

Abstract
BACKGROUND: Pneumonia is a common comorbidity among hospitalized older adults and may impede functional restoration and increase medical cost. Medicare reimbursement rates for patients receiving in-patient medical rehabilitation services are higher for individuals who have comorbid pneumonia. We examined the impact of comorbid pneumonia on outcomes for patients with lower extremity fracture receiving in-patient medical rehabilitation services.
METHODS: Secondary data analysis of medical records obtained from 919 in-patient rehabilitation facilities in the United States. The sample included 153,241 subjects who received in-patient rehabilitation services following lower extremity fracture in 2005–2007. We used multivariable linear regression to evaluate the independent effects of pneumonia on stay and discharge functional status (Functional Independence Measure instrument), and logistic regression models to explore discharge to home versus not home.
RESULTS: Pneumonia was a comorbidity for 4,265 (2.8%) of the subjects with lower extremity fracture. The multivariable models indicated that subjects with no payment-eligible comorbidity experienced shorter stay (regression coefficient −0.44, 95% CI −0.60 to −0.28 d), higher discharge functional status ratings (regression coefficient 1.84, 95% CI 1.42–2.25 points), and higher odds of home discharge (odds ratio 1.19, 95% CI 1.09–1.29), compared to subjects with pneumonia.
CONCLUSIONS: Our findings suggest that comorbid pneumonia is associated with poorer rehabilitation outcomes (stay, discharge functional status, and discharge setting) among subjects receiving in-patient rehabilitation services for lower extremity fracture.
Introduction
Lower extremity fractures (hip fractures, in particular) are a common reason for hospitalization in older adults and are associated with high morbidity and mortality.1 These fractures often occur in older adults who have comorbid conditions (eg, diabetes).1 Comorbidities can affect the recovery process and lead to longer stay and a lower likelihood of returning home.2
Pneumonia is a potential complication in older adults who experience a hip fracture or other lower extremity factures and are receiving in-patient medical rehabilitation.3 Pneumonia can compound disability, inhibit functional restoration, and increase medical costs. In 2002 the Centers for Medicare and Medicaid Services (CMS) introduced a prospective payment system for in-patient medical rehabilitation facilities, to help control costs.2 Rehabilitation facilities receive reimbursement based on projected resource use (costs) for a given patient. The rate is determined by the patient's primary medical diagnosis, age, and level of functional status at admission.4–6 Each patient is assigned to a case-mix group, which is used to establish the prospective payment rate.7 The base rate can be adjusted based on several factors, including the presence of comorbid conditions that likely increase the resources needed to attain a desired level of recovery or independence.
Medicare's comorbidity payment system consists of a 4-tier classification: tier 1 represents high cost, tier 2 represents medium cost, tier 3 is for low cost, and the final tier level includes patients with no payment-eligible comorbidities (non-tier).5 Little research has been done to examine the validity of specific condition-comorbidity combinations within the CMS comorbidity tier classification system.
The purpose of our study was to examine the impact of pneumonia as a comorbidity for patients with lower extremity fracture (hip, pelvis, or femur) who received in-patient medical rehabilitation services following acute care hospitalization. We examined stay, discharge functional status, and discharge setting (home vs not home). This information is relevant to establishing the validity of the comorbidity tier system developed by CMS.
QUICK LOOK
Current knowledge
Pneumonia is a common complication among hospitalized older adults with lower extremity fractures and may slow rehabilitation and increase costs. Medicare reimbursement rates for patients receiving in-patient medical rehabilitation services are higher for individuals who have pneumonia.
What this paper contributes to our knowledge
Patients who received in-patient rehabilitation following lower extremity fractures and who had comorbid pneumonia had longer stay and poorer functional status, and were less likely to be discharged home than patients without pneumonia.
Methods
Data Source and Study Sample
The data were obtained from 919 in-patient rehabilitation units and facilities that subscribed to the Uniform Data System for Medical Rehabilitation in 2005–2007.6 All information was derived from the items included in the In-patient Rehabilitation Facility-Patient Assessment Instrument (IRF-PAI).4,5 The IRF-PAI was developed by the CMS to determine eligibility for prospective payment, and includes 54 items. The sample included subjects receiving in-patient rehabilitation services for lower extremity fracture (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9] codes 820.0–820.9 and 821.0–821.3) during the 3-year study period. Approximately 85% of cases were hip fractures, 9% pelvis fractures, and 6% femur fractures. The initial sample contained 166,777 cases. Patients were excluded if the admission was not an initial rehabilitation stay (6,562), they were not between the ages of 20 and 100 years old (645), the duration from fracture to rehabilitation facility admission was > 30 days (5,183), or stay was > 30 days (1,146). The final sample contained 153,241 cases, representing 92% of the original cohort.
Dependent Variables
Stay.
Rehabilitation stay was recorded as the total number of days spent in the medical rehabilitation unit or facility.
Discharge Functional Status.
The functional status items in the IRF-PAI are from the Functional Independence Measure (FIM instrument),4 and include 18 items covering 6 domains: self-care, sphincter control, transfer, locomotion, communication, and social cognition. Items are scored on a 7-point scale, ranging from complete dependence (level 1) to complete independence (level 7) with a potential total score range of 18 to 126. Functional status ratings can be grouped into motor and cognition domains.4,6 The FIM items were administered by trained personnel within 36 hours of both admission and discharge. FIM ratings were used as a continuous variable in all analyses. The reliability, validity, and responsiveness of the functional status items have been widely investigated, with intraclass correlation coefficients consistently > 0.85.8
Discharge Setting.
The IRF-PAI contains 14 different discharge settings, including home, transitional care, skilled nursing facility, long-term care, and acute care hospital. For our analysis, discharge setting was dichotomized as home versus not home.
Independent Variable
The independent variable of interest was pneumonia comorbidity. It was coded as a dichotomous variable (yes/no) for descriptive summaries and combined with the 4-level tier variable to create 5 unique categories for the multivariable analyses. The IRF-PAI allows up to 10 comorbidity codes for each patient. Subjects with an ICD-9 code for pneumonia (480.0–487 or 506) within any of the 10 comorbidity variables were classified as positive for pneumonia. The primary diagnoses for these ICD-9 codes included: viral pneumonia; pneumococcal pneumonia; other bacterial pneumonia; pneumonia due to other specified organism; pneumonia in infectious diseases classified elsewhere; bronchopneumonia, organism unspecified; pneumonia, organism unspecified; influenza with pneumonia; and bronchitis and pneumonitis due to fumes and vapors. Within these primary diagnoses there are 30 sub ICD-9 code and diagnoses. In the Medicare prospective payment system for in-patient medical rehabilitation, all pneumonia ICD-9 codes are considered tier 3 comorbidities. Subjects with pneumonia who also had other tier 2 or tier 1 eligible comorbidities (eg, presence of tracheotomy) were coded as the latter, higher paying tier, for the multivariable analyses of rehabilitation outcomes.
Covariates
Sociodemographic variables included age in years, sex, race/ethnicity (black, white, Hispanic, other), and marital status (married, not married). Medical factors included sum of non-pneumonia comorbidities (range 0–10), duration to rehabilitation admission (days), admission or discharge functional status (FIM instrument ratings), and stay (days) in select models.
Statistical Analysis
Unadjusted descriptive summaries of subject characteristics and outcomes were stratified by pneumonia status and examined by univariate statistics (t tests and chi-square tests). We used multivariable linear regression to evaluate the independent effects of pneumonia on stay and discharge functional status. We used logistic regression to examine the dichotomous outcome of discharge to home versus not home. The 5-level pneumonia/tier variable was dummy-coded for inclusion in the multivariable models; pneumonia served as the reference category in all 3 models. We controlled for subject age, sex, race/ethnicity, sum of non-pneumonia comorbidities, and functional status (admission or discharge, as appropriate) in all 3 outcome models. Stay was included in both the discharge functional status and home discharge models, and marital status was added to the home discharge model as a proxy for social support. Lastly, we used the 3 regression models to estimate and plot mean stay and discharge functional status (FIM ratings), as well as probabilities of home discharge for subjects with pneumonia and each of the 4 tier comorbidity categories for all subjects with lower extremity fractures. Statistics software (SPSS 20, SPSS, Chicago, Illinois) was used for all statistical tests, with P < .01 indicating statistical significance.
Results
Pneumonia was listed as a comorbidity for 4,265 or 2.8% of the 153,241 subjects with lower extremity fracture. Approximately 12% (507) of subjects with pneumonia had other comorbidities that placed them into the higher-paying tier 1 or 2 levels. Table 1 shows that all sociodemographic characteristics, clinical factors, and unadjusted outcomes demonstrated statistically significant (P < .01) differences between the pneumonia yes/no groups, with one exception. There was not a statistically significant difference between lower extremity fracture patients with pneumonia and without pneumonia for marital status. In general, subjects with pneumonia tend to be older, to be delayed in getting to rehabilitation, to have more total comorbidities, to be more functionally impaired at admission and discharge, and to experience longer stay. They are also more likely to be male, more likely to be white, and less likely to be discharged home.
Characteristics and Outcomes of Subjects Receiving In-Patient Rehabilitation for Lower Extremity Fracture, by Pneumonia Comorbidity
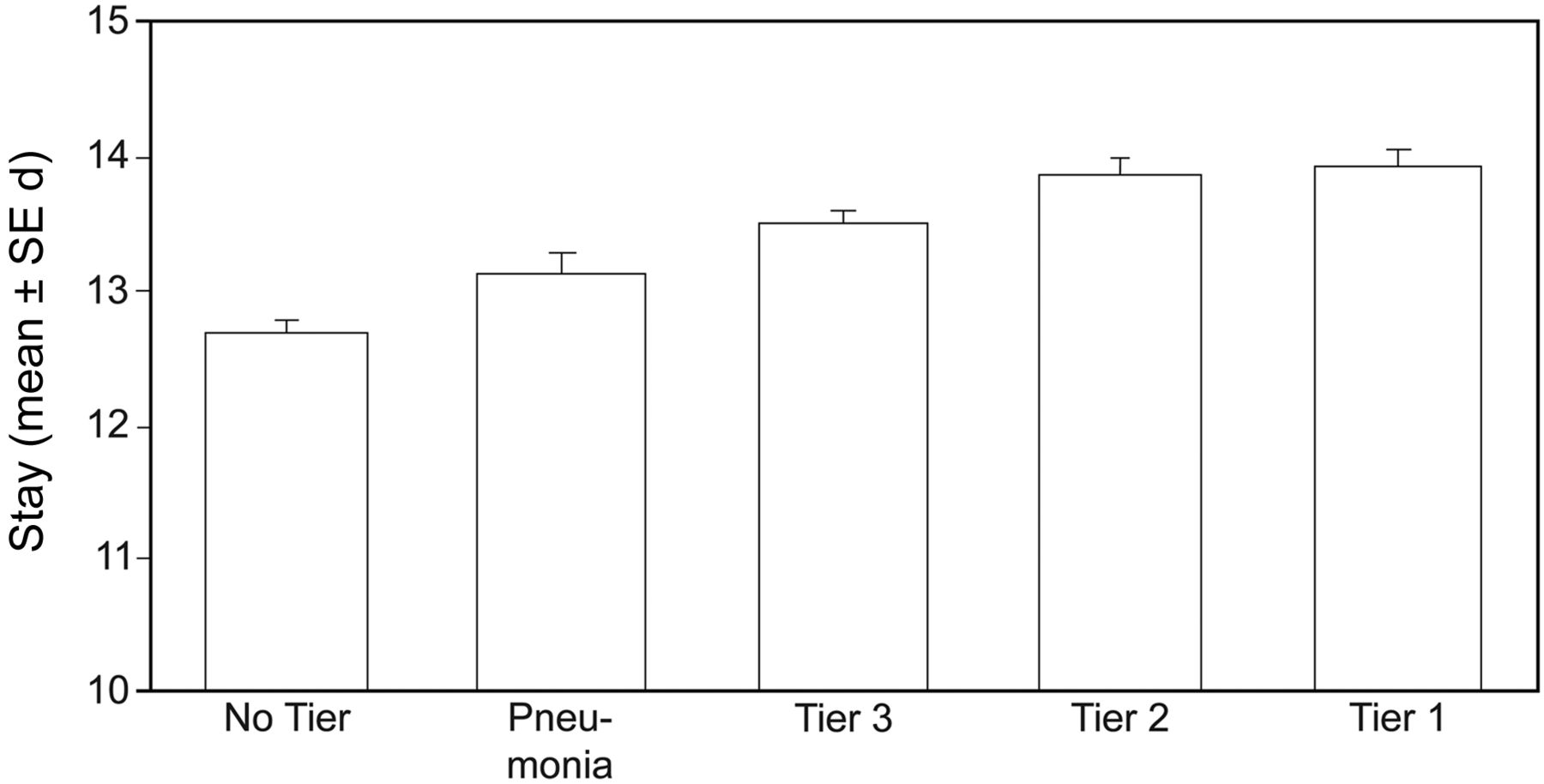
As expected, mortality during rehabilitation was quite low. The rates ranged from 0.1% in the no tier group to 0.4% in the tier 2 and pneumonia groups. The regression coefficients and odds ratios for the 4 tier levels relative to pneumonia from the multivariable (adjusted) models are displayed in Table 2. Estimated group means for stay and discharge functional status (FIM ratings), and group probabilities for home discharge are presented in Figures 1, 2, and 3, respectively. The pneumonia group experienced significantly longer stay (13.1 d vs 12.7 d), lower discharge (FIM ratings) (85.4 vs 87.2), and lower probability of home discharge (61.8% vs 65.8%), compared to the non-tier group, after adjusting for age, sex, race, comorbidity sum, duration since fracture, and other relevant variables (see Table 2). There were no significant differences between the pneumonia group and the aggregate of the other tier 3 comorbidities in terms of discharge (FIM ratings) and odds of home discharge. The predicted stay in the pneumonia group was significantly shorter (approximately 0.4 d) than in the combined (non-pneumonia) tier 3 category after adjusting for age, sex, race comorbidity sum, duration since fracture, and admission functional status.
Linear and Logistic Regression Models of Tier Comorbidity Classification
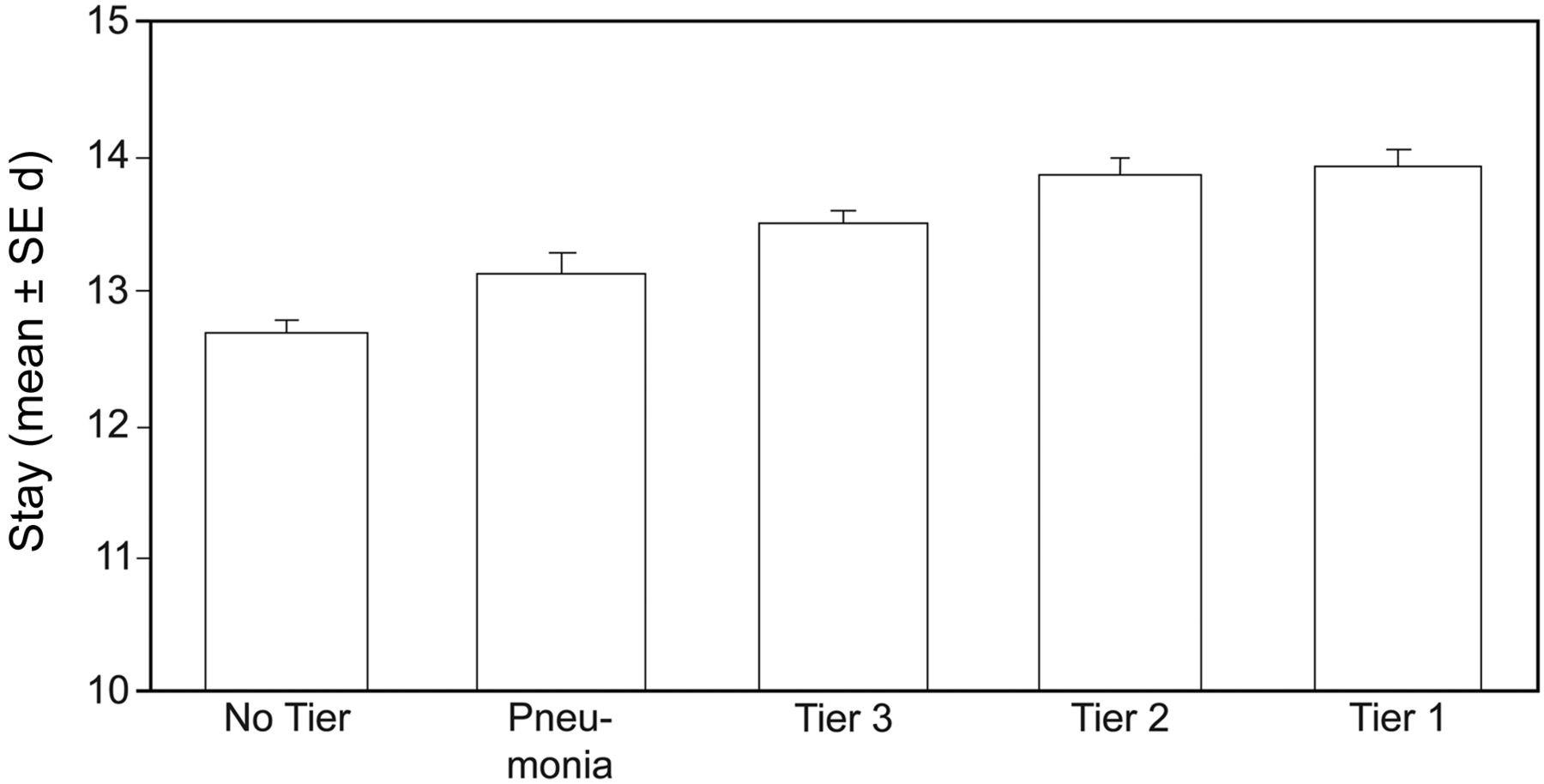
Predicted stay across the 5 comorbidity groups. Estimates and standard errors were obtained from the linear regression model, which controlled for age, sex, race, comorbidity sum, duration since fracture, and admission Functional Independence Measure. The reported values were derived by grand-mean centering continuous variables and selecting female and white for the 2 categorical variables.
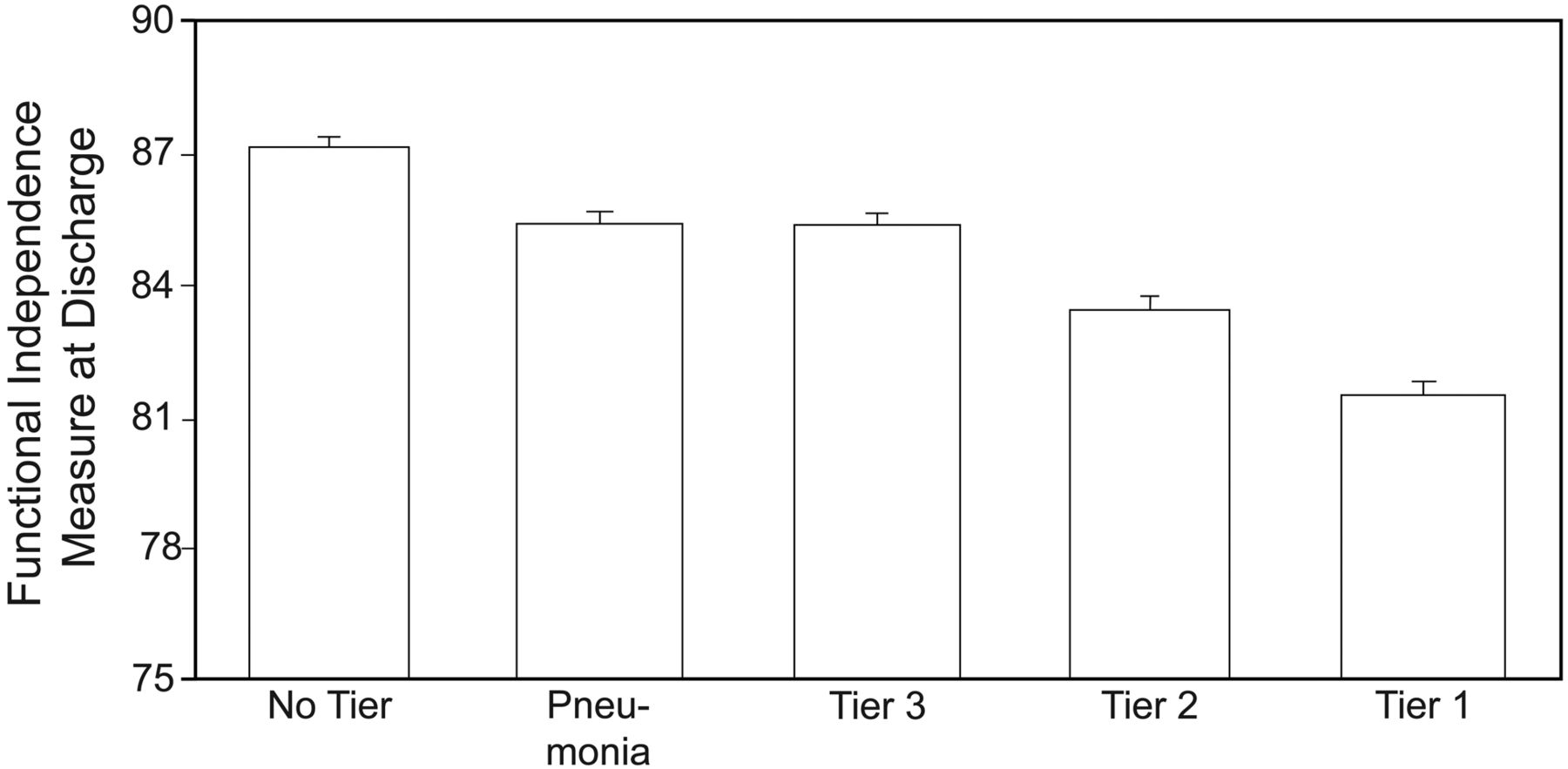
Predicted discharge Functional Independence Measure (FIM) ratings across the 5 comorbidity groups. Estimates and standard errors were obtained from the linear regression model, which controlled for age, sex, race, comorbidity sum, duration since fracture, admission FIM, and stay. The reported values were derived by grand-mean centering continuous variables and selecting female and white for the 2 categorical variables.
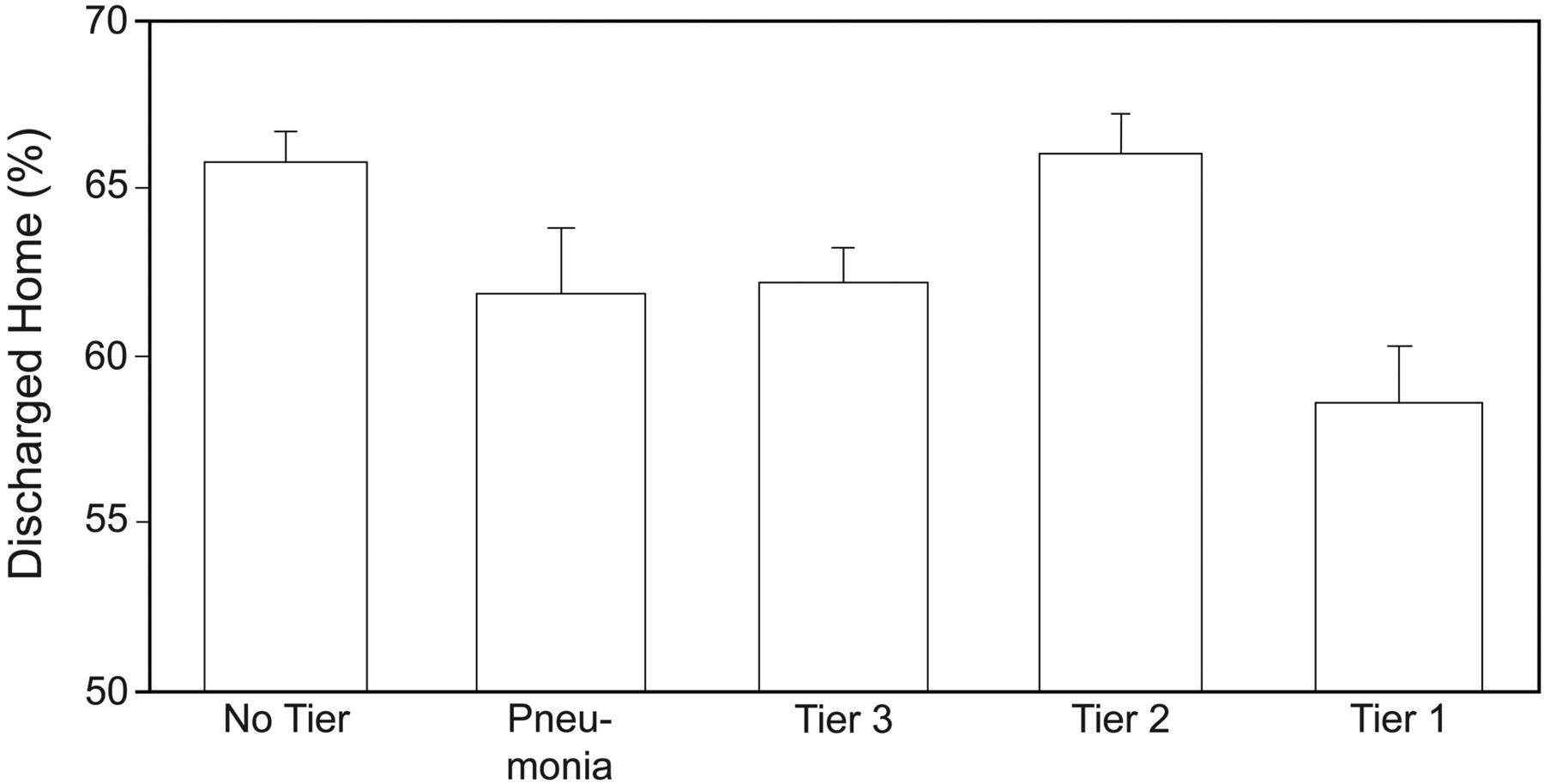
Predicted probabilities for home discharge across the 5 comorbidity groups. Estimates and standard errors were obtained from the logistic regression model, which controlled for age, sex, race, marital status, comorbidity sum, duration since fracture, discharge FIM, and stay. The reported values were derived by grand-mean centering continuous variables and selecting female, white, and unmarried for the 3 categorical variables.
Discussion
We studied the impact of pneumonia on in-patient rehabilitation outcomes among persons with lower extremity fracture in the context of the comorbidity tier system developed by CMS. After controlling for relevant subject characteristics and clinical factors, subjects in the pneumonia group demonstrated poorer outcomes, including longer stay, lower discharge functional status, and lower percentage of discharge to home, compared to subjects without pneumonia (see Table 2).
We also compared subjects with lower extremity fractures in the pneumonia tier group to subjects with other tier 3 comorbidities (eg, diabetes). The subgroup of subjects with pneumonia experienced equivalent discharge functional status ratings and odds of home discharge. Subjects with comorbid pneumonia, however, averaged slightly shorter stay, compared to other tier 3 subjects, and this difference was statistically significant.
The payment received by an in-patient medical rehabilitation facility for a patient with lower extremity fracture plus a tier 3 comorbidity such as pneumonia is approximately 11% greater than the payment for the same patient with no tier comorbidity (Federal Register volume 71, number 160; Friday, August 18, 2006). While our findings support the need for a comorbidity tier reimbursement system, there are important policy questions that remain to be addressed. For example, is the amount of increased reimbursement for pneumonia (and other tier 3 comorbidities) consistent with the increased resources necessary to achieve improved outcomes. In the past these judgments have been made largely based on outcomes associated with an episode of care. The current prospective payment system for in-patient medical rehabilitation was developed using stay as a proxy for cost.7 The purpose of increasing reimbursement for patients with pneumonia (and other tier level comorbidities) is to provide additional services during their treatment in the belief that these services will improve their functional status and reduce their stay for that episode of care. Our study did not address the issue of the cost-benefit of the tier 3 comorbidity reimbursement. This remains an important topic for future research. It is important for 2 reasons. First, hospital acquired pneumonia is predominantly a problem of older adults.9 Age and the presence of multiple comorbid conditions are primary risk factors for developing hospital acquired pneumonia.10,11 The aging demographics of the United States population mean that more older (> 75 years) adults will be experiencing hip fractures and potentially developing pneumonia in the next 2 decades.
The second factor contributing to the need for additional research is the changing healthcare system. The Affordable Care Act, and other components of healthcare reform, place an increased emphasis on outcomes and cost across the continuum of care, and away from the current focus on individual episodes of care.12 What occurs during the acute care and in-patient rehabilitation experience has implications for downstream outcomes and costs. For example, our study found 61.8% of subjects with pneumonia were discharged home, compared to 65.8% of subjects without pneumonia, after adjusting for relevant covariates (eg, age). The long-term cost for persons discharged to institutions versus discharged home will be substantial. In the current system the tier reimbursement for comorbid conditions is focused on reducing costs for the rehabilitation-related episode of care only (eg, stay), not the downstream costs.
Within the Affordable Care Act12 there is a focus on outcomes and cost across the continuum of healthcare service delivery, including prevention, acute care, and post-acute care. The ideal situation would be to prevent hip fractures, and, if they do occur, to prevent the development of pneumonia and other comorbidities. In a more integrated service delivery model, respiratory therapists would be important members of rehabilitation care teams and have a role in screening patients prior to admission to in-patient rehabilitation facilities. Respiratory therapists would also have an important role in helping to prevent and manage pneumonia in post-acute care environments. Such a service delivery model could help reduce discharges to institutional settings, including hospital readmissions. While there are isolated examples of this integrated team model approach across the service delivery continuum, more research is needed to document their effectiveness and demonstrate their compatibility with healthcare reform.
Our study has both limitations and strengths. The information in the Uniform Data System for Medical Rehabilitation database is obtained through medical records and observations, so it is possible that coding and reporting errors can occur. We used ICD-9 codes from patient records to categorize our primary independent variable (pneumonia), and it has been suggested that reliance on these codes may lead to under-reporting of severity or intensity of complications. We lacked data on many factors preceding admission to rehabilitation, including prior disability status and medical conditions. We also do not have data to examine what happened after the in-patient rehabilitation stay. Our study was limited to the variables and methods of data collection available in the Uniform Data System for Medical Rehabilitation; we did not have access to potentially important variables (eg, educational level) that may have influenced our outcomes.
A strength of this study is the use of a large national sample, which provides useful information regarding the role of pneumonia in recovery from lower extremity fracture in subjects receiving in-patient rehabilitation services. To our knowledge, this is the first study to examine the effect of comorbid pneumonia on rehabilitation outcomes following lower extremity fracture.
Conclusions
The findings of our study indicate that patients receiving in-patient medical rehabilitation following a lower extremity fracture and who have comorbid pneumonia demonstrate longer stay, poorer functional status, and are less likely to be discharged home than patients who do not have pneumonia. Our results suggest that the additional resources included in the tier reimbursement system for patients with comorbid pneumonia are appropriate. Further investigation is required, however, to better align the allocation of tier comorbidity resources with patient centered long-term outcomes and to document reductions in cost.
Footnotes
- Correspondence: Kenneth J Ottenbacher PhD, Division of Rehabilitation Sciences, University of Texas Medical Branch, 301 University Boulevard, Galveston TX 77555-1137, E-mail: kottenba{at}utmb.edu.
Dr Ahmed presented a version of this paper at the Open Forum of the AARC Congress 2013, held November 5–8, 2013, in Tampa, Florida.
Dr Ottenbacher was partly supported by National Institutes of Health grant R01 HD6570201. The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}