

Abstract
BACKGROUND: Children with neurological impairment often suffer from insufficient airway secretion clearance, which substantially increases their respiratory morbidity. The goal of the study was to assess the clinical feasibility of high-frequency chest wall compression (HFCWC) therapy in neurologically impaired children with respiratory symptoms.
METHODS: This was a single-center, investigator initiated, prospective study. Twenty-two subjects were studied for 12 months before and 12 months after initiation of HFCWC therapy, and 15 subjects were followed for an additional 12 months. The threshold of adherence to HFCWC therapy was 70%. The number of pulmonary exacerbations that required hospitalization was recorded.
RESULTS: Forty-five percent of the subjects required hospital admission before initiation of HFCWC therapy. This rate decreased to 36% after the first year with HFCWC, and to 13% after the second year with HFCWC. There was a statistically significant reduction of the number of hospital days at follow-up, relative to before treatment. Use of an assisted-cough device or the presence of tracheostomy did not significantly affect hospitalization days.
CONCLUSIONS: Regular HFCWC therapy may reduce the number of hospitalizations in neurologically impaired children.
- neurological impairment
- secretion clearance
- respiratory
- high-frequency chest wall compression
- hospitalization
Introduction
Respiratory management of children with neurological impairment is complex.1,2 Upper-airway obstruction syndromes, reflux and aspiration of gastric contents, impaired lower-respiratory secretion clearance due to weak cough, frequent lower-respiratory-tract infections, chest wall deformities and related deformities of the tracheobronchial tree contribute to morbidity and pose a constant challenge to clinicians.3–6 Frequent lower-respiratory-tract infections require multiple courses of antibiotics and hospital and ICU admissions that heavily burden the healthcare system.7–9
Impaired clearance of lower-respiratory secretions leads to acute and chronic lower-respiratory-tract infection, exacerbating a build-up of lower-respiratory secretions.10,11 In an attempt to promote clearance of these lower-respiratory secretions, chest physical therapy is often incorporated in the management of children with neurological impairment.1,4,12 An appreciation of the role of impaired cough clearance in the respiratory morbidity of children with neuromuscular weakness led to widespread use of the cough-assistance device (mechanical insufflator-exsufflator), which was shown to be effective and now is strongly recommended as a standard of care in these children.13–18 However, use of the cough-assistance device in children with cerebral palsy and other neurological syndromes has not yet been studied, is controversial, and the implementation differs between institutions.
Intrapulmonary percussive ventilation therapy was shown to be effective in adolescents and young adults with neuromuscular disease.19 Other chest physical therapy modalities include end-expiratory positive pressure devices, manual chest physical therapy, and high-frequency chest wall compression (HFCWC). The selection of chest physical therapy methods used in this group of patients depends on several factors, including the cognitive status of the patient, severity of respiratory compromise, and in many ways on the clinical experience of the clinicians.
There are limited data on the efficacy of HFCWC therapy in children with neurological impairment, and no data on the impact of HFCWC on healthcare costs in this category of patients. We conducted a prospective study to evaluate the clinical feasibility of HFCWC in children with neurological impairment and respiratory symptoms. We hypothesized that HFCWC would decrease respiratory morbidity in this population of children. We compared the number of hospitalizations and hospital days in a group of children with neurological impairment and respiratory symptoms before and after the introduction of HFCWC therapy.
QUICK LOOK
Current knowledge
Children with neurological impairment frequently suffer from insufficient airway secretion clearance, which increases respiratory morbidity. Various airway clearance techniques in these patients have varying levels of success.
What this paper contributes to our knowledge
The addition of high-frequency chest wall compressions (with The Vest) to an airway clearance regimen in children with neurologic impairment was associated with fewer hospitalizations.
Methods
This was a single-center, investigator initiated, prospective study assessing the efficacy of HFCWC therapy in patients with severe neurological impairment and frequent pulmonary exacerbations. The research was conducted at Maimonides Medical Center, Brooklyn, New York. Our institutional review board approved the study. The parents of all study subjects gave informed consent.
Initial Subject Enrollment
The inclusion criteria were age > 18 months, chest circumference > 48 cm, a diagnosis of neurological impairment, and ≥ 2 lower-respiratory-tract infections that required supplemental oxygen and hospitalization in the 12 months prior to study enrollment. The exclusion criteria were diagnosed allergy with a respiratory trigger, unstable head or spinal injury, unresolved pneumothorax or pneumomediastinum, unresolved hemorrhage, hypotension requiring vasopressors or positioning, bronchopleural fistula, gross hemoptysis, pulmonary embolism, burns, open wounds or skin infections on the thorax, osteomyelitis of the ribs, and osteoporosis with a history of fractures.
Follow-Up Subject Enrollment
Chart review was conducted 12 months after the cessation of the main study. Study subjects who completed the main study and remained adherent to HFCWC therapy were considered for enrollment in the follow-up study. Subjects were re-consented for the follow-up study, and data collection was performed retrospectively.
Study Procedures
A complete physical assessment was performed at study enrollment, every 3 months during the study, and at the final visit. Data (Table 1) were collected during study visits and telephone interviews, which were conducted every 14 days for 1 year after enrollment. Subjects continued their routine care, which may have included use of the cough-assist device (CoughAssist, Respironics, Murrysville, Pennsylvania), suctioning, and anti-reflux, anti-seizure, and other medications as usual.
Data Assessment
HFCWC therapy was initialized upon study enrollment. Once enrolled, a home visit was made for device fitting and training the subject and caregivers on the HFCWC device (The Vest, model 105, Hill-Rom, St Paul, Minnesota). The Vest has a built-in hour-meter to measure adherence. HFCWC therapy was used for 12 months, 20 min twice daily, and increased up to 4 times a day for lower-respiratory-tract infection associated with increased oxygen requirement. Subjects 18–36 months old used a frequency of 10 Hz, and subjects > 36 months old used a frequency of 12 Hz. All the subjects used an inflation pressure of 3 arbitrary units. The threshold for adherence to HFCWC therapy was 70%. Subjects who were non-adherent were not permitted to continue in the study, and their HFCWC devices were picked up and returned to Hill-Rom immediately after non-adherence was identified.
A 6 month wash-in period began at HFCWC initiation. The duration of the wash-in period reflected the suggestion that clinical benefits from HFCWC become more apparent after 6 months of treatment.19 The data from the wash-in period were excluded from analysis. An equivalent 6-month period before treatment was also excluded from data analysis, so that no seasonal difference skewed the data. A total of 12 months of data were analyzed for each subject (6 months before initiation of therapy and 6 months after). For example, for a subject enrolled on 6/1/2009, data from 1/1/2009–6/31/2009 and 1/1/2010–6/31/2010 were analyzed and compared. Equivalent 6-month periods before and after interventions were used, so that no seasonal differences skewed the data. The study timeline is summarized in the Figure.
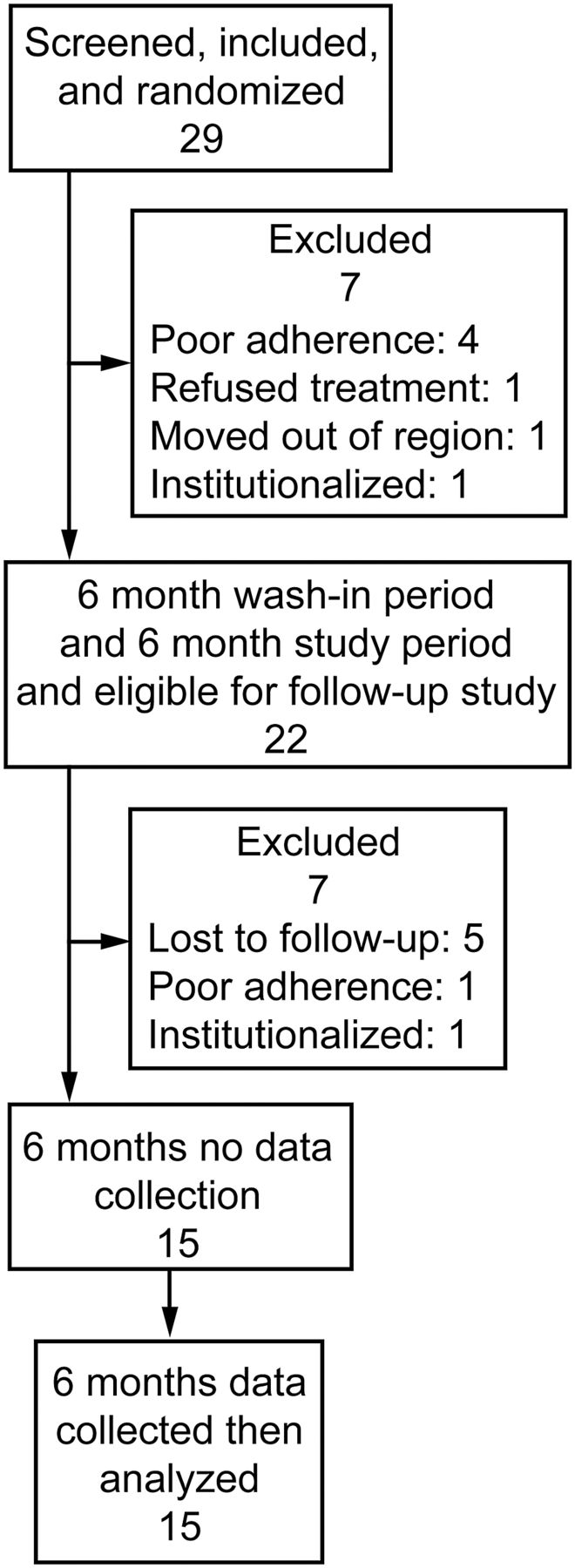
Flow chart of the study timeline.
Follow-up Study Procedures
The study subjects were followed for 12 months after completion of the main study. The data from the last 6 months of HFCWC therapy were compared with those collected during the corresponding 6 months before therapy initiation. An equivalent 6-month period of data from the 1-year follow-up was compared with the previously collected data from the corresponding 6-month period before enrollment.
Statistical Analysis
Normally distributed data are given as mean ± SD, skewed continuous variables as median and IQR, and categorical variables (eg, sex) as number and percent. More than 50% of the subjects had no hospital days (recorded as 0), and so this outcome was dichotomized and summarized in terms of percent hospitalization (yes/no). A one-sample chi-square test was used to test for differences in the proportion of subjects with different sex, race, diagnoses, technology modalities, and comorbid conditions between the main-study subjects and the follow-up subjects. The age difference between the main-study and follow-up subjects was assessed with a one-sample t test.
Primary outcome data were analyzed using general linear modeling, which allows for repeated-measures analysis of subjects with missing data, under the assumption that the data are missing at random, so that all subjects were included for analysis. An underlying gamma distribution for skewed outcomes was assumed, in order to compare the number of hospital days across time (ie, before vs after HFCWC treatment and follow-up). The possible impact of the CoughAssist device and tracheostomy upon outcome measures was analyzed by including appropriate group × time interactions in the general linear modeling analysis. Data were analyzed with statistics software (SAS 9.1, SAS Institute, Cary, North Carolina) for the general linear modeling. All analyses assumed differences were significant at P < .05.
Based on Giarraffa et al20 and Plioplys et al,21 the effect size for reduction in the number of hospital days was initially estimated to be between 1.36 and 1.55 days. Since these estimates appeared to be rather high, the lower one was reduced by half, to 0.68. Based on that effect size, a minimum of 19 subjects was assumed to be needed to detect a paired difference of that magnitude, with an alpha of .05 and power of 80%. Assuming a 25% drop-out rate, the minimum sample size for recruitment was determined to be 25.
Results
Twenty-nine subjects consented to inclusion in the main study. Four subjects were withdrawn due to non-adherence to HFCWC, one subject refused treatment, one subject moved out of state, and one subject was institutionalized. Twenty-two subjects completed the main study. The mean ± SD age of the main study subjects was 9.55 ± 5.57 years. Sixty-four percent of the subjects had cerebral palsy, and 45% had other diagnoses. Forty-five percent were on mechanical ventilation, and 27% had tracheostomy (Table 2).
Demographics and Clinical Characteristics of Subjects Who Received High-Frequency Chest Wall Compressions Therapy
Of the 22 subjects who completed the main study, 15 were included in the follow-up group, 7 of whom were later excluded (5 lost to follow-up, one institutionalized, and one was non-adherent to HFCWC during the follow-up period). The mean baseline age of the follow-up subjects was 9.44 ± 5.49 years. There were no significant differences in demographics, diagnoses, or technology modalities between the main-study subjects and the follow-up study subjects (see Table 2).
There was a statistically significant reduction in the number of hospital days at follow-up, relative to before treatment (P = .03), due to a dramatic decrease in the rate of hospitalization at follow-up (Table 3). Forty-five percent of the subjects required hospital admission before initiation of HFCWC. The rate of hospitalization decreased to 36% after the first year of using HFCWC (P = .47), and to 13% at follow-up (P = .002). The use of CoughAssist or the presence of tracheostomy did not significantly affect hospitalization days (P = .50, and P = .17, respectively).
Rate of Hospital Admissions Before and After Initiation of High-Frequency Chest Wall Compressions Treatment and at Follow-up
Discussion
There are limited data on HFCWC in children with neurological impairment in the peer-reviewed literature. One study found that 12 months of HFCWC significantly decreased the number of pneumonias in subjects with cerebral palsy; however, the sample size was only 7 subjects.21 Yuan et al22 found a trend toward fewer hospitalizations and less intravenous antibiotic use with HFCWC in a randomized controlled trial with 23 subjects with cerebral palsy and neuromuscular disorders.
In our subjects HFCWC reduced the number of hospitalizations and hospital days during the second year of using HFCWC, which suggests that prolonged use of HFCWC benefits children with neurological impairment and respiratory disorders. This finding concurs with Warwick et al,23 who found that long-term (7–26 months) of HFCWC significantly changed toward positivity the negative slope of lung function parameters in children with cystic fibrosis.
Patients with neurological impairment have multiple factors that predispose them to the retention of respiratory secretions and bronchiectasis,24–26 which leads to the characteristic thick and tenacious respiratory secretions. Plioplys et al21 studied HFCWC in children with neurological impairment and cerebral palsy and found that HFCWC dramatically increased effective suctioning, defined as suctioning attempts that retrieved sputum (summation score of effective suctioning 4,825 before treatment, versus 10,445 after treatment, P = .008). It is possible that HFCWC benefits children with cerebral palsy and neurological impairment by promoting the mobilization of tracheobronchial secretions and facilitating mucociliary clearance, as it does in children with cystic fibrosis.27
Impaired cough is a major contributor to respiratory morbidity.2,12 Cough assistance benefits and is now recommended for children with congenital muscle dystrophies.14 In our study the use of the CoughAssist device did not significantly affect hospitalization days, which raises the question of whether improving the rheological characteristics of airway secretions provides clinical benefit even in the absence of effective cough. It is possible that HFCWC loosens lower-respiratory secretions sufficiently to improve mucociliary clearance, but this hypothesis needs to be considered with caution. Acute respiratory deterioration after HFCWC occurred in a child with cerebral palsy, and was attributed to airway secretions mobilization in the presence of ineffective cough.28 Those authors suggested that cough adequacy should be determined before initiating secretion mobilization treatments in such children. Since we did not assess cough adequacy in our subjects, we cannot make a recommendation on assisted cough in children with neurological impairment.
Limitations
Obviously, our study design was suboptimal because of the absence of a control group and lack of randomization. A control group would have been desirable because of the well accepted notion that HFCWC was not shown to be clinically superior to manual chest physical therapy in children with cystic fibrosis.29 However, obtaining a control group that is adherent to manual chest physical therapy may be challenging. Yuan et al22 studied HFCWC in children similar to our subjects. They randomized the children into 2 groups, and 7 of the 12 children in the manual chest physical therapy group were < 30% adherent to manual chest physical therapy, in contrast to excellent adherence in the HFCWC group. Our own clinical experience concurs with that finding. The presence of severe chest wall deformities in many patients with cerebral palsy and neuromuscular impairment makes the delivery of effective manual chest physical therapy nearly impossible. The use of a form-fitting vest to deliver HFCWC overcomes that problem.
Our group of subjects was very heterogeneous; most had cerebral palsy, but other conditions and a wide range of respiratory-compromise severities were involved, and we were unable to factor in all those differences.
We found the use of CoughAssist and the presence of tracheostomy did not affect hospitalization days, but the inclusion of these confounders was post hoc and was not powered for the study outcome measures. Also, we did not monitor our subjects' adherence to the use of the CoughAssist device.
Conclusions
Long-term HFCWC may reduce the number of hospitalizations and hospitalization days in children with neurological impairment. HFCWC should be considered as an important part of the complex approach to respiratory health in children with neurological impairment and chronic respiratory disorders. Future research efforts should be devoted to further defining the indications for HFCWC in different groups of children with neurological impairment, depending on their diagnosis, cognitive function, and degree of respiratory impairment.
Footnotes
- Correspondence: Kathryn Fitzgerald MSN CPNP, Division of Pediatric Pulmonology, New York University Langone Medical Center, 550 First Avenue, New York NY 10016. E-mail: Kathryn.Fitzgerald{at}nyumc.org.
This research was partly supported and monitored by Hill-Rom Advanced Respiratory, which provided funding and vest generators, but did not participate directly in the data collection and analysis. Drs Fitzgerald and Kazachkov have disclosed relationships with Hill-Rom. The authors have disclosed no other conflicts of interest.
Ms Fitzgerald presented a version of this paper at the International Conference of the American Thoracic Society, held May 13–18, 2011, in Denver, Colorado.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}