

Abstract
The diagnosis of brain death is a complex process. Strong knowledge of neurophysiology and an understanding of brain death etiology must be used to confidently determine brain death. The key findings in brain death are unresponsiveness, and absence of brainstem reflexes in the setting of a devastating neurological injury. These findings are coupled with a series of confirmatory tests, and the diagnosis of brain death is established based on consensus recommendations. The drive to breathe in the setting of an intense ventilatory stimulus (ie, respiratory acidosis) is a critical marker of brainstem function. As a consequence, apnea testing is an important component of brain death assessment. This procedure requires close monitoring of a patient as all ventilator support is temporarily removed and Paco2 levels are allowed to rise. A “positive” test is defined by a total absence of respiratory efforts under these conditions. While apnea testing is not new, it still lacks consensus standardization regarding the actual procedure, monitored parameters, and evidence-based safety measures that may be used to prevent complications. The purpose of this report is to provide an overview of apnea testing and discuss issues related to the administration and safety of the procedure.
Introduction
The concept of brain death was first described in the medical literature in 1959, and was an attempt to separate the cessation of meaningful neurological function from the cessation of cardiorespiratory function.1 The rationale for this distinction was that the former represented human existence, while the latter was viewed simply as biological existence. However, despite more than half a century of the general acceptance of brain death as a medical concept, clear consensus regarding brain death determination is still lacking.2 In general, the declaration of brain death usually requires that the cause of brain injury is known, the irreversibility of the injury is certain, and important neurological signs of brain function are absent.
The recognition of confounding factors, proper interpretation of appropriate neurologic imaging, and performance of any confirmatory examination and testing should be considered when determining brain death. Medical conditions possibly complicating the clinical assessments include severe acidosis/alkalemia, body temperature irregularities, drug intoxication, poisoning, neuromuscular blockade, and a locked-in syndrome. These circumstances must be considered before brain death determination can proceed. It is also important to understand some neurologic states can mimic brain death.3
Brain Death Physiology
Brain death was defined in 1995 by the American Academy of Neurology as the irreversible cessation of function of the brain, including the brainstem.4 Two clinical findings are necessary to confirm this irreparable condition of the brain: coma (with a known cause), and absence of brainstem reflexes. The cause of brain death itself is variable, and can be a result of traumatic events or numerous medical conditions. Brain death may be frequently seen as a consequence of aneurysmal subarachnoid hemorrhage, intracerebral hemorrhage or infarct, cardiac arrest, and severe head injury. Regardless of the primary insult to the brain, tissue death occurs from brain anoxia by one of several mechanisms: severe blood hypoxemia (ie, lethal reductions in nutrient or oxygen blood content); severely impaired perfusion (eg, widespread edema, elevation of intracranial pressure; the cessation of blood flow to the brain and brainstem); or toxic neuronal injury.
Cerebral blood flow is particularly important when considering a diagnosis of brain death. Reduction of blood flow to the brain is usually created when the intracranial pressure is greater than the mean arterial pressure, thus lowering the cerebral perfusion pressure to a point that sufficient blood flow into the brain ceases. This lack of blood flow to the brain usually results in widespread cell anoxia and death. While this physiologic mechanism is considered the most devastating, it is not the only one described. Another pattern is characterized by intact cerebral blood flow, which should adequately deliver oxygen, glucose, and other nutrients to the brain at sufficient levels to sustain tissue life. However, in this pattern an intrinsic catastrophic event occurs at the cellular level, which prevents extraction or utilization of the oxygen and nutrients needed to maintain cellular function and metabolism. Examples include cyanide poisoning and other metabolic derangements. This mechanism results in lack of oxygenation to the brain, not by failure of the delivery system, but from end organ breakdown of the brain, at the capillary or tissue level.5
Ethical and Legal Issues
Historically, brain death and cardiorespiratory death often occurred together. However, the use of mechanical ventilation to prevent respiratory arrest, in conjunction with the improvement of blood pressure management, has transformed the course of terminal neurological disorders. Cardiorespiratory functions can now be mechanically maintained after the brain has ceased to function. This has led to ethical debates about the definition of brain death and the concept of human death. The American Academy of Neurology's definition of brain death is considered the accepted medical definition. However, it is important to understand that brain death essentially has 2 definitions: one is medical and the other is legal. The legal definition is set by the individual states, which are responsible for defining “death” for legal reasons.
Beyond medical definitions and considerations, cultural and regional acceptance of death varies and must be addressed. For example, some cultures and religions do not accept death until after all vital functions of the body have ceased.1 Many, regardless of culture or religion, may find it very difficult to accept death when the heart and lungs appear to still be living, although being completely supported by mechanical and pharmacologic means. However, when brain death is determined and documented, many states no longer require the continuation of cardiorespiratory life support. The decision to withdraw cardiorespiratory life support based on the concept of brain death may be difficult for many caregivers and family members. The clinical staff is responsible for clearly defining and communicating the process to those involved in patient decision making.
Individual hospitals are typically responsible for creating written policies to clearly specify the process of determining brain death. These may include a description of the examinations and diagnostic tests, and which individuals should be present to make the conclusion. Published guidelines for establishing brain death are available (Table 1).6 The evidence supporting these guidelines is not robust, and it is noted that some data supporting these recommendations are inadequate or conflicting.6
Brain Death Guidelines
Determining Brain Death: The Role of Apnea Testing
Apnea testing is an essential component in the clinical determination of brain death.6,7 The main objective of apnea testing is to prove the absence of respiratory control system reflexes in the brainstem when intense physiologic stimulation to breathe takes place. In the case of apnea testing, the stimulus is the rapid increase in the Paco2 to > 60 mm Hg (or a 20 mm Hg increase in Paco2 over baseline normal Paco2), and the corresponding decrease in pH before buffering mechanisms can occur.6,8
Because of the potential implications involved in the diagnosis of brain death, it is essential that apnea testing be safe, accurate, and reproducible. This not only serves the clinicians who are tasked with diagnosing brain death, but also allows family members of patients to rest more assured that the decisions regarding end of life issues were made with sound, informed, and proper judgment. The outcome of an apnea testing is very straightforward. A negative test is defined by any spontaneous respiratory efforts in response to hypercapnic/acidotic stimulation; a positive test is the absence of any respiratory activity under these conditions.
Wide practice variability exists in regard to apnea testing. A survey of respiratory therapists illustrated some of these variations, revealing disparities in both monitoring and methods (Table 2).9 There are potentially several reasons for different standards. Apnea testing is a low volume procedure. For example, large tertiary care hospitals may diagnose brain death only 25–30 times per year.10 The only universal agreement among surveyed participants was that respiratory therapists were to be present during all apnea tests. Recently, the apnea testing itself and its utility have been questioned.11,12 Also, substantial discussion among organ procurement organizations and clinicians has been provoked, due to the suggestion that only one clinical exam, along with the apnea test, may be enough to adequately and reasonably diagnose brain death. This further emphasizes the need for well designed studies involving the safety, efficiency, and effectiveness of the various methods of apnea testing.
Survey of Clinical Practice of Apnea Brain Death Assessment
Complications of Apnea Testing
In order to be considered a useful tool in the determination of brain death, apnea testing must be rigorous enough to reliably demonstrate apnea and brainstem death without causing further organ damage.13 Thus, care must be taken to avoid iatrogenic injury during apnea testing. Complications associated with apnea testing include hypoxemia, hypotension, acidosis, hypercapnia, increased intracranial pressure, pulmonary hypertension, and cardiac arrhythmias (Table 3).14–20 Cases of cardiac arrest and pneumothorax have also been reported.21
Apnea Test Studies
Certain complications can be considered inherent, due to the nature of the test itself. For example, some degree of respiratory acidosis and hypercapnia will be present if the patient is indeed apneic and carbon dioxide production in the body continues. While this is an expected response, the clinicians performing the study must be aware of the potential for severe acidemia and possible deleterious side effects. Carbon dioxide and acidemia cause peripheral vasodilation and cardiac depression, frequently resulting in hypotension, which is one of the most common complications of apnea testing.17,22,23 The impaired autonomic reflexes found in many of these patients increase the potential for blood pressure problems. Hypoxemia during apnea testing further increases the potential risk for cardiac dysrhythmias and hypotension. Appropriate precautionary steps, such as pre-oxygenation with 100% oxygen, are essential to prevent hypoxia during apnea testing, should be used, and have been shown to be effective.14,17
Other very serious complications of the apnea test have also been noted. Burns and Russell reported a case in which their patient developed a tension pneumothorax, pneumomediastinum, and pneumoperitoneum as a result of airway perforation from the oxygen catheter.24 Bar-Joseph et al also reported 2 cases of tension pneumothorax that they concluded were the result of massive air trapping beyond a cannula that was obstructing the airway.25 In the cases presented, both patients subsequently deteriorated rather quickly: one patient expired immediately after a cardiopulmonary resuscitation attempt; the other expired shortly after the condition was stabilized and was confirmed brain dead one hour later. Additionally, in the latter case the heart and lungs were damaged severely and were unable to be used for transplantation. The authors recommended use of a markedly smaller cannula than the inner diameter of the endotracheal tube during the apneic oxygenation procedure, to prevent air trapping. They concluded with a recommendation that all guidelines for the determination of brain death contain detailed instructions regarding the safe performance of apnea testing, ensuring adequate oxygenation and the prevention of inadvertent pneumothorax.
Methods of Performing Apnea Testing
Various methods to carry out apnea testing procedures vary from institution to institution, yet a core set of procedural elements are common (Table 4). Immediately before all apnea tests, an initial arterial blood gas sample should be obtained to establish baseline Paco2 levels. This information will be useful when making the final determination of whether or not the increase in arterial carbon dioxide/corresponding decrease in pH have occurred.
Apnea Testing Guidelines
A common method of apnea testing involves disconnection of mechanical ventilation from the patient, followed by the insertion of a catheter or cannula into the endotracheal tube, down to the level of the carina, through which oxygen is delivered.4,10,26 Disconnection from mechanical ventilation is thought to prevent erroneous ventilation readings by the ventilator itself. This is termed the apneic oxygenation method. Oxygen flow is usually 4–10 L/min.6 This flow ensures adequate delivery of oxygen to the blood through gas displacement in the upper bronchial tree, and diffusion to the alveoli, even in the absence of respiratory movement.
The duration of time of mechanical ventilation disconnection needs to be sufficient to raise the Paco2 to > 60 mm Hg. Current guidelines for apnea testing state that measurement of the blood gas should be conducted after approximately 8–10 min.6 However, relying on fixed durations, which are based upon the expected rise in Paco2 with apnea (3–4 mm Hg/min under normal physiologic conditions), may yield variable results, as the relationship of Paco2 and CO2 production may vary greatly under conditions of terminal illness and brain death.27 Because of this, the apnea testing may be continued until the arterial blood gas results are noted, as long as the patient remains hemodynamically stable and with an adequate Spo2. Continuing the apnea test for slightly longer periods (eg, up to 15 min) may be preferable to repeating the test. Additionally, CO2 elevation and elimination may be skewed by the oxygen flow via a catheter placed in the endotracheal tube. There are modifications of the apneic oxygenation method that serve to refine and streamline apnea testing. Benzel et al modified their protocol by initially reducing mechanical ventilation settings to allow for a higher initial Paco2 at baseline. This was shown to reduce the amount of time required to reach the desired goal of 60 mm Hg.14 As in other studies, they also noted that the rate of Paco2 elevation varies considerably from patient to patient, regardless of baseline Paco2.
Different technical variations of the apneic oxygenation technique for apnea testing have also been described. T-piece systems used to provide oxygen via standard corrugated tubing connected to 100% oxygen at a flow of 12 L/min have been shown to be as effective as the previously described oxygen cannula technique.19 This method of apnea testing may theoretically be safer than the intratracheal catheter method, since the possible risk of increased intrathoracic pressure or pneumothorax would be lower. The investigators further modified their T-piece approach with corrugated tubing technique, with a 10 cm H2O CPAP valve attached to the distal extremity of the T-piece extension to enhance oxygenation.19
Additional methods that allow the patient to stay connected to a mechanical ventilator circuit until the final phase of the apnea testing have been described. In one method, hypoventilation is achieved by reducing the minute ventilation to a low level and keeping the patient on the ventilator until the required Paco2 is attained. At this point the ventilator is disconnected. The authors recommend the patient be observed during this disconnection period for any respiratory movements, suggesting that 30–60 seconds is an adequate amount of time to observe for apnea.14 A modification of this method allows the patient to remain connected to the ventilator circuit in order to provide an elevated CPAP while the ventilator supplies no breaths.28
Artificial augmentation of Paco2 levels has also been considered an option for apnea testing.14,17,29,30 This method involves the exogenous administration of CO2 into the ventilator circuit to achieve the desired Paco2 level during the apnea testing. Different mixtures of oxygen/carbon dioxide (eg, 10% CO2, balance O2), sometimes referred to as carbogen, may be used to achieve these desired levels. The delivery of carbogen may be accomplished by utilizing a bag-valve system attached to the tank, or by attaching the tank to the ventilator itself.29,31 Other means of delivering CO2 have been described, such as the administration of pure CO2 into the inspiratory limb of the ventilator, without modifying other parameters such as the Fio2.8 The obvious advantage of providing CO2 in the ventilator circuit is that the desired Paco2 level can be reached very quickly, and thus the risks associated with hypoxemia are minimized. The procedure is generally monitored with an exhaled CO2 analyzer; when the desired level is reached (eg, a 20 mm Hg increase), the ventilator is either disconnected or switched to CPAP and the patient is monitored for 1–2 min for respiratory efforts.
All of the above apnea testing procedures have a simple common goal: elevate Paco2 and observe the patient for any spontaneous respiratory effort to reflect brainstem activity. It must be emphasized that spontaneous respiratory efforts may be subtle, so very close observation of the patient's chest and abdomen with an unobstructed view is essential. Further study to determine if one method is more safe, effective, and reproducible is warranted in order to establish guidelines to be used by both the expert and the novice clinician.
Monitoring/Precautions During Apnea Testing
Continuous patient monitoring during apnea testing is imperative. Due to the very nature of the clinical condition of the patient, apnea testing is most likely performed in a critical care area where monitoring and close patient supervision are provided. Physiologic parameters, including heart rate/rhythm, arterial blood pressure, exhaled CO2, and Spo2, should be continuously evaluated before, during, and after the apnea testing. Taking precautionary steps prior to apnea testing, such as ensuring normotension (eg, adequate intravenous access and intravenous vasopressor agents) and adequate pre-oxygenation, may be warranted to prevent complications. Goudreau et al found that cardiovascular complications were noted in approximately 1 in 4 apnea tests.17 This rate nearly doubled in tests performed in patients with unstable or borderline baseline blood pressure or Spo2. The authors emphasized that a majority (85%) of apnea testing can be performed without complications when adequate precautions are taken. Clinicians need to be educated on the complexities of apnea testing, and efforts need to be made to improve on the proper execution of apnea testing to reduce the risk of complications.
Supplementary monitoring with transcutaneous CO2 monitoring during the apnea testing procedure may be considered (Fig. 1). Transcutaneous CO2 monitoring has been reported to prevent excessive hypercarbia/respiratory acidosis resulting from the apnea testing procedure. Vivien et al, in a cohort study evaluating the use of transcutaneous CO2 monitoring in brain death determination, found that it accurately predicts when the Paco2 goal has been attained.13 Lang et al also reported a strong correlation between transcutaneous CO2 and Paco2. They suggested this modality was effective at reducing CO2 target overshoot during exogenous CO2 administration.21 It is important to note that the Paco2 sampling level, confirmed by arterial blood gas measurement, is the accepted standard.
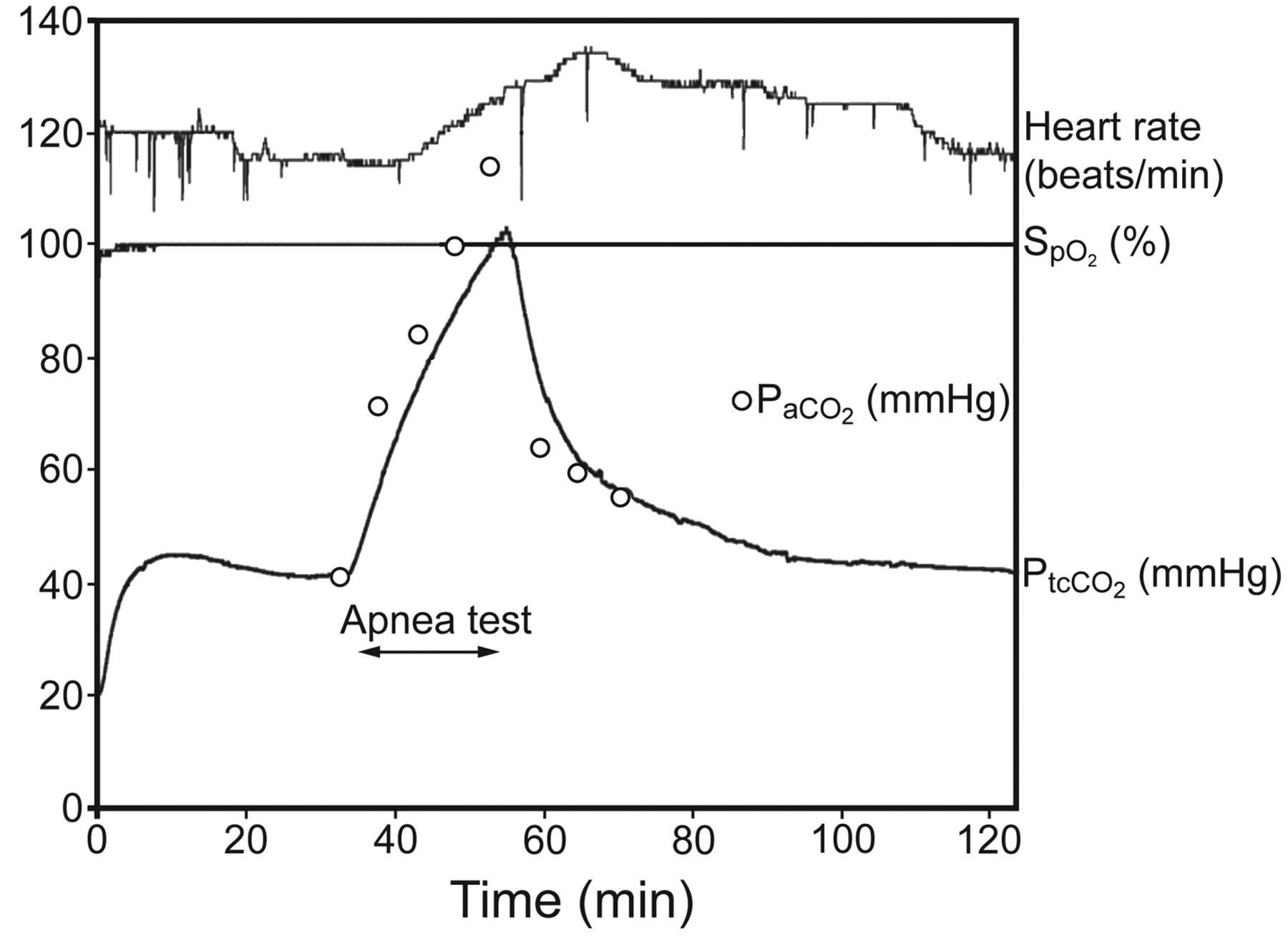
Representative tracings of transcutaneous CO2 (PtcCO2), Spo2, and heart rate during an apnea test designed to raise Paco2 to 100 mm Hg. At baseline, PtcCO2 is very close to Paco2, but exhibits a delay during the rapid increase of Paco2 during apnea. After reconnection to the ventilator, PtcCO2 becomes closer to Paco2, as the rate of decrease in Paco2 was reduced. (From Reference 13, with permission.)
Summary
Apnea testing is an integral component in brain death determination. Several attempts have been undertaken to better understand the best practice methods regarding the apnea testing. Most experts in the field of brain death determination consider apnea testing essential, but widely accepted guidelines and parameters, including detailed instructions regarding the procedure itself, do not yet exist. The safety and reliability of apnea testing are common themes when reviewing available literature. Debate continues regarding the specific parameters to be desired, met, and maintained. All known methods of apnea testing have yet to be fully scrutinized, although recommendations regarding their use have been published.
Footnotes
- Correspondence: J Brady Scott RRT-ACCS, Respiratory Care Services, Rush University Medical Center, 1620 West Harrison Street, LL 1202.13, Chicago IL 60612. E-mail: Jonathan_B_Scott{at}rush.edu.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}