

Abstract
INTRODUCTION: Respiratory muscle strength (RMS) is a determinant of vital capacity, and its decline can lead to inadequate ventilation and deficiency in the elimination of secretions from the airways. Studies analyzing RMS in older adults with Parkinson's disease (PD) and Alzheimer's disease (AD) remain scarce, making the analysis of this variable still very uncertain. The aim of this study was to analyze the RMS of older adults diagnosed with PD and AD, in relation to healthy control peers.
METHODS: A cross-sectional study was conducted involving 65 older adults comprising 3 groups: PD (n = 20), AD (n = 20), and control (n = 25). The participants underwent anthropometric and cirtometric measurements associated with maximal respiratory pressures. We analyzed data using descriptive (mean and SD) and inferential statistics (1-way analysis of variance, Student t test, and Scheffé post hoc) with a level of significance of 5% (P < .05) and a CI of 95%.
RESULTS: Although the anthropometric and cirtometric variables indicated similarity of values between groups (P > .05), the maximal inspiratory and expiratory pressures were considerably lower in the subjects with PD and AD (P < .01).
CONCLUSIONS: The control of the anthropometric and cirtometric variables of the subjects indicates that RMS is affected by the aging process, and its decline increases in neurodegenerative conditions. This fact represents a serious risk for the development of atelectasis and other pneumo-functional complications, which must be considered in proposing of future therapies.
- Parkinson's disease
- Alzheimer's disease
- airway pressure
- respiratory function tests
- public health
- critical care
Introduction
Respiratory dysfunctions represent serious problems for the population's health and are related to growing rates of co-morbidities and deaths. With the physiological process of aging, lung function undergoes changes in capacity, volume, and respiratory flow, caused by the loss of elasticity of pulmonary tissue, alveolar dilatation, and drops in the neural transmission and stimuli in the respiratory muscles.1,2 Respiratory muscle strength (RMS) is a determinant of the subjects' vital capacity, and its decline can lead to inadequate ventilation, particularly when linked with chronic neuromuscular conditions.3,4
Lower pulmonary function has been correlated with poor cognitive performance in patient populations as well as in community-dwelling subjects with a wide range of health statuses and ethnicities.5 However, studies evaluating RMS in neurodegenerative illnesses, such as Parkinson's disease (PD) and Alzheimer's disease (AD), remain scarce and with little scientific evidence.6
Regarding PD, it is important to emphasize that it is a progressive disorder characterized by the presentation of clinical signs of bradykinesia, rigidity, tremor at rest, and impairment of postural reflexes.7 In addition to this, the illness can lead to obstruction of the upper airways, restrictive defects, and inadequate ventilatory control.8
On the other hand, AD is characterized as one of the most prevalent causes of dementia in the world. It originally affects the basal nucleus of Meynert and is defined post mortem by the presence of amyloid plaques and neurofibrillary tangles.9 Its relation to dysfunctions of the respiratory tract can be linked with the subject's physical decline, arising, above all, from the depletion in the levels of acetylcholine and changes in the N-methyl-d-aspartate receptors in the brain.10,11
Although these conditions present psychological-behavioral and neuromotor impairments as the principal dysfunctions, one must also consider the influence of the brain alterations in RMS. Hence, it is necessary to evaluate the subjects' pulmonary function so as to ascertain the need to establish a guided and efficacious therapeutic plan for patients with such conditions.
This study aimed to analyze the maximum RMS (inspiratory and expiratory) of older adults diagnosed with PD and AD in relation to healthy control peers.
QUICK LOOK
Current knowledge
Respiratory muscle strength is a determinant of vital capacity, and its decline can lead to inadequate ventilation and secretion retention. Neurologic and neuromuscular diseases and increasing age conspire to reduce respiratory muscle strength.
What this paper contributes to our knowledge
Respiratory muscle strength is affected by the aging process, and its decline increases in neurodegenerative conditions, including Alzheimer's and Parkinson's disease.
Methods
In this cross-sectional study design, 65 males and females (60–80 y of age at entry) were recruited into three groups: PD (20 older adults diagnosed with PD,12 who were in stages 2, 3, or 4 of the Hoehn-Yahr scale13), AD (20 older adults with AD,14 who were in the moderate stage on the Clinical Dementia Rating15), and control group (CG, made up of 25 older adults). We allowed for a 5% margin of error, an effect size of 0.40, and a statistical power of 80% to calculate the necessary sample size. Based on this calculation, the sample size should be 65 subjects.
This study was performed at the Neurologic Outpatient Clinic of University Hospital (Campo Grande, Mato Grosso do Sul, Brazil), and all patients enrolled in the study were selected from this clinic. Ethical approval was obtained from the local research ethics committee (protocol 31,834), and this study complied with the Helsinki Declaration. Informed consent forms were signed by all subjects participating in this study. For AD subjects, the patient's next of kin (usually the main family caregiver) was approached to give informed consent.
With respect to the inclusion criteria, subjects were admitted with the clinical conditions described,12,14 all sedentary (not performing any physical activity superior to 3 metabolic equivalents of task), and independent for orthostatism and locomotion. A history of tobacco use, previous respiratory conditions (such as COPD, asthma, bronchitis, pneumonia, tuberculosis, sarcoidosis, or neoplasias), thoracic alterations (barrel chest, pigeon chest, excavatum, carinatum, or kyphoscoliotic) and serious cognitive decline, evidenced by a score < 5.0 on the mini-mental state examination16 (which would make it impossible for the participants to understand the tasks adequately) were stipulated as exclusion criteria. Cases involving dementia in PD and mixed dementias (Alzheimer's plus vascular) were also excluded.
Subjects were selected by referral from a doctor (neurologist or psychiatrist), with the predefined clinical diagnosis. Control subjects were selected during the same time period of case recruitment. The control group was essentially a convenience sample, selected to match the profile of the subjects with AD and PD.
No subject had renal or cardiac dysfunctions. Those with diabetes mellitus type 2 and hypertension were controlled under normal parameters. Furthermore, none of the participants had been hospitalized in the last 6 months or received any respiratory physical therapy.
Evaluative Procedures
The evaluative procedures involved the measuring of the thoracic cirtometry (cm), standardized in the subject's right and left armpits. For the analysis of the participants' RMS, a previously-calibrated manometer, graduated in cm H2O was used.
The cirtometry consisted of measuring the chest circumference with a measuring tape. The standardized procedure was to keep the 0 point of the tape fixed on the midline of the body, horizontally aligned with the landmarks, while the other end of the tape was allowed to move. The tape was snug but not tight, so that the soft-tissue contours remained unchanged. For this measurement, the subjects were asked to perform maximum inspiration and expirations twice, and to hold the maximum inspiration or expiration for at least 2 s, during which the measurements were taken.17 Through this procedure, it was possible to analyze the thoracic mobility in the situations of normal respiration and sustained maximum inspiration and expiration.
Maximum inspiratory pressure (PImax), followed by maximum expiratory pressure (PEmax), was obtained starting at residual volume or total lung capacity, respectively, with the subject seated (maintaining 90° of flexion in their knees and hips), wearing a nose clip, and with a rigid, plastic, flanged mouthpiece. A small leak was introduced between the occlusion and the mouth to prevent glottic closure, and the subject held his or her cheeks with one hand during the maneuver. Due to the evaluative standards previously accepted in the literature,18 this maneuver was undertaken 5 times, with a minimum of 3 correct measurements being accepted, technically characterized as: (1) absence of air leaks in the procedure, (2) minimum duration of 3 s, (3) a gross value that did not exceed the other accepted values by 10.0%, and (4) the last value not being higher than the others (which would entail the undertaking of a new respiratory maneuver).
Before the test, we assessed the ability of subjects to demonstrate proper task performance. Subjects with PD and AD were tested while on their medications: the PD subjects using drugs for which the active ingredient was based on dopamine, and the AD subjects using drugs for which the active ingredients were based on inhibitors of the acetylcholinesterase enzyme and N-methyl-d-aspartate receptor antagonists.
Statistical Analysis
We analyzed data using descriptive statistics (mean, SD, and percentage analysis) to characterize the sample, and inferential statistics to compare the values obtained between groups.
We complied with the precepts of normality and homogeneity required by the parametric statistics. Thus, the cross-sectional analysis obeyed the following system: if the variable presented a continuous character, 1-way analysis of variance was applied. The Scheffé post hoc test was applied for comparing the results between the groups, and the Student t test for independent samples was applied for comparing values between men and women from each group.
If the variable had a nominal categorical character, the nonparametric chi-square test was applied. A level of significance of 5% (P < .05) with a CI of 95% was considered in all the analyses.
Results
Sixty-five older adults participated in this study, of whom 29 were men (44.6%) and 36 were women (55.4%). The subjects' mean age was 72.26 ± 7.93 y old, and all were resident in the city of Campo Grande, in the state of Mato Grosso do Sul, Brazil. Table 1 shows the groups' characteristics in relation to gender, age, weight, height, body mass index, and cognitive functions.
Subject Characteristics
As may be observed in Table 1, the groups analyzed were homogeneous regarding sample size (P = .68), gender (P = .78), height (P = .38), weight (P = .27), and body mass index (P = .48). In relation to the participants' ages, differences were found between the groups (P = .01), being evidenced in the comparisons between the Parkinson's and Alzheimer's groups (P = .03, 95% CI = −11.95 to −0.34) and between the Alzheimer's and control groups (P = .01, 95% CI = 0.34 to 11.95). Regarding the cognitive score evaluated in the mini-mental state examination, there was a significant difference between the groups (P = .01), particularly in the comparisons between the Alzheimer's and Parkinson's groups (P = .01, 95% CI = −11.56 to −2.81) and the Alzheimer's and control groups (P = .01, 95% CI = −11.03 to −2.37).
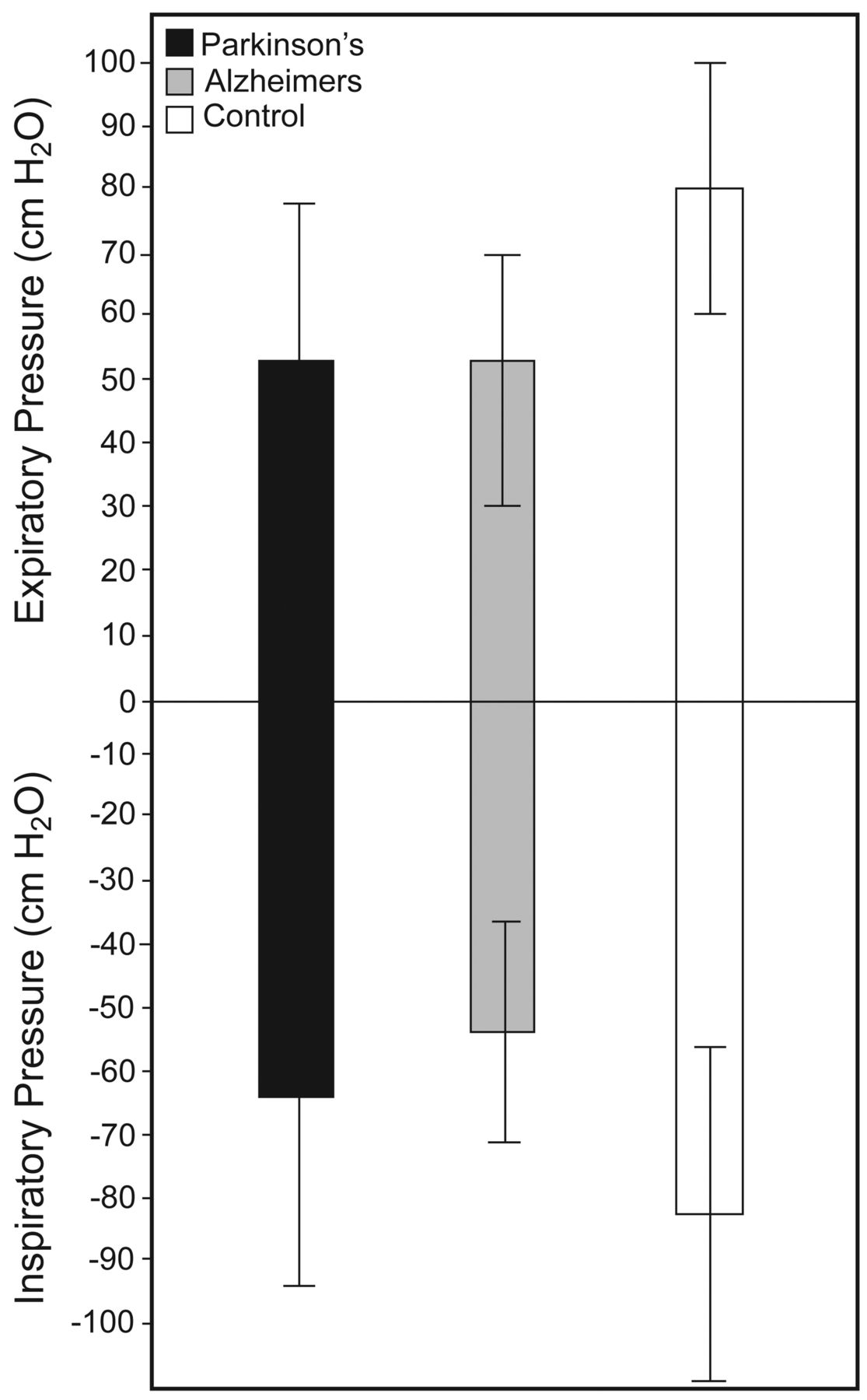
PImax and PEmax Values
Figure 1 details the PImax and PEmax values. The statistical analysis indicated differences between the groups both for inspiratory strength values (P = .01) and for maximum expiratory values (P = .01). Although different values were found for PImax and PEmax, no participant presented with dyspnea or other respiratory complaints during the evaluation.

Maximum inspiratory and expiratory values for each group. Data are shown as mean ± SD.
Regarding pairwise comparisons, a significant difference of PImax was observed between the Alzheimer's and control groups (P = .01, 95% CI = −46.30 to −11.85) and a tendency of significance between the Parkinson's and control groups (P = .06, 95% CI = −37.1 to .58). In relation to the PEmax, the comparison evidenced a difference between the Parkinson's and control groups (P = .01, 95% CI = −46.01 to −11.55), and between the Alzheimer's and control groups (P = .01, 95% CI = −46.31 to −11.85).
PImax and PEmax by Gender
Table 2 shows the PImax and PEmax values of the groups by the participants' gender, compared against the mean ages of the same and the staging of PD and AD in the respective groups.
Mean and SD of the Values for Maximum Inspiratory Pressure and Maximum Expiratory Pressure by Gender
Through the Student t test for independent samples, we observed that there was no significant difference between the mean ages for men and women in the Parkinson's group (P = .63, 95% CI = −5.71 to 9.16), Alzheimer's group (P = .73, 95% CI = −4.53 to 6.28), and control group (P = .86, 95% CI = −6.47 to 7.67). In relation to the extent of the progression of the participants' illnesses, there was no difference between the staging in comparisons between men and women from the Parkinson's (P = .96, 95% CI = −0.48 to 0.50) and Alzheimer's group (P = .60, 95% CI = −0.37 to 0.62), indicating statistical similarity.
Regarding the values referent to the PImax, we observed a significant difference between the sexes only in the Parkinson's group (P = .02, 95% CI = 3.57 to 51.27). In relation to the PEmax values, we observed a significant gender difference in the Parkinson's group (P = .02, 95% CI = 3.50 to 50.43) and in the Alzheimer's group (P = .04, 95% CI = 0.93 to 35.48).
Thoracic Cirtometry
Figure 2 shows the variation of thoracic amplitude in the Parkinson's, Alzheimer's, and control groups. According to 1-way analysis of variance, no difference was observed between the groups in relation to: (1) basal thoracic amplitude (P = .32), (2) inspiratory thoracic amplitude (P = .34), and (3) expiratory thoracic amplitude (P = .37).
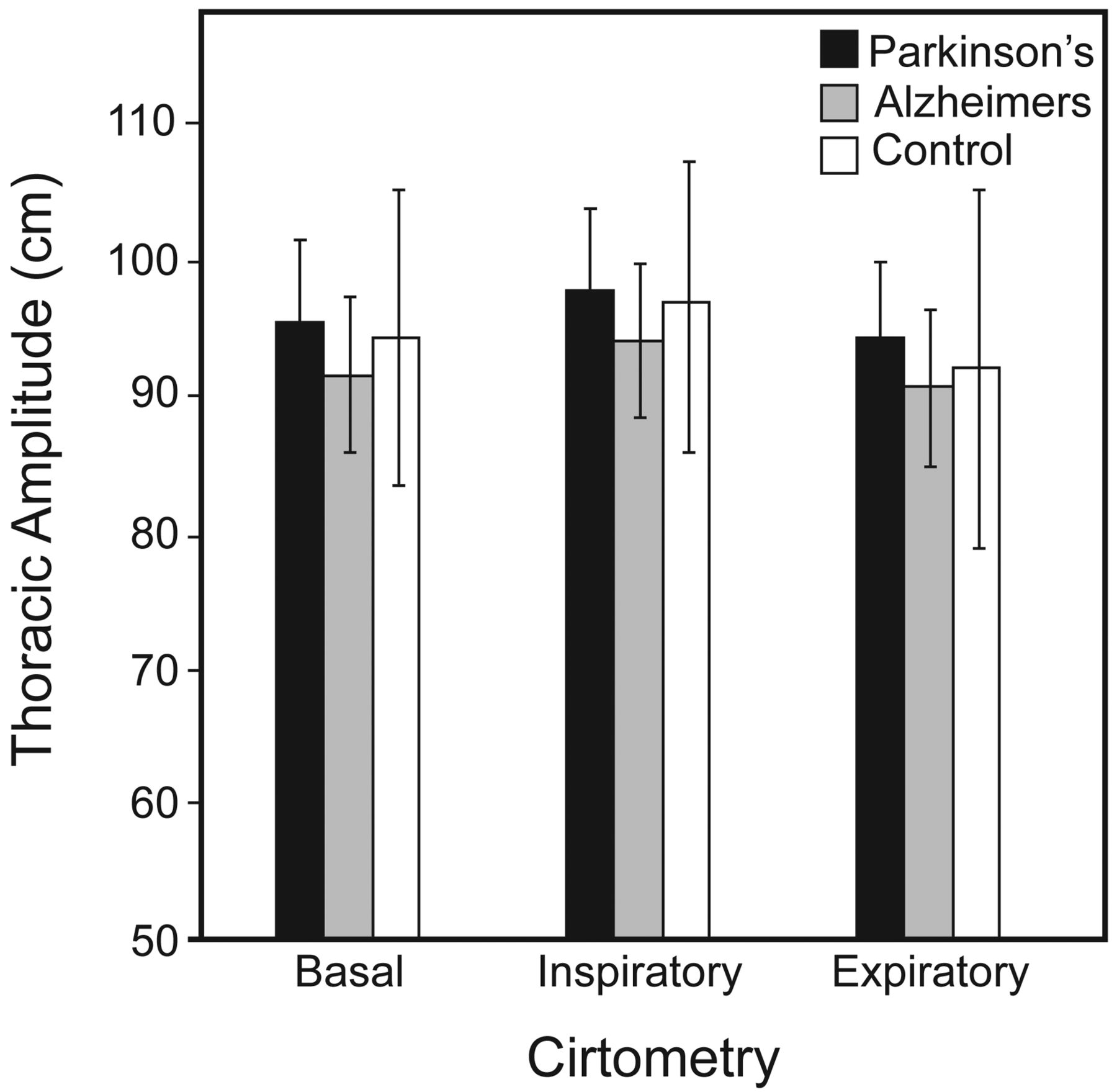
Variation of cirtometric measurements for each group. Data are shown as mean ± SD.
Thoracic Cirtometry By Gender
In relation to the cirtometric amplitude by gender, there was no difference between the men and women in the basal amplitude of the Parkinson's (P = .47, 95% CI = −3.76 to 7.76), Alzheimer's (P = .10, 95% CI = −1.02 to 9.48), and control groups (P = .10, 95% CI = −1.57 to 16.10). Regarding analysis by gender involving maximum inspiratory amplitude, there was also no difference in the Parkinson's (P = .67, 95% CI = −2.80 to 8.63), Alzheimer's (P = .10, 95% CI = −1.01 to 9.59), and control groups (P = .07, 95% CI = −0.56 to 16.42). The same result was obtained in the comparison by gender on the maximum expiratory amplitude in the Parkinson's (P = .57, 95% CI = −4.17 to 7.24), Alzheimer's (P = .09, 95% CI = −0.81 to 9.94), and control groups (P = .90, 95% CI = −1.57 to 20.03).
Discussion
The aging process exercises a large influence on respiratory parameters. The increase in the abdominal cavity, the reduction in pulmonary elasticity, the rise in pulmonary vascular resistance, and the generalized muscular weakness are some factors involved in the pneumo-functional decline of the older adult.19 When associated with pathological processes, the changes are accentuated, and may compromise the subjects' routine activities.
We decided to use the manometer as an instrument for measuring maximum muscular strength for two reasons: first, it represents a highly sensitive method for cases of inspiratory muscular weakness (PImax), and second, it reflects a parameter of the subjects' effectiveness of cough and expectoration (PEmax).20 The results found in this study indicate that older adults with PD and AD, even presenting anthropometric and cirtometric characteristics that are similar to those of healthy older adults, have greater compromise of maximum RMS (inspiratory and expiratory). In this case, understanding respiratory physiology and the influence of nosological conditions on this process is fundamental for reflection on the clinical findings.
Human respiration consists of an automatic body function, which depends on extrinsic motor command. The diaphragm, the principal human respiratory muscle, receives input from the phrenic motor neuron, originating from three main pathways: (1) the bulbo-spinal pathway, responsible for promoting the rhythmic respiratory pattern; (2) the cortico-bulbar-spinal pathway, which is involved, through its connection with the limbic system, in the modulation of respiration by emotion; and (3) the upper cortical pathways, which regulate respiration according to the synergic activation of other cerebral areas, such as speech or singing, for example.21,22 Thus, it is possible to assert that changes in one of these pathways may affect the efficacy of the muscle of the diaphragm.
The respiratory problems that older adults with PD present reflect the compromised values of PImax and PEmax, and result in situations of obstruction of the upper airways, restrictive disorders, and complications arising from aspiration.23 Mehanna and Jankovic24 hypothesized that the respiratory dysfunctions in PD may be the result of muscle dystonia causing abnormal rhythmic oscillations in the supraglottic structures. In addition to this, rigidity, freezing, and bradykinesia exacerbate the restrictive pulmonary dynamic, which, associated with the inefficacy of the cough reflex, predisposes the subject to an elevated risk of aspiration pneumonia.23,24
In spite of the most striking pathological modification in PD being the degeneration of the mesencephalic substantia nigra, recent studies prove that apoptotic processes suffered in the illness involve neuronal lesions adjacent to the basal nuclei that affect brainstem, locus coeruleus, and upper cerebral regions.25 Because of their compromised connective pathways, this study's clinical findings, which proved there were shortcomings in the patients' maximal respiratory strength (PImax and PEmax), are substantiated.
However, AD studies indicate respiratory complications as being a co-adjuvant outcome of the illness, affected above all by the patient's physical decline and total dependence in the final stage of the illness. Easterling and Robbins26 describe dysphagia and pulmonary aspiration as complications related to the process of human aging, and state that they are exacerbated in AD.
As the reduction in the sensitivity of the pharynx, the loss of dentition, the reduction in the capacity to produce saliva, and the slowing of the oral-pharyngeal reflex are signs common to old age, the structural alterations that occur in the brain of the patient with AD (with apoptosis and neuro-fibrillary tangles in cortical and sub-cortical regions) affect the efficacy of the pulmonary dynamic. In addition, the human cardiopulmonary capacity is directly influenced by the autonomic nervous system. In this context, Zakrzewska-Pniewska et al27 demonstrate that sympathetic and parasympathetic involvement occurs in AD in varying degrees, which may be related to the findings of PImax and PEmax demonstrated in this study.
Studies have had difficulty predicting a reference value for PImax and PEmax in the Brazilian population. Although Neder et al,28 analyzing the same age range as the present study, found normality of PImax values of −92.8 ± 72.8 cm H2O for men and −72.7 ± 3.9 cm H2O for women, Simões et al29 observed values of −74.0 ± 4.5 cm H2O for men and −57.6 ± 5.1 cm H2O for women. Regarding PEmax, there was also the same discrepancy of values: Neder et al28 found values of 111.5 ± 21.0 cm H2O for men and 69.6 ± 6.7 for women, and Simões et al29 observed values of 71.0 ± 4.5 cm H2O for men and 57.8 ± 4.7 cm H2O for the women. Despite use of the same methodology, the difference seen might be the result of differences in sample size. According to the values set up in the control group, the present study is closer to the reference values found by Simões et al.29
Because of the male biotype, it is common for the reference values for PImax and PEmax to be slightly higher in men than in women, although this does not necessarily indicate a significant difference between the sexes. The present study corroborates this fact, apart from the values of the Parkinson's group, which were shown to be perceptibly lower in women compared with men. Regarding this, various convergent factors explain this finding, representing an important influence of women's anthropometric, clinical, and bioimpedance variables, in relation to men.
Excess weight and obesity are major clinical and public health problems worldwide.30 In our study, the average body mass index for participants puts them in the overweight category. Related to that, it is known that excess body fat influences lung function by mechanical and nonmechanical mechanisms; therefore, this could have affected the results.31 However, the homogeneity of the groups in this variable minimizes this bias by exercising a similar effect in each group.
Nonetheless, the mobility of the thoracic cage may represent one bias of the studies which address the subjects' pneumo-functional characteristics, as it exercises a direct influence on the patients' RMS.32 When we undertook the cirtometric evaluation of all subjects and observed statistical similarity between groups in the comparisons of the thoracic amplitude (normal respiration, maximum inspiration and expiration), we provided support to affirm that this factor does not exercise any influence on the subjects' PImax and PEmax values. In addition to this, the exclusion of patients with possible alterations in the thoracic dynamic (commonly present in cases of barrel chest, pigeon chest, excavatum, carinatum, or kyphoscoliotic), made it possible for us to isolate this bias in the sample selection.
Furthermore, PD and AD are neurodegenerative conditions that cause a serious global decline in health for older adults, being commonly related to a high risk of falls and the subject's physical-functional dependence.33 Had the sample been heterogeneous in terms of the level of physical activity and the degree of functional independence, we would have been able to evaluate the influence of both processes on pneumo-functional values.34 Thus, we opted to restrict the sample to sedentary subjects who presented similar functional levels.
It is important to say that all subjects with PD and AD were evaluated while on their medications. We chose to maintain this delimitation, as previous studies show that medication based on dopamine (for PD) does not exercise any influence on the subjects' parameters of PImax and PEmax, just like medication based on acetylcholinesterase inhibitors and N-methyl-d-aspartate antagonists (for AD), which have a neuro-psycho-behavioral action.23,35
Limitations
Although we believe this study does have merits, the limitations should be pointed out. One limitation is that we used cross-sectional data that do not allow us to assess causal relationships. Longitudinal research aimed at assessing the predictive value of pulmonary functions is needed to better understand the mechanisms whereby the central nervous system affects PImax and PEmax in later years and to identify possible target areas for interventions.
Despite our having found differences between the subjects' ages, it is important to survey the mean age of the participants in this research. Benchmark studies previously published in the literature28,29 usually classify the subjects in age ranges of 10 y, indicating that possible differences in RMS from year to year are minimal. Thus, it is possible to assert that the age difference found in this study had little influence on the results.
Although one may argue about the small sample size, one has to consider the difficulty of recruiting subjects, as well as the fact of both pathologies presenting a complex diagnosis, requiring the integration of clinical evaluation with laboratory tests that are not always available. In AD, for example, the definitive diagnosis is undertaken by cerebral autopsy. In life, the use of structural neuroimaging exams (hippocampal volumetry, for example) and those of functional neuro-imaging (magnetic resonance spectrossist in making an accurate diagnosis. In PD, however, the difficulty in diagnosis is in differentiating idiopathic PD from Parkinsonian syndromes, which are secondary to cerebral compromise.
As our study involved the analysis of respiratory function, the use of another study center, with subjects living in another city, under another climate condition, air humidity, and pollution level could be a bias. Based on that, we restricted our sample to subjects living in Campo Grande, Mato Grosso do Sul, Brazil, a city located in the tropical region, with 8,096 km2 of area, 113,862 hectares of natural reserve, and pollution level in agreement with that recommended by the World Health Organization.36
Conclusions
This study observed an important reduction in the maximum RMS in older adults with PD and AD, when compared with healthy control subjects. The groups' similarity in socio-demographic and cirtometric variables indicates that the PImax and PEmax values of the Parkinson's and Alzheimer's groups are more associated with the alterations arising from the clinical situations than from the aging process per se.
This fact represents a serious risk for developing atelectasis and other pneumo-functional complications, and must be considered in proposing future therapies. Additional studies should investigate a larger and more heterogeneous sample to ensure that the results are applicable to the general populations of PD and AD patients.
Acknowledgments
We thank the National Council for Scientific and Technological Development (CNPq) for technical and scientific support.
Footnotes
- Correspondence: Gustavo Christofoletti PhD, Federal University of Mato Grosso do Sul, Biological and Health Science Center, Curso de Fisioterapia, Avenida Universitária, s/n, Setor Universitário, Caixa postal 549, 79060-900 Campo Grande, Mato Grosso do Sul, Brazil. E-mail: g.christofoletti{at}ufms.br.
Dr Christofoletti presented a version of this paper at the 11th International Conference on Alzheimer's and Parkinson's Diseases, held March 6–10, 2013, in Florence, Italy.
The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}