attached to the trachea and chest, and the data were recorded in a respiratory acoustics laboratory and on healthy subjects. An acoustical approach to respiratory phase detection is attractive, because it is objective, noninvasive, relatively inexpensive, and convenient to use24 in a clinical setting. Our use of it in this study was intended to explore an outcome measure to be used clinically.
In the absence of a gold standard to define the magnitude of minimally clinically important changes, the SRD provides evidence of a real change that is not attributable to “error” or “noise.”8 Changes smaller than the SRD should be interpreted as measurement error, while changes larger than the SRD can be interpreted as a real change in values. In this study, differences in mean 2CD were greater than the SRD in several participants at each chest location except the posterior right. This supports the hypothesis that crackle mean 2CD is responsive to change. No participants demonstrated a difference > 1 SRD for mean nBC. This suggests that mean nBC is a stable parameter that is not affected by airway clearance techniques, or that it is not responsive to change. Vyshedskiy et al27 have recently reported on the stability of crackle rate within single examination sessions, despite intervening maximal breathing maneuvers. Recording for 25 second periods provided sufficient data for our crackle analysis. However, there was considerable variability in the interaction effect between subject and data sample for the number of crackles per breath cycle, which resulted in a very high variance when calculating the nBC SRD figures per location. It is possible, therefore, that nBC might be responsive to change if recordings were taken for longer periods, but a requirement for longer recording periods would be less practical in clinical settings.
Bland-Altman plots revealed the presence of some systematic bias toward an increase in mean crackle 2CD (“coarser” crackles) after intervention in recordings made at anterior and lateral chest regions. Crackles heard here post intervention may therefore originate from more central airways, since smaller airways are believed to produce fine, late inspiratory crackles, whereas larger airways tend to produce coarser, earlier crackles.28 A movement of crackles to more central airways may arise as a result of forced expiratory maneuvers moving secretions and allowing more air to pass. The association between crackle classification (fine vs coarse) and the location in the airways of their generation has been previously investigated by Fredberg and Holford,29 and has been put on a firmer basis by Majumdar et al.30
Although CALSA has not previously been used as an outcome measure for therapeutic interventions, it has been reported that it can detect changes during the course of pharmacologically induced airway obstruction,31 during forced expiratory maneuvers,32 and during pathological processes such as pneumonia.6,33 Baughman and Loudon5 recorded lung sounds in asthma patients overnight and were able to detect degrees of obstruction severity not revealed by any other measure. CALSA may therefore provide a more sensitive measure to detect alterations in airway geometry than conventional outcome measures.
Devices that record and analyze wheezes are already in clinical use (eg, Wheezometer, Karmel Sonix, Haifa, Israel), but the technology for instant crackle analysis clinically at the bedside is not yet commercially available. The aim is to produce a simple, reliable device that can record and analyze sounds at the bedside to provide clinicians with immediate information about a patient's lung health. This would provide objective information not only in terms of whether an individual was improving, stable, or deteriorating in relation to previous recordings, or in response to an intervention, but also in relation to normative data (similar to comparisons for lung function data). Before this can be achieved, there is further work to be done in terms of validation studies (eg, against expert opinion and objective imaging data), and further work on the signal processing techniques to provide real-time automated analysis. The main cost at present is in relation to the research and development required. Once a commercial system is available, further health economic evaluations will be required to determine the cost-benefit or otherwise of implementing such technology in clinical practice.
Conclusions
Respiratory therapy urgently needs robust outcome measures to monitor and evaluate effectiveness and to produce an evidence base. Lung sounds contain a wealth of clinically useful information that has the potential to be used to evaluate treatment. To our knowledge, this study is the first to estimate change in the number and duration of specific adventitious lung sounds (ie, crackles) after a therapeutic intervention. Mean nBC did not change, but mean 2CD did change within individuals. We have previously reported that the 2CD is a stable and reliable measure over short periods of time.7 The findings of this research therefore provide further indication that 2CD has potential for application as a new individual outcome measure in respiratory clinical practice.
Acknowledgments
The authors would like to thank Prof Paul White, University of Southampton, Highfield, Southampton, United Kingdom, for useful discussions regarding this study. We are also very grateful to all the participants for their involvement and to the staff of the Respiratory Center at Queen Alexandra Hospital, Portsmouth, United Kingdom.
Footnotes
- Correspondence: Alda Marques PhD MSc PT, School of Health Sciences, University of Aveiro, Campus de Santiago, Edifício III, 3810–193 Aveiro, Portugal. E-mail: amarques{at}ua.pt.
This research was partially supported by Fundação para a Ciência e Tecnologia, Portugal (ref. SFRH/BD/21375/2005).
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}