

Abstract
BACKGROUND: Previous investigation showed that the volume-time curve technique could be an alternative for endotracheal tube (ETT) cuff management. However, the clinical impact of the volume-time curve application has not been documented. The purpose of this study was to compare the occurrence and intensity of a sore throat, cough, thoracic pain, and pulmonary function between these 2 techniques for ETT cuff management: volume-time curve technique versus minimal occlusive volume (MOV) technique after coronary artery bypass grafting.
METHODS: A total of 450 subjects were randomized into 2 groups for cuff management after intubation: MOV group (n = 222) and volume-time curve group (n = 228). We measured cuff pressure before extubation. We performed spirometry 24 h before and after surgery. We graded sore throat and cough according to a 4-point scale at 1, 24, 72, and 120 h after extubation and assessed thoracic pain at 24 h after extubation and quantified the level of pain by a 10-point scale.
RESULTS: The volume-time curve group presented significantly lower cuff pressure (30.9 ± 2.8 vs 37.7 ± 3.4 cm H2O), less incidence and intensity of sore throat (1 h, 23.7 vs 51.4%; and 24 h, 18.9 vs 40.5%, P < .001), cough (1 h, 19.3 vs 48.6%; and 24 h, 18.4 vs 42.3%, P < .001), thoracic pain (5.2 ± 1.8 vs 7.1 ± 1.7), better preservation of FVC (49.5 ± 9.9 vs 41.8 ± 12.9%, P = .005), and FEV1 (46.6 ± 1.8 vs 38.6 ± 1.4%, P = .005) compared with the MOV group.
CONCLUSIONS: The subjects who received the volume-time curve technique for ETT cuff management presented a significantly lower incidence and severity of sore throat and cough, less thoracic pain, and minimally impaired pulmonary function than those subjects who received the MOV technique during the first 24 h after coronary artery bypass grafting.
Introduction
Sore throat and cough are common problems that occur after endotracheal intubation. In most cases, these symptoms are attributed to increased cuff pressure secondary to endotracheal tube (ETT) cuff overinflation.1 For this reason, various techniques (ie, automated cuff inflation) have been proposed in an attempt to minimize the aforementioned symptoms. Despite the development of newer techniques, conventional techniques (ie, minimal occlusive volume (MOV), seal pressure, minimal leak, finger palpation, and manual cuff inflation with target pressures around 25 cm H2O) are still used in many countries.2
Independent of the technique used, a consensus in the literature confirms that the cuff must be inflated until the air leak stops. The MOV technique has been suggested in the literature as the most appropriate technique for promoting adequate cuff inflation, although several studies have indicated that this technique could be inaccurate because it is difficult to determine precisely when to stop inflating the cuff, which can result in cuff overinflation or hyperinflation.2–5
In a previous study,3 we showed that the volume-time curve technique for ETT cuff management can promote lower cuff pressure and a lower volume of air injected into the cuff compared with the MOV technique because of its capability to identify in real time the exact air volume that is required to fill the cuff to prevent air leakage. However, the clinical impact of the volume-time curve technique has not been documented.
We hypothesized that using the volume-time curve technique, which resulted in smaller cuff pressure after airway sealing,3 could reduce the occurrence of endotracheal intubation-related respiratory symptoms, including sore throat, cough, and thoracic pain, secondary to a cough in patients submitted to coronary artery bypass grafting and a short period of mechanical ventilation, thus influencing the capacities and pulmonary volumes in the early postoperative phase.
The purpose of this study was to compare the occurrence and intensity of sore throat, cough, thoracic pain, and pulmonary function between 2 techniques for ETT cuff management, namely, volume-time curve technique versus MOV technique, after coronary artery bypass grafting.
QUICK LOOK
Current knowledge
Maintenance of endotracheal tube cuff pressure within a safe range prevents silent aspiration of pharyngeal secretions and reduces injury to the tracheal mucosa. A number of techniques, including the minimal seal and minimal leak, have been proposed as the best practices. More recently, closed-loop control of cuff pressure and the use of the volume-time curve have been proposed as alternatives.
What this paper contributes to our knowledge
In the first 24 h following coronary artery bypass grafting, patients receiving the volume-time curve technique had a lower incidence of sore throat, cough, and thoracic pain compared with the minimal occlusive volume technique.
Methods
The institutional ethics committee of the Federal University of São Paulo (São Paulo, Brazil) approved this double-blind randomized controlled study. All of the subjects were informed about the study before their enrollment. Each subject provided a signed consent form. We included subjects who were hospitalized at the Pirajussara and São Paulo Hospitals of the Federal University of São Paulo and who underwent elective off-pump or on-pump coronary artery bypass grafting. The criteria for inclusion in this study were as follows: age ≥ 18 y, oral endotracheal intubation, and conventional mechanical ventilation. We excluded subjects who were obese or had COPD, laryngeal disease or anomaly, difficult intubation (2 or more trials), and previous sore throat (evaluated 1 d before surgery). We also excluded subjects who required prolonged time of mechanical ventilation (> 24 h), placement of a nasogastric tube, and additional analgesia. We included in this study 450 subjects who were randomized into 2 groups: MOV group (n = 222) and volume-time curve group (n = 228).
Anesthesia and Operative Technique
We induced anesthesia in a routine fashion using etomidate and midazolam and maintained with sufentanil and isoflurane (0.5–1%). Experienced anesthesiologists intubated the subjects with standard ETTs of high-residual volume and low-pressure cuff, with an inner diameter of 7.5 mm for females and 8.0 mm for males. Pancuronium was used to intubate and to avoid possible trauma. No lubricant or local anesthetic gel was applied on the ETTs, and peroxide was not used in any patient. After intubation, anesthesiologists inflated the ETT cuffs according to their clinical experience and assessment, and the subjects were allocated into either of the 2 groups according to computer software randomization (using opaque, sealed, and numbered envelopes insured that the randomization data would be kept secret). The 2 groups were as follows.
MOV Group (n = 222).
The cuff was completely deflated by a 20-mL syringe that was attached to the pilot balloon; the cuff was gradually inflated by air injection until the leak disappeared. During inflation, the examiner kept his ear 10 cm from the subject's mouth to ensure that there was no air leak.3
Volume-Time Curve Group (n = 228).
The cuff was fully deflated and gradually inflated with a 20-mL syringe while the examiner analyzed the volume-time curve to generate a proper adjustment of air volume that should be injected into the cuff. We performed a volume-time curve analysis using a specific device for respiratory mechanics evaluation (Ventcare 9505 VSF, Takaoka, São Paulo, Brazil) and a pressure transducer interposed between the mechanical ventilator circuit and the ETT. The volume-time curve can demonstrate the presence of air leaks. An air leak causes a decrease in the exhaled tidal volume compared with the inspiratory volume. In the presence of air leakage, the descending branch of the volume-time curve does not reach the zero value with flattening, being abruptly interrupted by the beginning of the next inspiration (Fig. 1).6 To determine air leakage, we used the time at which flattening of the expiratory branch of the curve occurred. We performed the inflation until the descending branch of the volume-time curve returned to zero, interrupting the flattening that presented earlier.3

Graphic monitoring during cuff adjustment by volume-time curve. The 1st cycle represents a normal curve without air leak. The inspired and expired volumes are equal, and the descendant branch of the curve reaches the baseline. The 2nd cycle represents a curve with a higher air leak. The descendant branch does not reach the baseline, and the expired volume is shorter than the inspired volume; note at the flow-time curve, the lesser expiratory flow. The 3rd cycle represents a curve with lesser air leak (during cuff inflation). The 4th cycle represents a normal curve after cuff adjustment.
During the operation, we ventilated the subjects to maintain normocapnia with FIO2 between 50 and 60% without PEEP. We conducted the on-pump or off-pump coronary artery bypass grafting through a midline sternotomy and the left internal thoracic artery, complemented with additional saphenous vein grafts. In all cases in which the pleural cavity was opened, we inserted an intercostal pleural drain. In all of the subjects, we left a mediastinal tubular drain in the subxiphoid region.
Pulmonary Function Assessment
We evaluated the FVC and FEV1 at the subject's bedside using a portable spirometer (Spirobank G, Medical International Research, Rome, Italy) and according to the standards of the American Thoracic Society.7 We repeated each test 3 times and selected the best result. The same respiratory physiotherapist who was blinded to group allotment performed the pulmonary function testing preoperatively and 24 h after extubation.
Postoperative Management
After the operation, the subjects were transferred to the ICU and ventilated using pressure controlled continuous mandatory ventilation at 14 breaths/min, inspiratory time of 1.2 s, PEEP 5 cm H2O, inspiratory pressure to promote a tidal volume of 8 mL/kg of the predicted body weight, and FIO2 adjusted to maintain an arterial oxygen saturation of > 90%.
We performed extubation when the subject was hemodynamically stable and alert enough to maintain self-ventilation and adequate blood gas values. All of the subjects received the same analgesic protocol (100 mg of tramadol chlorhydrate), which was administered 4 times/d until discharge.
Measurements and Recordings
A professional who was blinded to the group allotment measured cuff pressure, independent of randomization, at the end of expiration immediately before extubation (to avoid possible bias secondary to the manometer attachment)8 using a manometer graduated in cm H2O (VBM Medizintechnik GmbH, Sulz am Neckar, Germany) and connected to the inflating channel of the pilot balloon.
At 1, 24, 72, and 120 h after extubation, the subjects related their symptoms and intensity of their sore throat according to a 4-point scale (0–3): 0 = no sore throat, 1 = mild sore throat (less severe than with a cold), 2 = moderate sore throat (similar to that noted with a cold), and 3 = severe sore throat (more severe than with a cold).9
The grades of coughing episodes (0 = no coughing, 1 = one cough, 2 = more than one episode of nonsustained coughing, 3 = sustained and repetitive coughing with head lift)10 were also evaluated at 4 time points: 1, 24, 72, and 120 h after extubation.
Thoracic pain sensation was always assessed 24 h after extubation before spirometry and quantified by a modified standard score (ranging from 0 = no pain to 10 = unbearable pain).11 The subjects were blinded to the randomization, and the examiner who assessed sore throat, cough, and thoracic pain scores was also blinded to the group allocation.
Statistical Analysis
Calculation of sample size was based on the assumptions for detecting a 20% difference between the subjects for the primary end point: sore throat with a significance level of 5% and a power of 95%. These assumptions suggested a sample size of 222 subjects, which resulted in a sample size of 500 subjects for covering attrition. Data were expressed as the mean ± SD. The FVC and FEV1 values were expressed as a percentage of the preoperative value. We compared normally distributed continuous variables between groups using unpaired Student t tests and abnormally distributed data using the Mann-Whitney test. We analyzed the categorical variables using the Pearson chi-square test, and the Pearson correlation coefficient was used to evaluate associations between cough and thoracic pain, as well as thoracic pain and FVC. We performed statistical analysis using GraphPad Prism 3.0 software (GraphPad Software, San Diego, California). P < .05 was considered statistically significant.
Results
We assessed 638 subjects for eligibility in our study. Of these, we allocated 500 subjects into 2 groups and analyzed 450 subjects (Fig. 2).
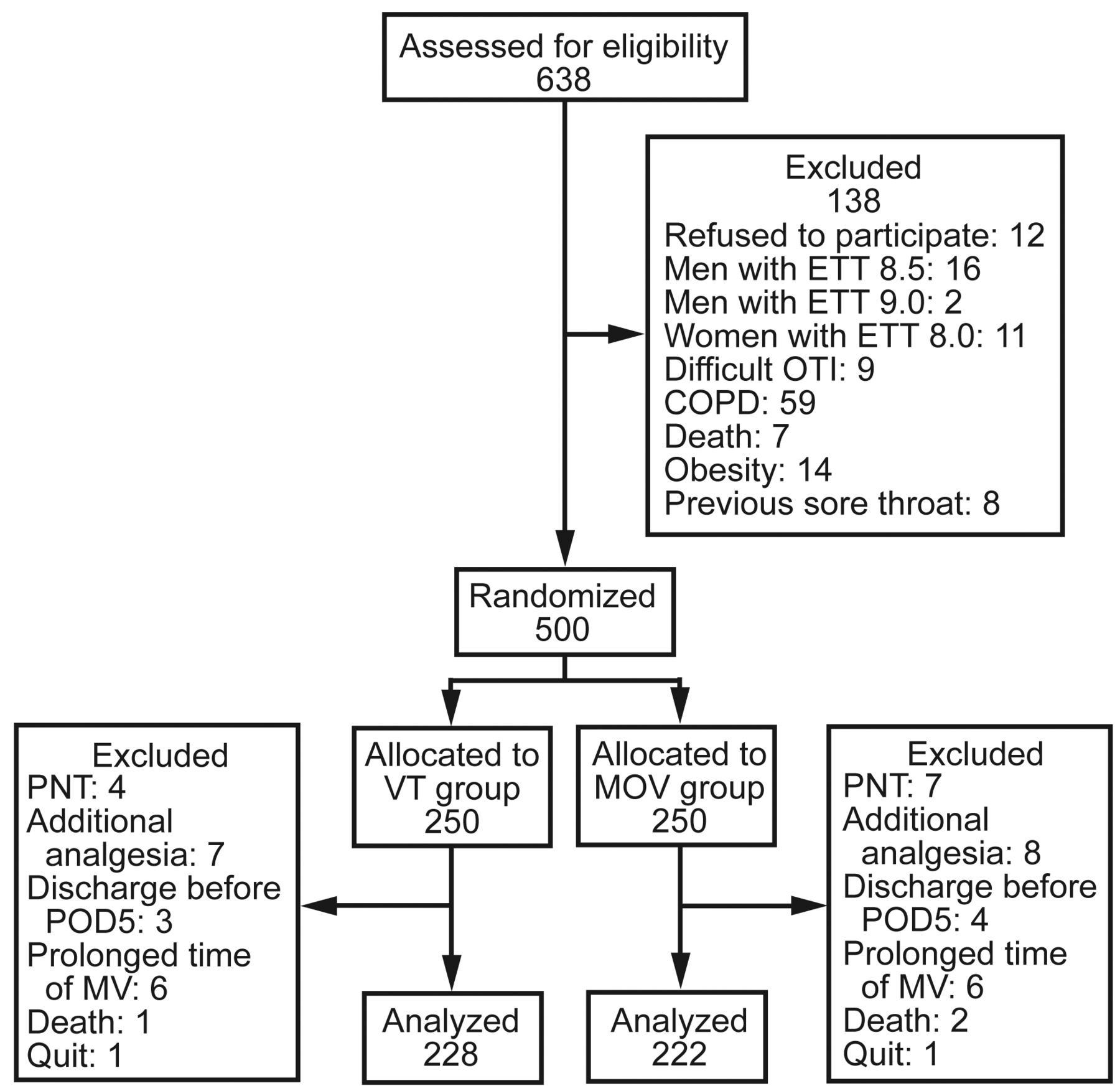
Study flow chart of the trial. ETT = endotracheal tube; OTI = orotracheal intubation; PNT = placement of nasogastric tube; POD5 = 5th postoperative day; MV = mechanical ventilation; VT = volume-time curve group; MOV = minimal occlusive volume group.
The groups were homogeneous in terms of age, gender, body mass index, preoperative pulmonary function, time of intubation, type of surgery (on-pump or off-pump coronary artery bypass grafting), and pleural opening. Perioperative subject characteristics are summarized in Table 1.
Preoperative and Intra-operative Clinical and Demographic Characteristics
The volume-time curve group showed a significantly lower cuff pressure compared with the MOV group: 30.9 ± 2.8 and 37.7 ± 3.4 cm H2O, respectively (P < .001).
Both groups presented evidence of sore throat at 1 h after extubation. However, the incidence of sore throat was significantly lower in the volume-time curve group compared with the MOV group (P < .001). After 24 h, this difference remained significantly higher when the MOV technique was applied (P < .001). Seventy-two h after extubation, the volume-time curve technique presented less severe sore throat, without a significant difference between the groups (P = .11). Of the 450 subjects analyzed, a small number of subjects had residual symptoms of sore throat after 120 h, without a significant difference between compared (P = .48) (Table 2).
Comparison of Values Between the Groups for Postoperative Sore Throat
The sore throat intensity was significantly less in the volume-time curve group compared with the MOV group at 1 and 24 h after extubation (P < .05). The subjects graded their discomfort as mild to severe in the MOV group and as mild to moderate in the volume-time curve group (Fig. 3).
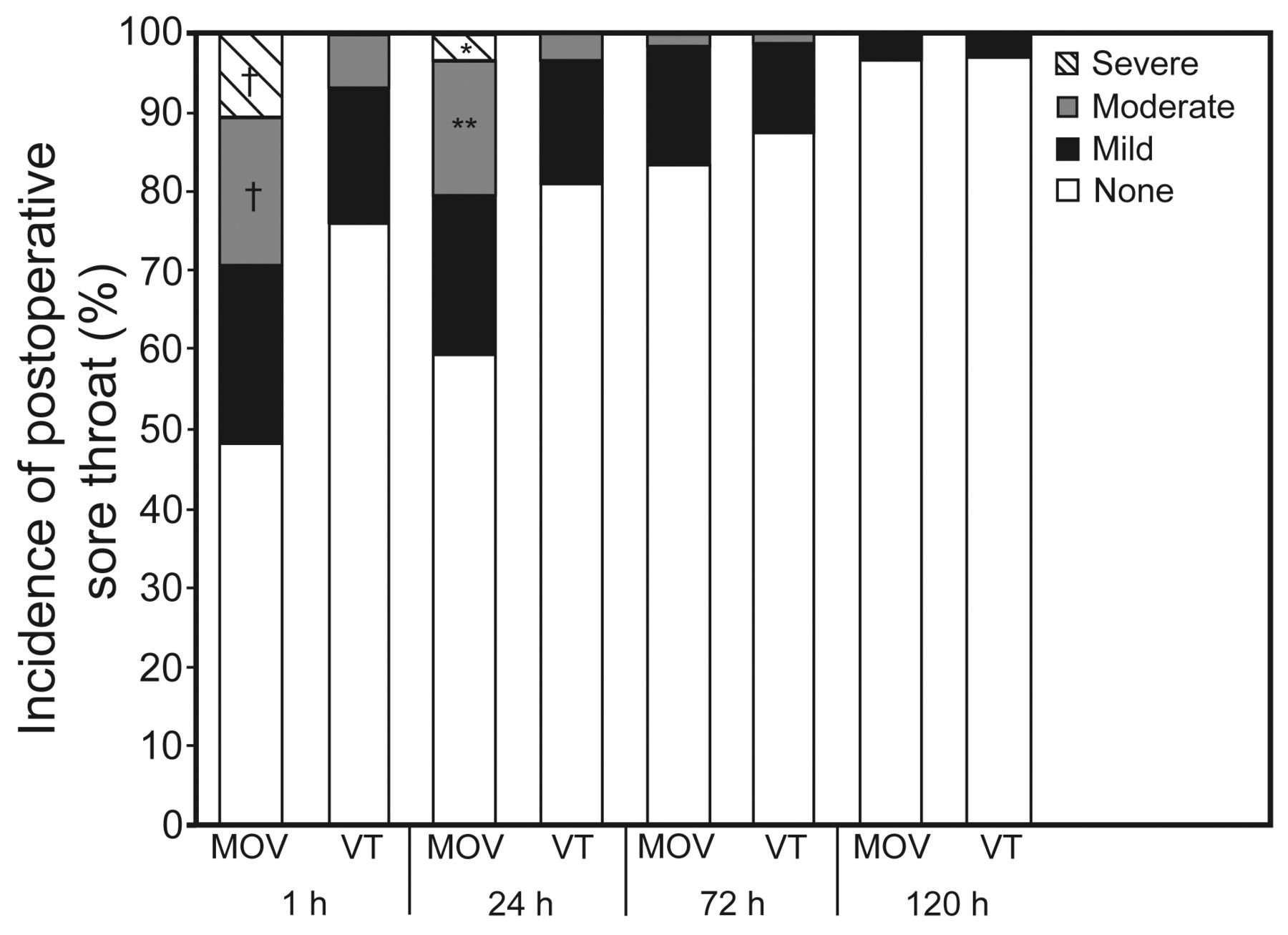
Postoperative incidence of sore throat from mild to severe in the minimal occlusive volume group (MOV) compared with incidence of sore throat from mild to moderate in the volume-time curve group (VT). † P < .001; * P = .006; ** P = .002.
The incidence of coughing episodes was shorter in the volume-time curve group compared with the MOV group at 1 and 24 h after extubation (P < .001). A few subjects had coughing episodes after 72 h (P = .14), and none had coughing episodes after 120 h in either group (Table 3). In relation to the graduated coughing episodes, the volume-time curve group graded these episodes as less frequent and sustained than did the MOV group (P < .05) (Fig. 4). The subjects graded their thoracic pain as less severe in the volume-time curve group (5.2 ± 1.8) compared with the MOV group (7.1 ± 1.7, P < .001).
Comparison of Values Between the Groups for Postoperative Cough

Postoperative incidence of cough, from no cough to sustained coughing, in the minimal occlusive volume group (MOV) compared with the volume-time curve group (VT). † P < .001; * P = .005.
Both groups showed a significant decrease in pulmonary function at 24 h after extubation. However, a significant difference was observed when the groups were compared. The FVC mean, expressed as a percentage of the preoperative value, was significantly higher in the volume-time curve group than in the MOV group (49.5 ± 9.9 vs 41.8 ± 12.9%, P = .005). Similar results were found for FEV1 (46.6 ± 1.8 vs 38.6 ± 1.4%, P = .005). There were significant correlations between cough and thoracic pain (r = .71, P < .01) and also between thoracic pain and FVC (r = −0.73, P = .02).
Discussion
In this study, the volume-time curve technique was associated with lower cuff pressure and less occurrence of sore throat and coughing episodes compared with the MOV technique in subjects who underwent coronary artery bypass grafting during the first 24 h after extubation. To our knowledge, this is the first study that compared the occurrence of sore throat and coughing episodes after endotracheal extubation between volume-time curve and MOV techniques for cuff inflation. Our previous investigation demonstrated that the volume-time curve technique could be a more reliable alternative for ETT cuff management compared with the MOV technique.3 However, the focus of this study was comparison of the ETT cuff volume and cuff pressure generated after both techniques were used. Therefore, our study is unique because of the evaluation of the clinical impact that resulted from these 2 techniques for ETT cuff inflation.
Several studies argued that the best way to adjust the cuff pressure properly would be to use the MOV technique, also known as the seal pressure technique.2–5 Using this technique, we can slowly inflate the cuff until the air leak stops during the inspiratory phase of positive-pressure ventilation.12 Documentation has suggested that the MOV technique can be an inaccurate method for promoting adequate cuff inflation because it might result in overinflated cuff pressure to seal the airway.3 Studies have shown that increased cuff pressure can contribute to the development of tracheal mucosa injuries, sore throat, and coughing episodes after endotracheal intubation.1,13 For this reason, the presence of sore throat and coughing after extubation has been extensively studied, and various techniques have been proposed to minimize these symptoms.1,9,10,13–16
In this study independent of the technique (MOV or volume-time curve), we found a significant occurrence of sore throat and coughing at 1 and 24 h after extubation. However, the incidence of sore throat was shorter in the volume-time curve group. Additionally, the incidence of coughing immediately after surgery was considerably lower in the volume-time curve group compared with the MOV group, which demonstrates a beneficial effect of the volume-time curve in minimizing the irritation stimuli of the ETT cuff on the tracheal mucosa. The cuff pressure was 18% higher in the MOV group compared with the volume-time curve group. Our data demonstrated that in the early postoperative period, the MOV group had almost a double risk for developing sore throat and cough compared with the volume-time curve group. On the basis of these findings, we believe that the volume-time curve technique is less subjective and permits a more appropriate cuff adjustment in the trachea that results in minor cuff pressure and a lower incidence of sore throat and cough. Suzuki et al17 supported these findings: the higher the cuff pressure, the higher the sore throat occurrence.
Reports have documented that the symptoms from a sore throat usually resolve within 72 h.1,13 In our study, ∼12.27% of the subjects in the volume-time curve group and 16.21% in the MOV group presented some degree of sore throat after 72 h. The reason for these persistent symptoms might be related to the higher intubation time that our subjects endured compared with those subjects reported by other researchers. The literature suggests that the incidence of sore throat after ETT removal increases proportionally with endotracheal intubation time, which is most likely attributed to a longer period of compression on the trachea, worsening the local ischemia.13,18 As expected, after 120 h, a few of our subjects had residual sore throat symptoms. According to these data, we assumed that the MOV technique might be associated with a higher risk of tracheal damage related to the increased cuff pressure presented.
The intensity of the sore throat was also greater in the MOV group compared with the volume-time curve group. When the subjects graded their discomfort, the MOV technique was associated with a mild-to-severe intensity of sore throat, and the volume-time curve technique was associated with a mild-to-moderate intensity of sore throat symptoms. The coughing episodes were more sustained when the MOV technique was applied. We believe that the lower grades of coughing episodes and lower sore throat discomfort scores might be related to the lower cuff pressure achieved when the volume-time curve technique was applied.
In a similar study comparing 2 techniques for cuff inflation, Liu et al1 found a good correlation between ETT cuff pressure and presence of tracheal pain. Although the symptoms are always subjective, these authors suggested that the severity of symptomatology might be proportional to the degree of tracheal mucosa injury. Therefore, we speculate that the less discomfort generated by sore throat and lower grades of coughing episodes in the volume-time curve group could be related to less tracheal mucosa injury.
Previous studies have shown that pulmonary dysfunction in postoperative subjects after coronary artery bypass grafting is inevitable.19–24 Similar results were found in our study. Conventionally, coronary artery bypass grafting involves trauma to the rib cage, which causes pain that can be intensified by coughing. Milgrom et al25 reported that cough is most painful after open-heart surgery. Because of thoracic pain, the subject reacts with superficial breathing, and deep breathing may be restricted, reducing pulmonary volumes and capacities.26,27 Consequently, a major incidence of respiratory complications during the postoperative course may occur and delay pulmonary function recovery.28,29 This may explain our findings. The MOV group, which presented a higher incidence of cough and consequently more thoracic pain, demonstrated a greater impairment in pulmonary function at 24 h after the extubation, as demonstrated by the correlation tests applied in this study. On the basis of these results, we believe that the subjects who received the volume-time curve technique presented better pulmonary function preservation and would be less vulnerable to present pulmonary complications postoperatively after coronary artery bypass grafting.
Patients submitted to a prolonged time of mechanical ventilation may be susceptible to a higher degree of tracheal mucosa injury.2 Unfortunately, in this study, the volume-time curve technique was not evaluated in a general population of ICU patients. However, this research assumes clinical importance due to the capacity of the volume-time curve to identify in real time the exact volume of air to fill the cuff to prevent air leakage, thus resulting in lower cuff pressure and fewer endotracheal intubation-related respiratory symptoms. Because most mechanical ventilators have graphic monitoring, the volume-time curve technique could be easily applied in clinical practice.
This study has some limitations. For ethical considerations, we did not conduct a histological study in subjects to evaluate possible injuries to the tracheal mucosa secondary to the cuff pressure achieved. We did not perform fiberoptic bronchoscopy at the time of extubation, so we could not observe or confirm the severity of the tracheal mucosa injuries. The major limitation of this study is that all of the patients had been submitted to the same analgesic regime. Not all patients experience pain in the same way. This could confuse chest pain secondary to cough with the additional analgesia requirement. In an attempt to avoid bias, patients requiring additional analgesia were excluded, and the Pearson correlation coefficient test was applied to the variables of cough and chest pain and also chest pain and FVC.
Conclusions
The subjects who received the volume-time curve technique for ETT cuff management presented a significantly lower incidence and severity of sore throat and cough, less thoracic pain, and minimally impaired pulmonary function than those subjects who received the MOV technique during the first 24 h after coronary artery bypass grafting.
Footnotes
- Correspondence: Walter Jose Gomes PhD MD, Escola Paulista de Medicina, Avenida Dr Bacelar 395, Federal University of São Paulo, São Paulo 04042-004, Brazil. E-mail: wjgomes.dcir{at}epm.br.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1810
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}