

Introduction
Lipoid pneumonia is an unusual form of pneumonitis. It is categorized as either exogenous or endogenous, depending on the lipid source. Diagnosis requires a high index of suspicion, with clues provided by history and characteristic radiographic findings. Evaluation of samples obtained via bronchoscopy can confirm the diagnosis with oil red O staining, without requiring surgical biopsy. We report a case of exogenous lipoid pneumonia that resolved with conservative management. No clear synthetic source, such as mineral oil or petroleum jelly use, was identified, despite a thorough history. However, years of episodic dyspnea preceded by nausea and vomiting resolved with surgical repair of a large hiatal hernia suggest aspiration of food as the exogenous lipid source.
Case Summary
A 63-year-old woman presented with progressive dyspnea over 24 hours, with associated fever and cough productive of white sputum. Her symptoms were associated with nausea but without vomiting, abdominal pain, or diarrhea. She denied chest pain, arthralgias, myalgias, or rash. She had experienced these symptoms intermittently over many years, typically preceded by episodes of nausea and non-bloody emesis. However, this episode was more severe, and her symptoms were also worsening, prompting her to seek medical attention.
Past medical history was notable for a distant history of Hodgkin lymphoma, in remission, treated with radiation and splenectomy, hypothyroidism, leukocytoclastic vasculitis on biopsy of a skin rash, intermittent leukocytosis, gastroesophageal reflux disease, and depression. Review of systems was otherwise unrevealing. She did not smoke, drink alcohol, or use illicit drugs. There was no important travel or exposure history. Family history was unremarkable. She had no allergies. Medications included levothyroxine, esomeprazole, vitamin D, escitalopram, and tolterodine.
Vital signs were notable for a temperature of 38°C, blood pressure 99/66 mm Hg, with a pulse of 74 beats/min, breathing frequency of 22 breaths/min, and a peripheral oxygen saturation of 84%. Physical exam revealed crackles, most prominent at the mid portion of her left lung field. Cardiac exam was regular, without murmurs. Abdominal exam was unremarkable other than a well healed surgical scar. Her extremities were without edema and there were no rashes.
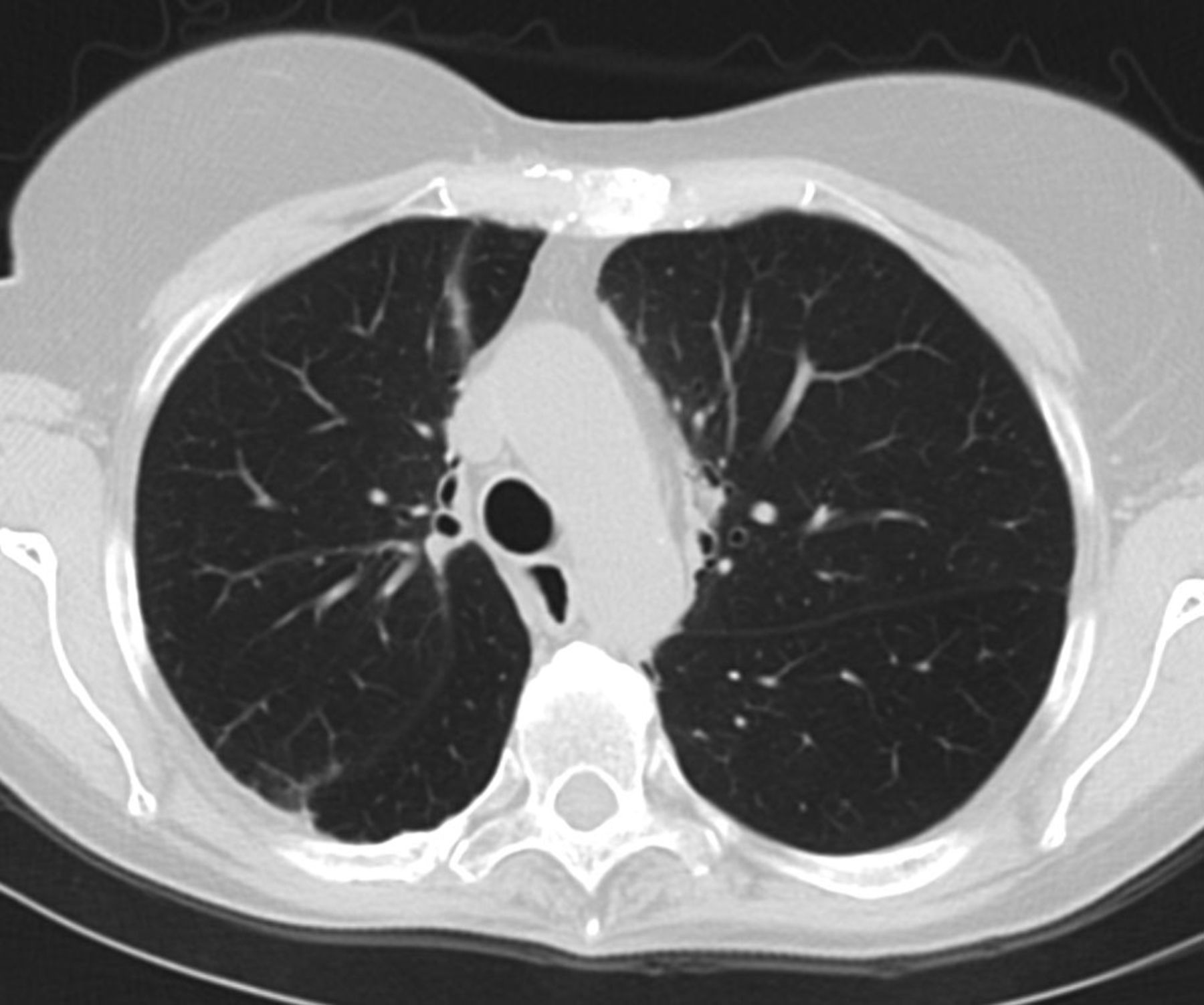
Initial laboratory studies revealed a leukocytosis of 19.18 × 103/uL, with a neutrophilic predominance of 80%, arterial blood gas showing pH 7.42, Paco2 38 mm Hg, and Pao2 55 mm Hg, troponin 0.05 ng/mL, brain natriuretic peptide 105 pg/mL, and d-dimer 519 ng/mL. The remainder of the complete blood count, chemistry panel, and coagulation panel was within normal limits. Electrocardiogram demonstrated a normal sinus rhythm, and serial troponins were negative. Chest radiograph demonstrated patchy air space disease in the mid and lower left lung fields (Fig. 1). She was admitted for community-acquired pneumonia. Her symptoms persisted, with continued fever and requiring supplemental oxygen at 2 L/min via nasal cannula after 3 days of levofloxacin and the addition of piperacillin/tazobactam. Computed tomography (CT) of the chest demonstrated bilateral central ground glass and consolidative opacities in the left upper lobe, and perihilar right upper lobe in a “crazy paving” pattern (Fig. 2). The left lower lobe also demonstrated less confluent multifocal ground glass opacities, in addition to a large hiatal hernia.
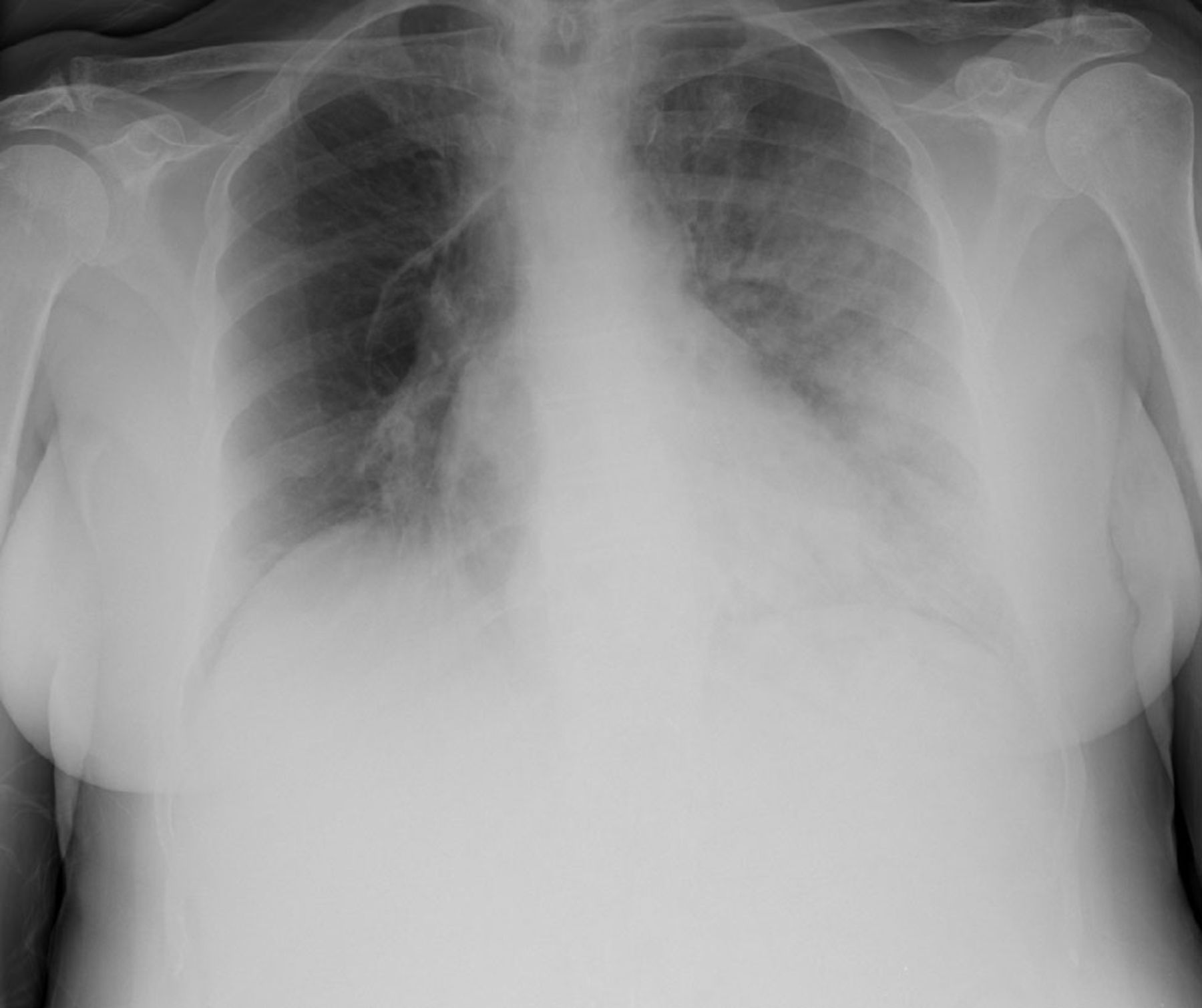
Initial chest radiograph demonstrating patchy air space disease in the middle and lower left lung fields.

Computed tomogram chest demonstrating bilateral central ground glass and consolidative opacities in the left upper lobe and perihilar right upper lobe.
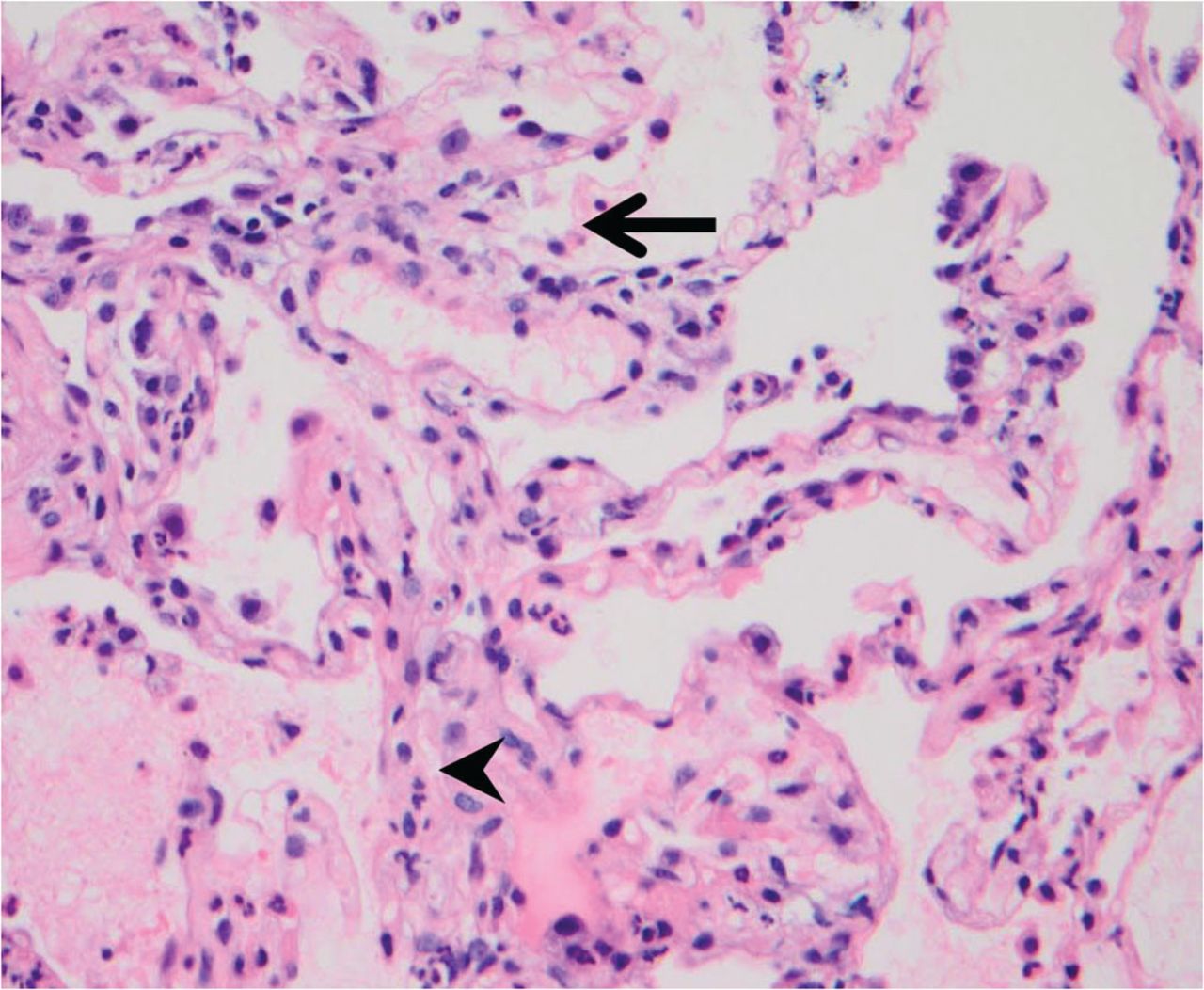
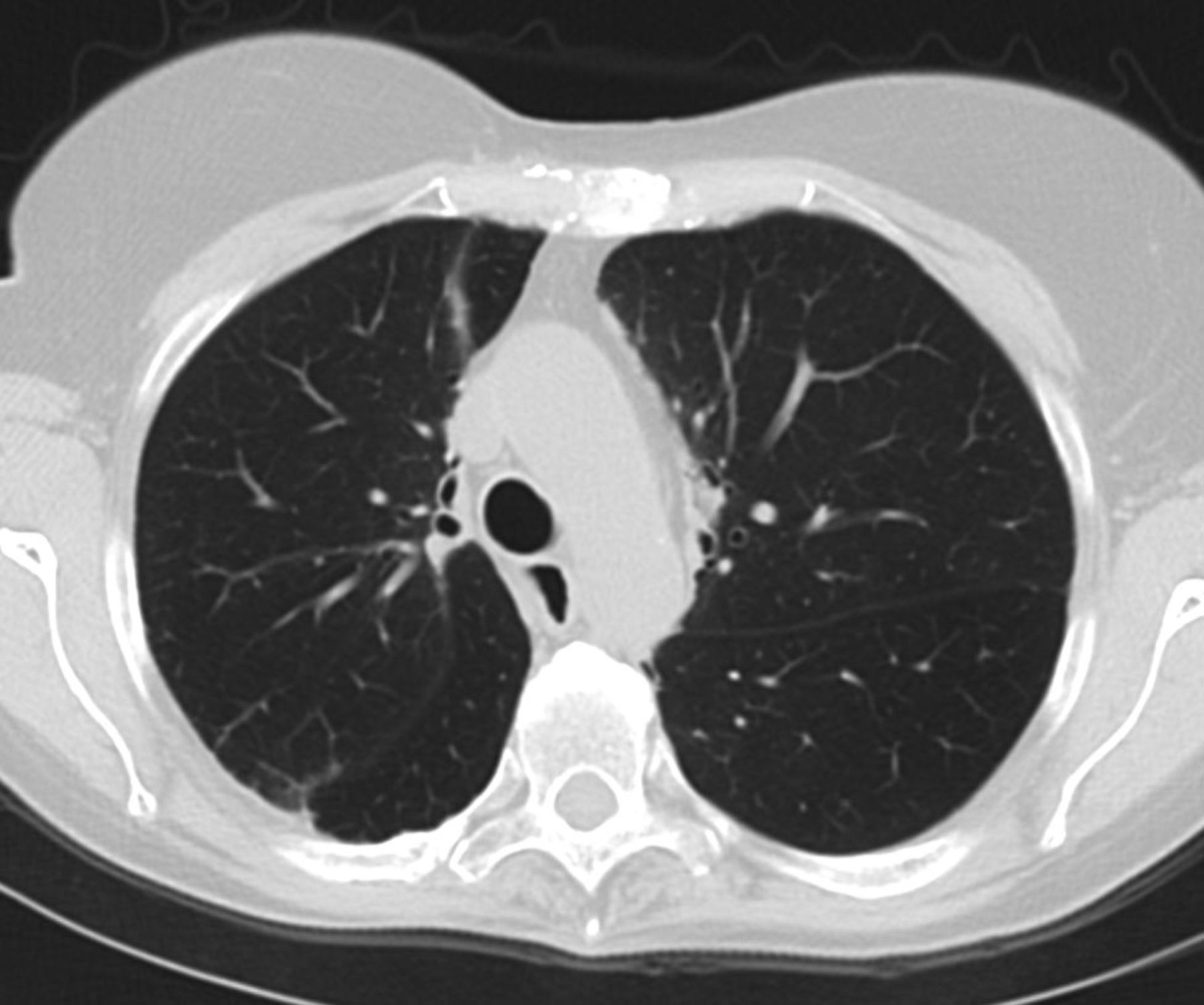
Bronchoscopy was performed with bronchoalveolar lavage (BAL) and transbronchial biopsies. Microbiologic studies for bacterial, fungal, mycobacterial, and viral pathogens were negative. Acute interstitial inflammation and foamy histiocytes were seen on transbronchial biopsies (Fig. 3). BAL cytology demonstrated numerous lipid-laden macrophages that stained oil red O positive consistent with exogenous lipoid pneumonia (Fig. 4). Antimicrobials were de-escalated, and a course of azithromycin was completed. By the time of discharge her symptoms, leukocytosis, and oxygenation had normalized. Given her history of recurrent episodes of dyspnea preceded by nausea and vomiting, the patient underwent surgical repair of her hiatal hernia. CT of the chest at 3 months demonstrated near total resolution of her air space disease (Fig. 5), and at a 1 year follow-up she reported no further episodes of nausea, vomiting, or dyspnea.

a. Transbronchial biopsy demonstrating acute interstitial inflammation (arrow) and foamy histiocytes (arrowhead).

Bronchoalveolar lavage demonstrating lipid laden macrophages highlighted by oil red O staining.
Computed tomogram chest 3 months after initial presentation demonstrating resolution of initial findings.
Discussion
Lipoid pneumonia was first described in 1925 by Laughlin and was relatively common prior to the ban of oil based nasal drops in 1942.1 Although much rarer since the ban, oil based products continue to be the primary causative agent of the disease. Oil is easily aspirated, as it elicits only modest cough and is difficult to clear by mucociliary mechanisms. Accumulation in combination with an inflammatory reaction to aspirated lipids leads to the clinical findings of lipoid pneumonia.
There are 2 types of lipoid pneumonia, based on the source of the lipid: exogenous, as seen in the presented case, and endogenous. Exogenous lipoid pneumonia, as the name suggests, usually occurs when an oily substance reaches the alveoli through aspiration or inhalation. Animal oils cause intense inflammation, while vegetable and mineral oils result in a more smoldering presentation. Mineral and vegetable oils are less likely to cause an immediate inflammatory response, but with chronic use can result in a foreign body reaction.2 Specifically, these substances are consumed by macrophages which ultimately congest the alveolar and interstitial space, leading to inflammatory cellular infiltration and variable fibrosis.3,4
The most common offending agent is mineral oil, also known as paraffin, due to its popularity as a laxative. Other sources include olive oil, shark oil, petroleum jelly, and endemic herbal remedies.1,2,5–8 Advanced age, a debilitated state, or neurologic conditions impairing the swallow or cough reflex increase the risk of lipoid pneumonia, presumably by increasing the risk of aspiration of these substances.5 In addition, structural abnormalities of the pharynx and esophagus, which cause pooling of food and gastric contents, have been well documented to be associated with lipoid pneumonia. These abnormalities include but are not limited to Zenker diverticulum, gastroesophageal fistula, hiatal hernia, gastroesophageal reflux disease, Chagas induced mega-esophagus, and achalasia.9–12 Because lipids tend to overlay water and gastrointestinal fluids in static situations, these conditions are thought to make one more vulnerable to chronic aspiration of fats and oils. In the presented case, although no classic source of lipid, such as paraffin, was identified by history, it is thought that the patient suffered from chronic aspiration, due to her large hiatal hernia, thereby predisposing her to lipoid pneumonia.
Endogenous lipoid pneumonia, which comprises a minority of cases, occurs when lipid containing materials are released from degenerated alveolar cells in the setting of impaired means of clearance. This can happen as a result of airway obstruction from diseases such as lung carcinoma, abscess, or severe bronchiectasis.2,5 Endogenous lipoid pneumonia has also been associated with lipid and glycogen storage disorders.13,14
The presentation and natural history of lipoid pneumonia are variable. Many individuals are asymptomatic and only diagnosed when an abnormality is seen on routine chest radiograph.5 Others may present with cough or dyspnea, similar to the presented case. Rarer symptoms include fever, weight loss, chest pain, sputum production, hemoptysis, digital clubbing, and wheezes or rales on exam.9 In general, elderly patients have a more chronic and indolent course, while younger patients may present with acute clinical decompensation and hypoxia.15 Duration between time of exposure and symptoms is highly variable and may range from days to years.9 If left untreated, patients may develop chronic bronchiectasis and pulmonary fibrosis.16 As a result of this, there have been case reports of cor pulmonale seen in end stage lipoid pneumonia.17 Hypercalcemia is an unusual manifestation of the disease, but can be seen due to granuloma formation from aberrant macrophage congregation.18
Diagnosis of lipoid pneumonia may be challenging. Laboratory findings such as leukocytosis with neutrophil predominance, elevated erythrocyte sedimentation rate,9 and imaging studies are often nonspecific. As such, diagnosis relies on a combination of high clinical suspicion, compatible radiographic studies, and analysis of sputum, BAL, or tissue samples.
Chest radiographs most commonly exhibit air space consolidation. However, reticular patterns, mixed alveolar and interstitial patterns, nodular patterns, and the appearance of mass lesions have been described.2 CT scans may demonstrate alveolar consolidation, ground glass opacities, interstitial abnormalities, and nodular lesions. Mass or consolidation with the low attenuation of fat (−30 to −150 Hounsfield units) is highly suggestive of lipoid pneumonia.19,20 CT images demonstrating vessels within and around an area of consolidation and the “crazy paving pattern,” which is a superimposition of a ground glass opacity over a reticular pattern due to interlobular septal thickening, have also been described.2,19–21 Use of magnetic resonance imaging and positron emission tomography have been reported, but with mixed results.20,22
BAL or sputum cytology provides key diagnostic data. The presence of lipid-laden macrophages detected by oil red O staining is highly suggestive of lipoid pneumonia.23 It is important that this stain be done on samples prior to being paraffin imbedded, as this process dissolves lipids.
There are no studies in the literature delineating the best therapeutic options. As such, supportive respiratory care, as well as identification and withdrawal of the offending agent, is crucial in cases of exogenous lipoid pneumonia.2,5 In acute cases, symptoms often resolve spontaneously, and imaging abnormalities are usually reversible if the offending agent is removed. However, in more indolent cases fibrotic changes may be permanent and lead to loss of lung function despite appropriate supportive care. Although symptoms and radiographic changes may resolve in months, expectoration of lipids may continue for years.15,16 Anecdotal use of corticosteroids has been reported. Theoretically, systemic corticosteroids would be useful in reducing or slowing the inflammatory response caused by macrophage activation. However, as there have been no randomized controlled trials, their use should be limited to severe cases, given the risk for side effects, including immunosuppression and infection.24 Whole-lung lavage, as used in patients with alveolar proteinosis, has been reported, but its benefit is unclear at this time.2,5,14,24,25 There is some thought that lipid phagocytosis by macrophages may make removal by bronchial lavage of limited use.26 Lastly, surgical lung resection has been proposed in patients who develop severe bronchiectasis. This should only be undertaken if they do not respond to aggressive medical therapy.27
Complications, though rare, may occur, and can include superinfection with bacteria, atypical mycobacteria, and cryptococcus.28–31 Reports of coexisting carcinoma have also been documented. One case of nonfatal but massive hemoptysis has been described.32
Teaching Points
Exogenous lipoid pneumonia is a relatively uncommon disease and requires a high clinical suspicion for diagnosis. Its presentation is nonspecific and often mimics both more and less common disease states such as pneumonia, pulmonary fibrosis, and lung cancer. As such, it should be considered as a potential diagnosis in patients with a compatible history, particularly where standard treatment for a presumed diagnosis does not yield an expected clinical response.
Key diagnostic clues include a history of regular use of lipid containing substances such as mineral oil or petroleum jelly. Radiographic findings can provide important clues, and include a pattern of “crazy paving” and low attenuation air-space disease with Hounsfield units in the range of −30 to −150, consistent with fat.
Tissue confirmation can be obtained by bronchoscopy with oil red O staining of samples, including BAL and transbronchial biopsies. Red oil O staining must be done prior to paraffin embedding, as this process dissolves lipids.
The overall prognosis of exogenous lipoid pneumonia is good, but it can cause irreversible fibrosis. Occasionally steroids may be warranted if abnormalities persist despite withdrawal of the offending agent.
Footnotes
- Correspondence: Scott S Oh DO, Division of Pulmonary and Critical Care Medicine, David Geffen School of Medicine at UCLA, 1233 16th Street, Suite 3400, Santa Monica CA 90404. E-mail: ssoh{at}mednet.ucla.edu.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}