

Abstract
BACKGROUND: Adrenomedullin (ADM) is a regulatory peptide with many biological actions, but little is known about its role in patients with COPD exacerbation. The purpose of this study was to evaluate the diagnostic and prognostic value of plasma ADM levels on hospital admission in patients with COPD exacerbation.
METHODS: Consecutive subjects admitted to the hospital for COPD exacerbation were included and were followed up for 1 y; in addition, subjects with stable COPD from an out-patient clinic and healthy volunteers were recruited as controls.
RESULTS: Compared with healthy subjects (145 pg/mL [interquartile range {IQR} 103–290 pg/mL]), plasma ADM levels were significantly higher in subjects with COPD exacerbation (270 pg/mL [IQR 170–510 pg/mL], P = .001) and in subjects with stable COPD (400 pg/mL [IQR 210–525 pg/mL], P < .001). In subjects with COPD exacerbation, ADM levels were significantly elevated during exacerbation (560 pg/mL [IQR 495–630 pg/mL]) compared with the recovery phase (470 pg/mL [IQR 393–553 pg/mL], P = .01) and the stable phase (200 pg/mL [IQR 143–308 pg/mL], P < .001). In receiver operating characteristic analysis, in subjects with COPD exacerbation, ADM had high diagnostic accuracy in differentiating between exacerbation and the stable phase (area under the curve 0.97, 95% CI 0.93–1.02, P < .001). In Cox regression analysis, plasma ADM was not independently associated with 1-y survival (P = .97), but it could accurately predicted the need for ICU care (hazard ratio 1.37, 95% CI 1.09–1.72, P = .008).
CONCLUSIONS: Plasma ADM is a valuable biomarker to confirm COPD exacerbation; furthermore, plasma ADM independently predicts the need of ICU care, although it is not associated with long-term mortality in patients with COPD exacerbation.
Introduction
COPD is the fourth leading cause of death worldwide, and it is predicted to be the third leading cause by the year 2020.1 Exacerbations are important events in the chronic and progressive course of COPD.2 Frequent exacerbations could reduce quality of life, speed disease progression, and increase the risk of death.3 Exacerbation management usually requires medical care, and severe exacerbations frequently require hospital admission. Several systemic biomarkers are increased during exacerbations, and some of them have been identified as valuable tools for disease diagnosis4 and outcome prediction5 in the stable stage. However, whether these biomarkers have diagnostic or prognostic value for exacerbations is not clear.
Although COPD exacerbation was defined in 2000,6 it is difficult in clinical practice to reliably distinguish between exacerbation and the stable stage because this definition is based on the patient's symptom changes and requires subjective assessment by the patient and the physician. It is now widely recognized that COPD is associated with systemic inflammation, and several circulating biomarkers are increased at the time of exacerbation. Within this context, there has been great interest in developing a biomarker that is present at different concentrations on exacerbation and in stable disease. One biomarker of interest is adrenomedullin (ADM), a peptide that has a range of biological functions.
ADM is a 52-amino acid peptide that was first isolated from human pheochromocytoma.7 It can be synthesized by many tissues and cells, such as the adrenal medulla, myocardium, central nervous system, and vascular smooth muscle cells.8 ADM has a variety of biological actions, including vasodilatory,9 bactericidal,10 and anti-inflammatory activities.11 Plasma ADM has been shown to be elevated in a number of diseases, such as arterial hypertension,12 myocardial infarction,13 heart failure,14 renal diseases,15 and septic shock.16 Furthermore, it is involved in the pathophysiology of these disorders. An earlier study described increased ADM levels in patients with COPD,17 but its mechanism of action in this disease remains unclear.
The utility of plasma ADM levels in disease diagnosis has been discussed in acute dyspnea18 and sepsis,19 and plasma ADM levels have been shown to be helpful in the early diagnosis of sepsis. In addition, plasma ADM concentrations have also been found to predict prognosis in patients with acute myocardial infarction20 and community-acquired pneumonia.21 However, there is little information about the use of ADM levels in patients with COPD.
Therefore, in this study, we aimed to investigate the diagnostic and prognostic value of plasma ADM levels on hospital admission in patients with COPD exacerbation. First, we tried to evaluate the diagnostic accuracy of ADM in patients with COPD requiring hospitalization for exacerbation. Second, we sought to assess the predictive ability of ADM for long-term outcome in the same patients.
QUICK LOOK
Current knowledge
Adrenomedullin (ADM) is a regulatory peptide with vasodilatory, bactericidal, and anti-inflammatory activity. Little is known about the role of ADM in patients with COPD exacerbation.
What this paper contributes to our knowledge
Plasma ADM is a valuable biomarker to confirm COPD exacerbation. Additionally, plasma ADM levels independently predict the need for ICU admission, although they are not associated with long-term mortality.
Methods
Study Design and Subjects
From May 1, 2011, to May 31, 2012, all subjects with COPD exacerbation admitted to the Respiratory Department of Union Hospital in Wuhan, China, were included in this study. In addition, subjects with stable COPD from the out-patient clinic and healthy volunteers were recruited as controls. The diagnosis of COPD was based on clinical history, physical examination, spirometry, and chest radiographs. COPD exacerbation is defined as a sustained worsening of a patient's condition (from the stable state and beyond normal day-to-day variations) that is acute in onset and necessitates a change in regular medication in a patient with underlying COPD.6 Stable COPD is defined as the time point of inclusion without any reported worsening of a patient's condition beyond normal day-to-day variations and with no change in regular medication in the preceding 30 d. Subjects were excluded if they had significant comorbidities, including tuberculosis, any lung disease other than COPD, coronary artery disease, congestive heart failure, liver or renal impairment or failure, diabetes mellitus, cancer, or collagen and vascular disorders.
Subjects with COPD exacerbation were examined on admission by a specialist in pulmonary medicine. The baseline assessment included the gathering of clinical data and the performance of routine blood tests. Blood for ADM measurement was drawn immediately after admission and before the administration of any drug therapy and then stored at −80°C for subsequent analysis. Anthonisen criteria and exacerbation type were recorded.22 Spirometry was performed during hospitalization when available. The severity of COPD was classified according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) grades.23 After full recovery, during out-patient visits, some subjects were re-evaluated at 14–21 d (recovery phase) and 6 months (stable phase) after the initial hospital admission; their blood samples for ADM measurement were collected at the same time.
All subjects with COPD exacerbation were followed until September 31, 2013. The primary end point of this study was all-cause mortality during 1 y of follow-up. The secondary end point was the need for ICU care during the initial hospitalization. Survival status and death dates were obtained based on review of medical records and personal interviews with subjects or their families. Medical record review was performed by 2 independent pulmonary specialists. Discrepancies were settled by consensus.
The study was carried out according to the principles of the Declaration of Helsinki and was approved by our local ethics committee. Written informed consent was obtained from all participants.
Measurements
Adrenomedullin was detected in the plasma of all subjects with an enzyme immunoassay kit (Phoenix Pharmaceuticals, Burlingame, California). The lower detection limit of the assay is 0.13 ng/mL, and the assay range is 0–100 ng/mL. Arterial blood gases (PaCO2 and PaO2), leukocyte counts, and serum C-reactive protein levels were recorded from the hospital records.
Statistical Analyses
Discrete variables are expressed as counts (percentages), and continuous variables are expressed as means ± SD or median (interquartile range [IQR]). Comparability of groups was analyzed by chi-square test, 2-sample t test, Mann-Whitney U test, Kruskal-Wallis analysis of variance, Wilcoxon signed-rank test, or Friedman test as appropriate. Receiver operating characteristic curve analyses with area under the curve were constructed to evaluate the diagnostic accuracy of ADM for COPD exacerbation. Correlation analyses were performed using the Spearman rank correlation. Cox regression univariate and multivariate analyses were applied to assess the influence of age, gender, body mass index, leukocyte counts, C-reactive protein, percent-of-predicted FEV1, PaO2, PaCO2, and ADM levels at admission on 1-y survival and to identify independent predictors for the need for ICU care. Skewed data were logarithmically transformed for regression analyses. Statistical analyses were performed using SPSS 19.0 (SPSS, Chicago, Illinois). All tests were 2-tailed, and P < .05 was regarded as statistically significant.
Results
Seventy-nine subjects with COPD exacerbation were included, and 29 subjects with stable COPD and 20 healthy volunteers were also enrolled. The detailed baseline characteristics of the 128 subjects are presented in Table 1. For subjects with COPD exacerbation, the main cause of exacerbations was infection (72.2%), diagnosed by the isolation of bacterial pathogens in sputum culture or by the presence of purulent sputum and fever. Other causes of exacerbations were inhalation of cold air or particles (19.0%), non-adherence to inhaled medication (6.3%), and pneumothorax (2.5%). Mean age at inclusion was 67.0 y. Spirometry measurement during hospitalization was available for 58 subjects. The mean ± SD percent-of-predicted FEV1 was 35.05 ± 17.98%, and the mean ± SD FEV1/FVC was 0.45 ± 0.13. According to Anthonisen criteria, exacerbation were graded as type 1 in 22 subjects (27.8%), as type 2 in 24 subjects (30.4%), and as type 3 in 33 subjects (41.8%). The median hospital stay was 9 d (IQR 6–13 d). Four subjects (5.0%) died in the hospital. There were another 9 deaths during the follow-up period. Thus, 13 subjects (16.5%) died within 1 y of the initial hospitalization. In addition, 30 subjects (38.0%) required a re-hospitalization due to exacerbation within 1 y of follow-up. For subjects with stable COPD, the mean age at inclusion was 64.9 y. The mean ± SD percent-of-predicted FEV1 was 34.94 ± 13.18%, and the mean ± SD FEV1/FVC was 0.37 ± 0.09. According to the GOLD criteria, 5 subjects (17.2%) were GOLD 2, 12 subjects (41.4%) were GOLD 3, and 12 subjects (41.4%) were GOLD 4. For healthy volunteers, the mean age at inclusion was 61.6 y, the mean ± SD percent-of-predicted FEV1 was 103.33 ± 8.42%, and the mean ± SD FEV1/FVC was 0.80 ± 0.04.
Baseline Characteristics of Subjects Requiring Hospitalization for COPD Exacerbation, Subjects With Stable COPD From an Out-Patient Clinic, and Healthy Controls
In subjects with COPD exacerbation, although a correlation was found between ADM levels at hospital admission and COPD severity according to the GOLD criteria (r = 0.28, P = .03), the ADM levels did not discriminate between different GOLD grades (P = .13): ADM levels in subjects with GOLD 2 were 175 pg/mL (IQR 115–355 pg/mL), with GOLD 3 were 285 pg/mL (IQR 163–580 pg/mL), and with GOLD 4 were 380 pg/mL (IQR 205–615 pg/mL). Similarly, there were no differences between 3 Anthonisen exacerbation types (P = .55): ADM levels for subjects with type 1 were 255 pg/mL (IQR 165–408 pg/mL), with type 2 were 240 pg/mL (IQR 155–535 pg/mL), and with type 3 were 420 pg/mL (IQR 170–570 pg/mL). As shown in Table 2, a significant correlation was observed between ADM levels on hospital admission and smoking history (r = 0.23, P = .04), but there was no correlation between ADM levels and leukocyte counts (r = 0.11, P = .33), C-reactive protein (r = 0.02, P = .90), PaO2 (r = −0.20, P = .10), PaCO2 (r = 0.11, P = .39), or percent-of-predicted FEV1 (r = −0.18, P = .19).
Spearman Correlation Between Clinical, Laboratory Parameters, and Plasma Adrenomedullin Levels of Subjects With COPD Exacerbation on Hospital Admission
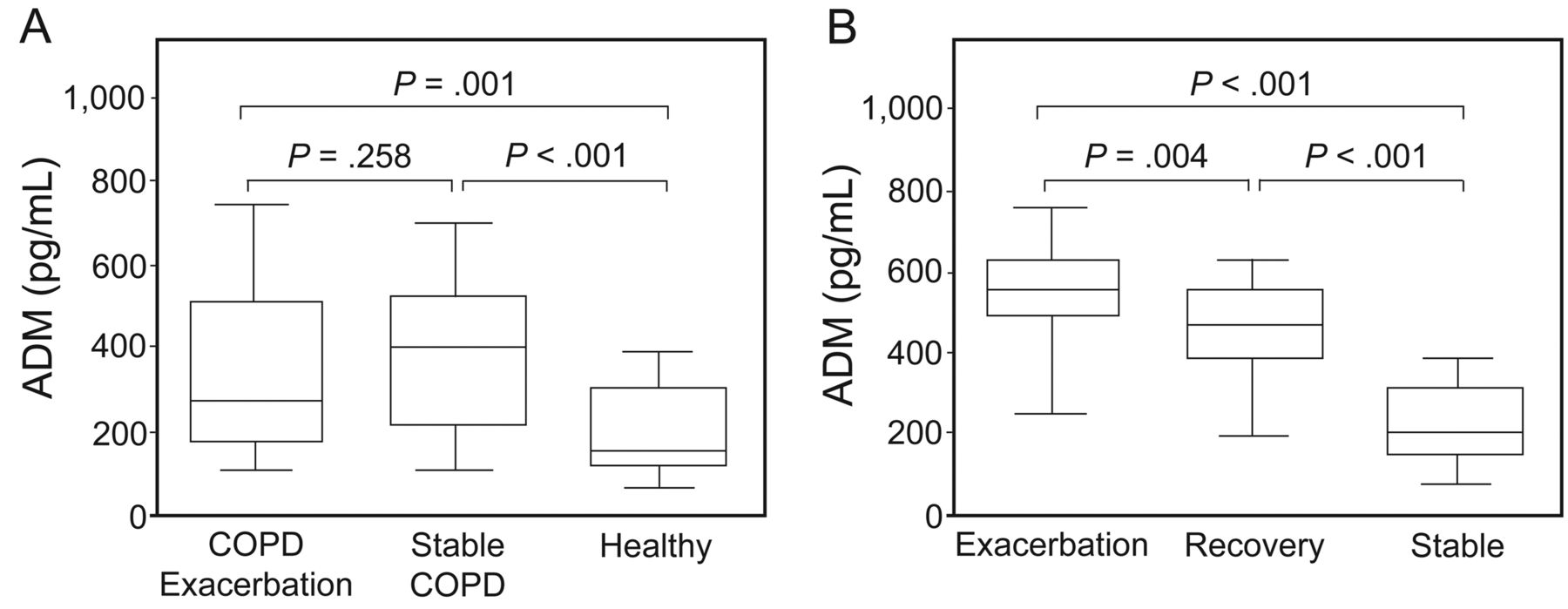
Compared with healthy individuals (145 pg/mL [IQR 103–290 pg/mL]), ADM levels were significantly higher in subjects with COPD exacerbation (270 pg/mL [IQR 170–510 pg/mL], P = .001) and in subjects with stable COPD (400 pg/mL [IQR 210–525 pg/mL], P < .001) (Fig. 1A). Although subjects with stable COPD seemed to have higher ADM concentrations than COPD exacerbation, it was not significant (P = .26). For subjects with COPD exacerbation, blood drawn for ADM analysis in 3 phases was available for 20 subjects. ADM levels were significantly elevated during exacerbation (560 pg/mL [IQR 495–630 pg/mL]) compared with the recovery phase (470 pg/mL [IQR 393–553 pg/mL], P = .01) and the stable phase (200 pg/mL [IQR 143–308 pg/mL], P < .001). Furthermore, ADM levels in the stable phase were significantly lower than in the recovery phase (P < .001) (Fig. 1B).

A: Plasma adrenomedullin (ADM) levels in subjects with COPD exacerbation (n = 79), subjects with stable COPD (n = 29), and healthy volunteers (n = 20). Compared with healthy subjects (145 pg/mL [IQR 103–290 pg/mL]), ADM levels were significantly higher in subjects with COPD exacerbation (270 pg/mL [IQR 170–510 pg/mL], P = .001) and in subjects with stable COPD (400 pg/mL [IQR 210–525 pg/mL], P < .001), but there were no differences between subjects with COPD exacerbation and those with stable COPD (P = .26). B: Plasma ADM levels on hospital admission, in the recovery phase (14–21 d after hospital admission), and in the stable phase (6 months after hospital admission) (n = 20). ADM levels were significantly elevated during exacerbation (560 pg/mL [IQR 495–630 pg/mL]) compared with the recovery phase (470 pg/mL [IQR 393–553 pg/mL], P = .004) and the stable phase (200 pg/mL [IQR 143–308 pg/mL], P < .001). Furthermore, ADM levels in the stable phase were significantly lower than in the recovery phase (P < .001). The center line represents the median, the box represents the 25th to 75th interquartile range, and the bars represent the 5th/95th percentiles.
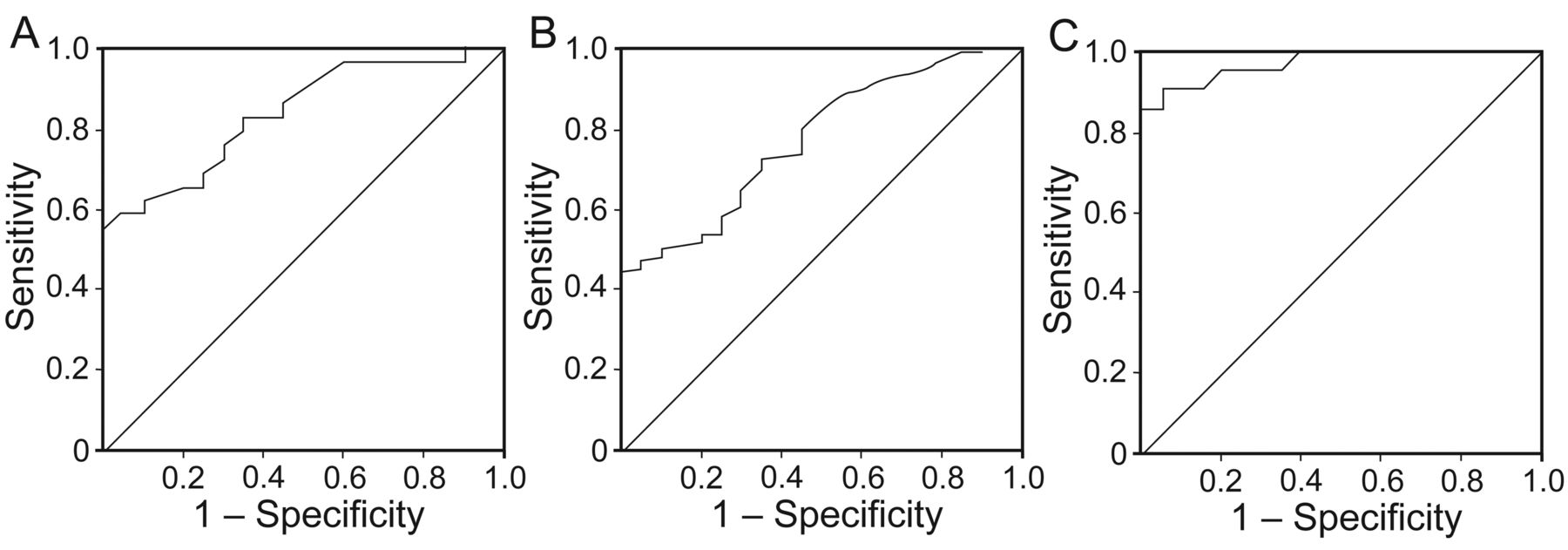
In receiver operating characteristic analysis (Table 3), ADM levels could not be used to differentiate COPD exacerbation from stable COPD (area under the curve 0.43, 95% CI 0.31–0.55, P = .26); however, they could distinguish between stable COPD and healthy control (area under the curve 0.84, 95% CI 0.73–0.95, P < .001) with a cutoff of 225 pg/mL (Fig. 2A). Moreover, for the diagnosis of COPD (COPD vs healthy control), ADM had an area under the curve of 0.78 (95% CI 0.68–0.88, P < .001) with a cutoff of 185 pg/mL (Fig. 2B). Of note, in subjects with COPD exacerbation (n = 20), ADM levels had high diagnostic accuracy in differentiating between exacerbation and the stable phase (area under the curve 0.97, 95% CI 0.93–1.02, P < .001) (Fig. 2C). Using a cutoff of 360 pg/mL for ADM led to a sensitivity of 90.0%, a specificity of 95.0%, a positive likelihood ratio of 18, and a negative likelihood ratio of 0.11.
Diagnostic Accuracy of Plasma Adrenomedullin in Receiver Operating Characteristic Curve Analysis

Diagnostic performance of plasma adrenomedullin (ADM) in receiver operating characteristic curve analysis. A: Plasma ADM was able to differentiate between stable COPD (n = 29) and healthy control (n = 20) (area under the curve 0.84, 95% CI 0.73–0.95, P < .001). B: Plasma ADM could also distinguish between COPD (COPD exacerbation and stable COPD; n = 108) and healthy control (n = 20) (area under the curve 0.78 95% CI 0.68–0.87, P < .001). C: For subjects with COPD exacerbation (n = 20), plasma ADM had high diagnostic accuracy in differentiating between exacerbation and the stable phase (area under the curve 0.97, 95% CI 0.93–1.02, P < .001).
Overall, 12 subjects with COPD exacerbation died during the 6-month follow-up period, and one patient died within the following 6 months. ADM levels on presentation did not differ significantly between subjects dying within 1 y after the index hospitalization and long-term survivors (380 pg/mL [IQR 180–480 pg/mL] vs 260 pg/mL [IQR 165–550 pg/mL], P = .86). In univariate Cox regression analysis, age (P = .19), gender (P = .31), body mass index (P = .34), PaO2 (P = .21), leukocyte counts (P = .19), percent-of-predicted FEV1 (P = .32), and ADM levels (P = .97) on hospital admission were not associated with 1-y survival, but associations were found for a number of admissions in the previous year (hazard ratio 1.13, 95% CI 1.01–1.25, P = .03) and PaCO2 (hazard ratio 1.06, 95% CI 1.02–1.09, P = .001), whereas in multivariate Cox regression analysis, the number of admissions in the previous year (hazard ratio 1.16, 95% CI 1.02–1.32, P = .030) and PaCO2 (hazard ratio 1.06, 95% CI 1.03–1.10, P = .001) were still the independent predictive factors associated with 1-y survival.
A total of 16 subjects (20.3%) required ICU treatment and mechanical ventilation or vasopressor therapy. Except for a higher PaCO2 on hospital admission (mean ± SD 66.7 ± 17.7 vs 53.9 ± 14.9 mm Hg, P = .01), there were no differences in age, out-patient medication, oxygen saturation, and duration of exacerbation episode between these subjects and the overall cohort, whereas ADM levels were significantly higher in subjects transferred to the ICU compared with those treated in the medical ward (510 pg/mL [IQR 253–628 pg/mL] vs 230 pg/mL [IQR 150–465 pg/mL], P = .007) (Fig. 3) and correlated well with ICU stay (r = 0.32, P = .004) and in-hospital stay (r = 0.41, P < .001). Hence, a Cox regression analysis was performed to identify predictors of the need for ICU treatment (Table 4). Interestingly, in univariate analysis, only ADM levels accurately predicted the need for ICU care (hazard ratio 1.37, 95% CI 1.09–1.72, P = .008).

Plasma adrenomedullin (ADM) levels in subjects requiring ICU treatment (n = 16) compared with subjects not requiring ICU treatment (n = 63) (510 pg/mL [IQR 253–628 pg/mL] vs 230 pg/mL [IQR 150–465 pg/mL], P = .007). The center line represents the median, the box represents the 25th to 75th interquartile range, and the bars represent the 5th/95th percentiles.
Prediction of Need for ICU Treatment in Subjects With COPD Exacerbation by Cox Regression Analysis
Discussion
In this study, we investigated the diagnostic and prognostic value of plasma ADM levels in subjects with COPD exacerbation. Three major findings were reported. First, we found that ADM levels were different among subjects with COPD exacerbation, subjects with stable COPD, and healthy individuals. Second, plasma ADM levels were helpful in differentiating between exacerbation and the stable phase, suggesting that it is an effective biomarker to confirm COPD exacerbation. Finally, ADM levels were significantly higher in subjects requiring ICU treatment and accurately predicted the need for ICU care.
Although a previous study reported that in subjects with COPD exacerbation, ADM levels were markedly increased at exacerbation and decreased significantly in the stable phase,24 the diagnostic accuracy of plasma ADM for this disease had not yet been discussed.
This study is the first to explore the diagnostic performance of plasma ADM levels in subjects with COPD exacerbation. In our work, the utility of plasma ADM in the diagnosis of COPD exacerbation was examined not only horizontally but also longitudinally. Interestingly, plasma ADM levels could not be used to differentiate between subjects with COPD exacerbation and those with stable COPD, but they could be used to differentiate between subjects with stable COPD and healthy individuals. More importantly, plasma ADM levels had high diagnostic accuracy in differentiating between exacerbation and the stable phase in subjects admitted to the hospital for COPD exacerbation. In 2006, Hurst et al25 assessed 36 biomarkers in paired stable and exacerbation plasma samples from 90 subjects with COPD. They found that C-reactive protein was the most selective biomarker in confirming exacerbation; however, its diagnostic accuracy was limited (area under the curve 0.73, 95% CI 0.66–0.8). Compared with C-reactive protein, ADM in our study was sufficiently sensitive and specific for confirming COPD exacerbation (area under the curve 0.97, 95% CI 0.93–1.02).
In contrast to our expectations, plasma ADM levels did not predict death in subjects admitted to the hospital for COPD exacerbation. This result was not in line with a previous investigation24 that established ADM as a strong predictor of death. The possible explanation for this difference is to assume that the baseline characteristics differed between the 2 cohorts of subjects with COPD exacerbation. About 70% of subjects included in the previous study had one or more comorbidities, such as diabetes mellitus, renal failure, and malignancy. Of the subjects who died during the follow-up period, 27% had concomitant malignancy, and 13.5% of deaths were attributed to a cause other than COPD, whereas in our study, subjects were excluded if they had significant comorbidities, and the main causes of mortality were respiratory conditions (ie, COPD-related respiratory failure or pulmonary hypertension). It is known that ADM can behave both as a hormone and a cytokine.26 The inclusion of concomitant comorbidities might complicate the effect of ADM on COPD and confuse its actions on survival. Consequently, we hypothesized that the missing predictive potential of ADM in our work was probably caused by a low prevalence of comorbidities in subjects with COPD exacerbation.
Nevertheless, multivariate Cox regression analysis suggested that the number of admissions in the previous year and PaCO2 on admission are able to adequately predict death in our cohort. This result is consistent with previous studies. Almagro et al27 found that subjects hospitalized on more than one occasion for COPD exacerbation in the previous year had a higher mortality rate compared with other subjects, and mortality increased with the number of hospital admissions. PaCO2 was a well accepted risk factor for mortality in subjects admitted to the hospital for COPD exacerbation.28 The high level of PaCO2, suggestive of chronic alveolar hypoventilation, reflects the severity of the underlying respiratory condition.29 Subjects with chronic hypercapnia often need mechanical ventilation and have a worse prognosis than subjects with normal ventilation.
It is noteworthy that plasma ADM levels on hospital admission correlated significantly with ICU stay and could predict the need for ICU treatment in subjects with COPD exacerbation. This seems to contradict the result obtained for the prediction of death. We assumed that respiratory failure underlying pulmonary disease might contribute to the utility of ADM. Due to hypoxemia or hypercapnia, these subjects were more likely to be treated in the ICU. Previous studies have indicated that hypoxia can up-regulate ADM expression,30 so elevated ADM levels may imply the presence of respiratory failure in subjects with COPD and their need for mechanical ventilation.
Several limitations in this investigation should be mentioned. First, this was a single-center observational study; therefore, our results need to be confirmed by conducting a larger and longer study. Second, pulmonary arterial hypertension, a factor known to be related to COPD, was not included in our analysis because the previous study did not find an association between pulmonary arterial hypertension and ADM and did not demonstrate pulmonary arterial hypertension to be associated with increased mortality.24 Finally, because we conducted an observational study, we can only hypothesize that measurement of ADM levels on admission will help to identify subjects requiring ICU treatment.
Conclusions
In summary, plasma ADM is an effective biomarker to confirm COPD exacerbation. Additionally, plasma ADM levels independently predict the need for ICU treatment, although they are not associated with long-term mortality in patients with COPD exacerbation. Therefore, use of ADM in risk stratification could contribute to an improved outcome in patients with COPD exacerbation.
Footnotes
- Correspondence: Wei-Bing Yang MD, Department of Respiratory and Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1277 Jiefang Avenue, Wuhan 430022, China. E-mail: wbingyang{at}aliyun.com.
Drs Meng and Li are co-first authors.
This work was supported by special funds for chronic respiratory disease research in clinical medicine from the Chinese Medical Association. The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}