

Abstract
OBJECTIVE: To assess whether high-resolution computed tomography (HRCT) variables are as good as other known clinical variables in grading emphysema patients.
METHODS: A detailed clinical history was taken and physical examination performed. We performed serum study, lung function testing, and HRCT scanning to assess emphysema. Mean lung density, the attenuation value separating the least 15% of pixels (PERC15), the percentage of the relative area of the lungs with attenuation values < –950 Hounsfield units (HU) (RA950), and histogram analysis were calculated from computerized data.
RESULTS: The final analysis was based on data from 92 subjects, and they were moderately emphysematous (mean lung density was –877 ± 23 HU, PERC15 was –953 ± 21 HU, and RA950 was 16 ± 5%). There was a significant difference regarding subjective emphysema severity in the St George's Respiratory Questionnaire, smoking history, FEV1, C-reactive protein, age, and body mass index (P < .001). There was a significant correlation between the 3 objective image variables and the 6 objective clinical variables (St George's Respiratory Questionnaire, smoking history, FEV1, C-reactive protein, age, and body mass index) (P < .001).
CONCLUSIONS: This study shows the possible important role of HRCT in the diagnosis and quantification of pulmonary emphysema.
Introduction
The major advantage of high-resolution computed tomography (HRCT) in pulmonary emphysema is that, in addition to providing data concerning overall lung destruction, it also identifies the specific locations in the lung where the alveolar surface has been destroyed.1,2 Accurate diagnosis and quantification of pulmonary emphysema during life are important to understand the natural history of the disease, to assess the extent of the disease, and to evaluate and follow up therapeutic interventions. Many studies have addressed the capability of CT to accurately quantify the extent and severity of pulmonary emphysema.3,4
FEV1 is commonly used as a clinical indicator for evaluating the severity of COPD.5 The BODE index, by combining the body-mass index (BMI), air-flow limitation (FEV1), symptoms (as measured by the modified Medical Research Council [MMRC] scale), and exercise capacity (6-min walk distance [6MWD]), predicts mortality in COPD better than lung function alone.6 The recent 2 indexes are also useful in assessing COPD.7,8 COPD is characterized by systemic inflammation with increasing evidence,9 and C-reactive protein (CRP) is a good parameter to monitor the severity of COPD.10 The use of health-related quality of life measures in COPD has currently achieved widespread acceptance. This study uses these parameters to assess subjects with emphysema. The objective of this study was to assess whether the HRCT variables are as good as other known clinical variables in grading emphysema patients.
QUICK LOOK
Current knowledge
Accurate diagnosis and quantification of pulmonary emphysema is important to understanding the natural history of the disease, to assessing the extent of the disease, and to evaluating response to therapy. Traditional methods of assessing the progression include the 6-min walk test, FEV1, and composite scores, including body mass index. High-resolution computed tomography (HRCT) provides morphological information and might provide structure identification in emphysema.
What this paper contributes to our knowledge
The presence and extent of pulmonary emphysema can be roughly estimated by visual assessment of computed tomography sections, but objective quantification is more accurate and more reproducible. HRCT may assist in the diagnosis and quantification.
Methods
Subjects
We recruited patients who had stable symptoms of COPD at an out-patient department, from July 2004 to December 2006. All the smokers had an FEV1/FVC of < 70%, and chest image revealed emphysematous change. The study was approved by the hospital ethics review board. Subjects were prospectively recruited for the purpose of the study and gave their written informed consent prior to participation.
Clinical Variables
A detailed clinical history was taken, and physical examination performed. Lung function testing consisted of spirometry, carried out according to the American Thoracic Society guidelines.11 The degree of dyspnea was checked with the use of the modified MMRC dyspnea scale,12 and the scores on the MMRC dyspnea scale were classified as 0–1, 2, 3, and 4.6 The ADO index includes age, dyspnea, and air-flow obstruction and does not require 6MWD, which may facilitate its use in primary care settings.7 The DOSE index, another attempt to create a multicomponent assessment index of COPD severity, includes symptoms (MMRC dyspnea scale), air-flow limitation (FEV1), smoking status (current vs former), and, importantly, previous exacerbation frequency per year.8 The serum CRP was measured using nephelometry, in accordance with recommendations from Centers for Disease Control and Prevention and the American Heart Association.13 Health-related quality of life was assessed using the validated Chinese version of the St George's Respiratory Questionnaire (SGRQ).14 The SGRQ is a self-administered, disease-specific questionnaire. Scores range from 100 (worst possible health status) to 0 (best possible health status). Based on clinical assessment, all subjects were enrolled according to the Global Initiative for Chronic Obstructive Lung Disease criteria.15 None of the subjects was atopic and none showed substantial bronchodilator reversibility (> 12% of baseline FEV1 and > 200 mL).
Imaging Variables
HRCT scanning was used for the evaluation of emphysema, and scans (Somatom Sensation 16 scanner, Siemens, Erlangen, Germany) were performed on full inspiration at 6 mm intervals, with a collimation (slice thickness) of 1 mm. The scanner was subject to a weekly quality assessment with a phantom check including uniformity, linearity, and noise. In addition there was a 3 monthly engineering check of spatial and contrast resolution and an annual medical physics check. Scanning voltage was 120 kV, and current was 120 mA. Hard copy images were photographed at a window level of –600 Hounsfield units (HU) and a window width of 1,600 HU, as appropriate for viewing lung parenchyma. The scans were evaluated for the presence of emphysema, both qualitatively by the radiologists independently of the remaining research, and quantitatively by a computerized portable and expandable software (OSIRIX 4.19, University Hospital of Geneva, Geneva, Switzerland) for interactive display and manipulation of medical images from different imaging modalities. After data were processed through a spreadsheet (Excel 2007, Microsoft, Redmond, Washington), 3 major lung density parameters were measured. Both lungs were divided into 6 areas comprising the upper, middle, and lower lung fields; an upper section was obtained 1 cm above the superior margin of the aortic arch, a middle section was taken at 1 cm below the carina, and a lower section was taken approximately 3 cm above the top of the diaphragm.16 The severity of emphysema was scored as 0 points = no emphysematous lesions, 1 point = occupying < 25% of the entire lung field, 2 points = occupying 25% to < 50% of the entire lung field, 3 points = occupying 50% to < 75% of the entire lung field, 4 points = occupying > 75% of the entire lung field.17 Mild emphysema was defined as a total score of < 8 points, moderate emphysema was defined as a total score of 8–16 points, and severe emphysema was defined as a total score of > 16 points. Mean lung density (MLD) is the mean attenuation value of all pixels excluding the mediastinum and trachea. The 15th percentile (PERC15) is defined as the threshold value for which 15% of all pixels have a lower density. The relative area 950 (RA950) of low attenuation has been defined as the percentage of pixels within the lungs with a density lower than a predefined threshold (−950 HU). Histogram analysis was calculated from computerized data.
Statistical Analysis
Analysis of the data was done using a spreadsheet (Excel 2007, Microsoft, Redmond, Washington) and statistics software (SPSS 18, SPSS, Chicago, Illinois). The Kruskal–Wallis test for independent samples was applied while nonparametric data of several groups were compared, and the chi-square test was performed to assess differences in categorical variables. A P value < .05 was considered to be statistically significant. Continuous variables are expressed as mean ± SD unless otherwise specified. Linear regression modeling was applied between the 3 objective image variables and the 6 objective clinical variables (SGRQ, smoking history, FEV1, CRP, age, and BMI).
Results
Figure 1 shows an example of a histogram of the density values of pixels in a case of emphysema. The mean was –913 ± 62 HU, the minimal was –1,024 HU, the maximal was –200 HU, and the volume was 5,322 mL. For the part < –950 HU (emphysema), the mean was –963 ± 12 HU, the minimal was –1,024 HU, the maximal was –950 HU, and the volume was 1,110 mL (21%). The RA950 and PERC15 point are closely related, since they are basically each other's inverse functions. This can be best appreciated when the definitions of RA950 and PERC15 are illustrated using the cumulative histogram of the densities (Fig. 2). The RA950 is the y value at which x = –950 HU, and the 15th percentile point is found by determining the x value for which y = 15% in the cumulative histogram.

Histogram of density of pixels in the whole lung in an emphysematous individual. The proportion of the area under the curve to the left of –950 Hounsfield units is a common measure of emphysema.

Definition of relative area below –950 Hounsfield units (RA950) and 15th percentile point (PERC15) in a cumulative histogram by which PERC15 and RA950 have been defined.
Subject Characteristics
The final analysis was based on data from 92 subjects. The average age was 66 ± 9 years, and 71% (n = 65) were men. Mean height was 162 ± 7 cm, and mean weight was 57 ± 8 kg. They had moderately impaired health-related quality of life (SGRQ score was 52 ± 13) and moderate obstructive ventilatory impairment (FEV1 was 56 ± 14% of predicted). They were mildly underweight (BMI was 21.7 ± 3.5 kg/m2), mildly inflamed (CRP was 3.8 ± 1.0 mg/L), smoked heavily (56 ± 15 pack-years), and their imaging showed moderate emphysema (MLD was –877 ± 23 HU, PERC15 was –953 ± 21 HU, and RA950 was 16 ± 5%). They had moderate COPD severity; few were exacerbated. They were mildly to moderately dyspneic, mildly to moderately risky for poor prognosis, and moderately emphysematous imaged.
Clinical and Imaging Variables
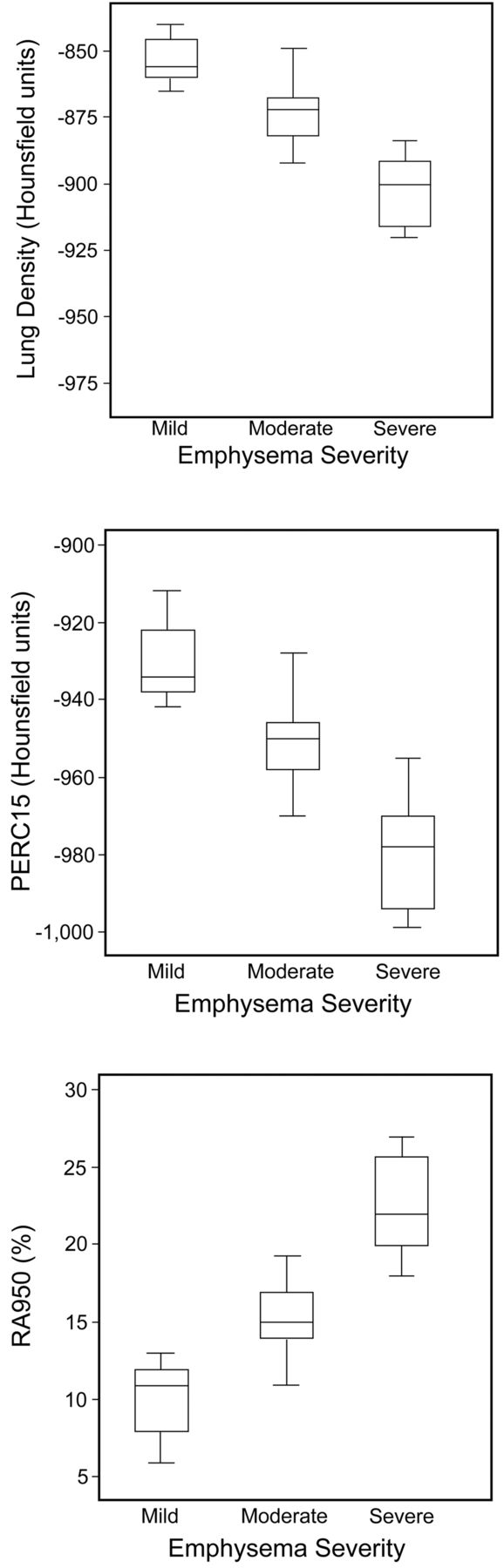
There was a significant difference regarding COPD severity and subjective emphysema severity in SGRQ, smoking history, FEV1, CRP, age, and BMI (P < .001, but P = .003 in smoking history for COPD severity) (Table 1 and Table 2). Subjective imaging variables are as good as other known objective clinical variables in grading emphysema patients. The mean of MLD was –853 ± 8 HU in the mild group, –876 ± 18 HU in the moderate group, and –903 ± 12 HU in the severe group. The mean of PERC15 was –930 ± 9 HU in the mild group, –951 ± 9 HU in the moderate group, and –980 ± 13 HU in the severe group. The mean of RA950 was 10 ± 2% in the mild group, 15 ± 2% in the moderate group, and 23 ± 3% in the severe group. There was also a significant difference regarding COPD severity and subjective emphysema severity in exacerbation, MMRC, ADO index, DOSE index (P < .001, and in sex, nonsignificant for the former, with P = .004 for the latter) (see Table 1 and Table 2). Subjective imaging variables are as good as other known clinical variables in grading emphysema patients. The box plot of 3 objective image variables for subjective emphysema severity is shown in Figure 3. The interquartile range of subjects with various severities was separated, and there was no extreme or outlying value in either group. Subjective imaging variables are as good as objective imaging variables in grading emphysema patients. There were significant correlations between the 3 objective image variables and the 6 objective clinical variables (SGRQ, smoking history, FEV1, CRP, age, and BMI) (P < .001) (Table 3). Objective imaging variables are as good as other known objective clinical variables in grading emphysema patients. RA950 was better correlated with objective clinical variables than PERC15 and MLD. Besides, CRP was better correlated with objective imaging variables than SGRQ, age, BMI, FEV1, and smoking history (Fig. 4).
Subjects by COPD Severity
Subjects by Emphysema Severity
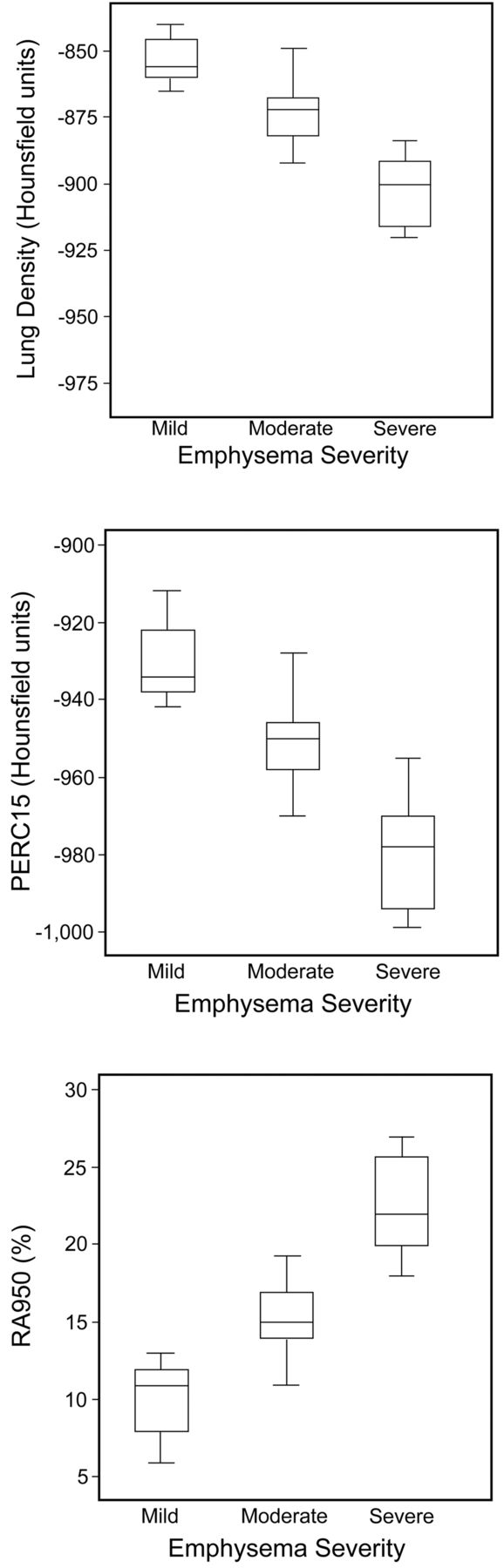
Box plot of mean lung density, the 15th percentile point, and relative area below –950 Hounsfield units for emphysema severity. The lines, boxes, and whiskers represent the median, interquartile range, and minimum or maximum. The central tendency of subjects with various severities are separated.
Correlation Coefficients Between Image Variables and Clinical Variables*
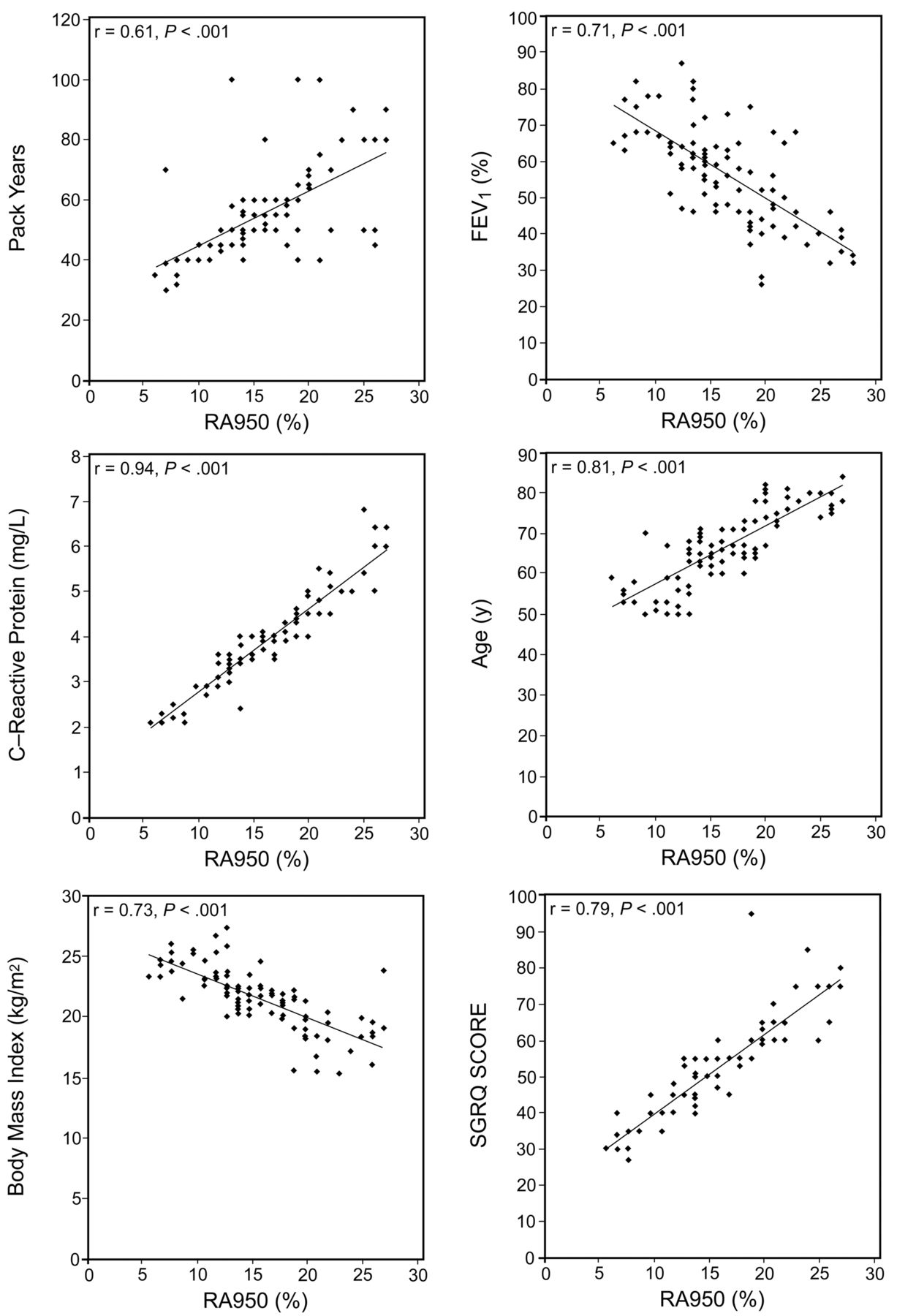
Emphysema severity versus the threshold value for which 15% of all pixels have a lower density (PERC15), and versus the relative area of low attenuation (percentage of pixels lower than the predefined threshold of –950 Hounsfield units [RA950]), and RA950 versus smoking history, FEV1, C-reactive protein, age, body mass index, and St George Respiratory Questionnaire (SGRQ) score. The black lines represents the linear regressions of the data.
Discussion
This was a clinical study to assess whether the HRCT variables are as good as other known clinical variables in grading emphysema patients. The results show that our subjects had moderate emphysema, with MLD of –877 ± 23 HU, PERC15 of –953 ± 21 HU, and RA950 of 16 ± 5%. Moreover, all imaging variables in grading emphysema patients were potentially as useful as other known clinical variables, as shown in Table 1, Table 2, Table 3, Figure 3, and Figure 4.
Modern CT is an imaging method providing transverse anatomical images in which the value of each picture element (ie, pixel) corresponds to the x-ray attenuation of a defined volume of tissue (ie, voxel). Pulmonary emphysema by subjective CT quantification is based on the visual assessment of areas of vascular disruption and decreased attenuation without clear margins, in comparison with contiguous normal parenchyma.18
Given the inherent limitations of subjective visual scoring, the characteristic presentation of emphysema as areas of low CT attenuation values, and the digital nature of the CT data, there is considerable interest in the objective quantification of emphysema on CT scans. Three different approaches have mainly been used for objective quantification of emphysema on CT scanning: use of a threshold value below which emphysema is considered to be present19–21; assessment of the range of lung densities represented in a lung slice21,22; and assessment of overall lung density, often in combination with volumetric imaging.23,24 The objective quantification allows more consistent assessment of disease extent than subjective analysis. It allows assessment of overall and regional changes, to monitor the progression of emphysematous lung destruction in individual patients and to assess the impact of surgical and medical treatment. It should be noted, however, that lung density measurements on CT scanning can be affected by a number of variables, including patient size, depth of inspiration, type of CT scanner used, collimation, and the reconstruction algorithm. The analysis therefore requires careful attention to technique.
The advantage of computer-assisted quantification is the reproducibility of the technique across readers of varying expertise and experience, and across institutions, allowing more accurate comparison of results among different centers.25 Conversely, the advantages of a subjective scoring system are the ease of application and no requirement for expensive dedicated software. A previous study suggests that subjective visual grading should be supplemented with more reliable objective methods whenever a precise and reader-independent quantification of emphysema is required.26
The BODE index is not widely used in clinical practice because 6MWD is time consuming, requires supervision and space, and has not been calibrated to accurately predict the absolute risk of an event in individual patients. An updated BODE index with a simplified point system has been calibrated to predict absolute risks, and a simplified index, the ADO index, has been developed.7 The ADO index includes age, dyspnea, and air-flow obstruction, which may facilitate its use in primary care settings. The DOSE index, another attempt to create a multi-component assessment index of COPD severity, includes symptoms (MMRC dyspnea scale), air-flow limitation (FEV1), smoking status (current vs former), and previous exacerbation frequency.8 Unlike other severity indices, the DOSE index aims at being used in routine clinical practice in all stages of disease severity. Low-grade systemic inflammation, as measured by CRP, has been suggested to link both COPD and cardiovascular diseases through increased atherosclerosis.27
The extent of emphysema, as assessed by CT scan, is a good predictor of mortality in patients with COPD,16 and greater emphysematous destruction is a predictor of a high BODE index.28 A significant inverse relationship between BMI and the extent of emphysema on CT scan in the lungs of male smokers was found, and it is unclear if emphysema predisposes to weight loss among patients who develop COPD or whether low body weight contributes to the development of emphysema.29 The CT measurements revealed that a decreased FEV1 is associated with an increase of emphysema.30 Emphysema severity was increased with increasing age and with increasing number of pack-years.31 The Omori et al study showed that CRP levels were not significantly higher in individuals with mild or moderate emphysema, compared with individuals without emphysema, but CRP levels were modestly correlated with FEV1 among individuals with air-flow obstruction.17 Their subjects were younger, BMI higher, smoking history shorter, CRP better, and FEV1 better. Exacerbation frequency was not related with emphysema severity in the Mair et al study,32 but their subjects' emphysema was less severe, their BMI was higher, and their smoking history shorter. RA950 was better correlated with clinical variables than PERC15 and MLD; that meant that RA950 is a better index for emphysema. Besides, CRP was better correlated with objective imaging variables than age, BMI, FEV1, and smoking history; that meant low-grade systemic inflammation in emphysema patients. (CRP is log-distributed in most studies, and CRP is somehow normally distributed in this study. The histogram, log scale, and median with interquartile range of CRP were reported as supplemental data.)
Our study has some other limitations. First, the study population did not receive uniform treatment; therefore, it was impossible to demonstrate the influence of treatment. Second, it took time to perform automatic lung parenchyma segmentation on a slice-by-slice basis, as well as to calculate the variables related to the severity of the pulmonary emphysema component. Third, attention should be paid to radiation dose, and quantification obtained using low-dose CT should be further investigated. Fourth, we did not consider the influence of comorbidities. Fifth, not all subjects had data on lung volume and diffusing capacity. Finally, the study lacked histopathologic corroboration. For these reasons, our findings may not be applicable to all patients with COPD, and larger scale studies that adjust for these limits are needed to investigate the effects.
Conclusions
In summary, CT scanning is of particular interest for the in vivo diagnosis and quantification of pulmonary emphysema, because this imaging technique offers measurements of morphological information with the possibility of structure identification. The presence and extent of pulmonary emphysema can be roughly estimated by visual assessment of CT sections, but objective quantification is more accurate and more reproducible. This study shows the possible important role of CT in the diagnosis and quantification of pulmonary emphysema.
Acknowledgments
The authors thank Chi-Jen Chen and Hui-Ling Hsu for their advice and help in setting up the technique, Dr Robbin Lin for his help with the statistical analysis and graphical presentation of data, Dr Winston W Shen for his editing assistance, and the Lung Function Staff for their help in recruiting data.
Footnotes
- Correspondence: Jeng-Shing Wang MD MSc, Division of Respirology, Antai Tian-Sheng Memorial Hospital, 166 Min-Shiang Street, Kaohsiung 800, Taiwan. E-mail: wangjs6{at}hotmail.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}