

Abstract
BACKGROUND: Randomized trials and meta-analyses have reached conflicting conclusions regarding the risk benefit ratio of thrombolytic therapy or anticoagulant therapy in patients with moderate pulmonary embolism. To investigate the effect of initial thrombolysis and anticoagulant therapy in patients with moderate pulmonary embolism, we performed an updated meta-analysis.
METHODS: We searched the MEDLINE, Embase, Cochrane Library, Wanfang, and CNKI databases for randomized controlled trials focusing on moderate pulmonary embolism. We then performed a meta-analysis of all randomized trials comparing thrombolytic therapy with heparin treatment in subjects with moderate pulmonary embolism.
RESULTS: Fifteen trials involving 1,247 subjects were included. Compared with anticoagulation, thrombolytic therapy was associated with a significant reduction in recurrent pulmonary embolism or death (1.94% vs 5.87%, odds ratio (OR) of 0.37, 95% CI 0.21–0.66, P for heterogeneity = .49), a nonsignificant increase in major bleeding (3.57% vs 2.67%, OR 1.34, 95% CI 0.70–2.58), and a significant increase in non-major bleeding (12.78% vs 3.65%, OR 4.12, 95% CI 2.37–7.17). Thrombolysis was associated with a significant reduction in recurrent pulmonary embolism or death in trials that enrolled both foreign subjects (3.46% vs 7.76%, OR 0.45, 95% CI 0.23–0.86) and Chinese subjects (0% vs 3.72%, OR 0.18, 95% CI 0.05–0.73). With regard to moderate pulmonary embolism, comparison of thrombolysis and anticoagulation showed a nonsignificant heterogeneity between the 2 trial groups (P = .12).
CONCLUSIONS: Both mortality and pulmonary embolism recurrence are decreased with thrombolysis compared with heparin treatment in patients with moderate pulmonary embolism. The risk of non-major bleeding is increased, but the risk of major bleeding is not.
Introduction
Pulmonary embolism is a life-threatening disease, with an estimated incidence of 6–7/10,000 people, and it is associated with a 3-month mortality rate of up to 17%.1,2 To date, the use of thrombolysis is recommend only in patients with massive pulmonary embolism. Moderate pulmonary embolism is a defined subgroup of pulmonary embolism, in which patients have hemodynamic stability but with right ventricular enlargement or hypokinesia or elevation of biomarkers of right ventricular injury. The initial treatment of moderate pulmonary embolism with thrombolytic therapy or anticoagulation has been under dispute for > 3 decades. The principal contradiction comes from different risk benefit ratios of treatment with thrombolytic therapy or anticoagulant therapy in randomized controlled trials (RCTs). The interpretation of meta-analyses3–6 showed that thrombolytic therapy in patients with moderate pulmonary embolism does not reduce mortality or recurrence rate. However, these previous meta-analyses included a few RCTs that were small sample studies and appear to be of limited value in guiding clinical treatment. The recently published RCTs showed reduction in recurrent pulmonary embolism or death with thrombolysis compared with anticoagulant therapy. To investigate the benefits of thrombolysis in moderate pulmonary embolism, we performed an updated meta-analysis of RCTs comparing thrombolysis and anticoagulation in subjects with moderate pulmonary embolism.
QUICK LOOK
Current knowledge
In patients with moderate pulmonary embolism, conflicting conclusions have been reached regarding the risk-benefit ratio of thrombolytic therapy to anticoagulant therapy in randomized trials and meta-analyses.
What this paper contributes to our knowledge
Compared with heparin, both mortality and pulmonary embolism recurrence are decreased by thrombolysis in patients with moderate pulmonary embolism. The risk of non-major bleeding increases, but the risk of major bleeding does not increase.
Methods
Study Identification
We attempted to identify all relevant published RCTs comparing thrombolytic therapy and anticoagulant therapy for the initial treatment of moderate pulmonary embolism. We searched the MEDLINE and Embase databases from January 1980 to June 2013 and the Cochrane Library, Wanfang, and CNKI databases from January 1990 to June 2013 using the terms pulmonary embolism, thromboembolism, thrombolysis, fibrinolysis, recombinant tissue plasminogen activator, rt-PA, alteplase, randomized controlled trial, controlled clinical trial, and humans. We also searched references cited in journal articles.
Study Selection
Two investigators (Hong Chen MD and CR) independently evaluated studies for inclusion, and any disagreement was resolved by discussion. The criteria for inclusion were (1) proper randomization, (2) objectively diagnosed hemodynamically stable acute pulmonary embolism, (3) comparison of thrombolytic therapy and anticoagulant therapy for the initial treatment of pulmonary embolism, and (4) outcomes including death, pulmonary embolism recurrence, and bleeding. The criteria for exclusion were (1) < 18 y of age, (2) pregnancy or lactation, and (3) objectively diagnosed massive acute pulmonary embolism.
Data Extraction
Two investigators (Hong Chen MD and CR) independently extracted data on the study design and quality and on the efficacy and safety outcomes during hospitalization or follow-up. In the event of discrepancy in the results obtained by the investigators concerning data extraction, the third investigator (Hong Chen MD PhD) helped in the final decision. Outcomes included (1) hemodynamically stable acute pulmonary embolism, (2) death, (3) pulmonary embolism recurrence, (4) major bleeding, (5) non-major bleeding, and (6) intracranial hemorrhage.
Assessment of Study Quality
We adopted the criteria for study quality outlined in the Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 (http://www.cochrane.org/handbook, accessed August 13, 2014) in the evaluation of studies included in the present meta-analysis. These criteria include (1) proper random sequence generation, (2) proper concealment of the allocation sequence, (3) blinding of the patient and the investigator assessing clinical outcomes to treatment allocation, and (4) completeness of follow-up. Two investigators (Hong Chen MD and CR) independently evaluated study quality, and any disagreements were resolved by discussion.
Outcomes
The primary efficacy outcome was a composite of recurrent pulmonary embolism or death. Secondary outcomes were the individual components of the primary outcome, and safety outcomes were major bleeding, non-major bleeding, and intracranial hemorrhage.
Statistical Analysis
We used a meta-analysis of all randomized trials comparing thrombolytic therapy and anticoagulant therapy in subjects with moderate pulmonary embolism by curative effect and safety index. Relative risks were combined using the Cochrane RevMan 5.2 software. We assessed the heterogeneity between studies with the Cochran Q test and took P < .05 as the threshold of statistical significance for heterogeneity and for calculating the effect of the odds ratio (OR) and 95% CI. After clarifying the study effect of heterogeneity, we used a fixed-effects model based on the Mantel-Haenszel method5 for combining results from the individual trials. Potential publication bias was evaluated using the funnel plot approach.
Results
Studies Included
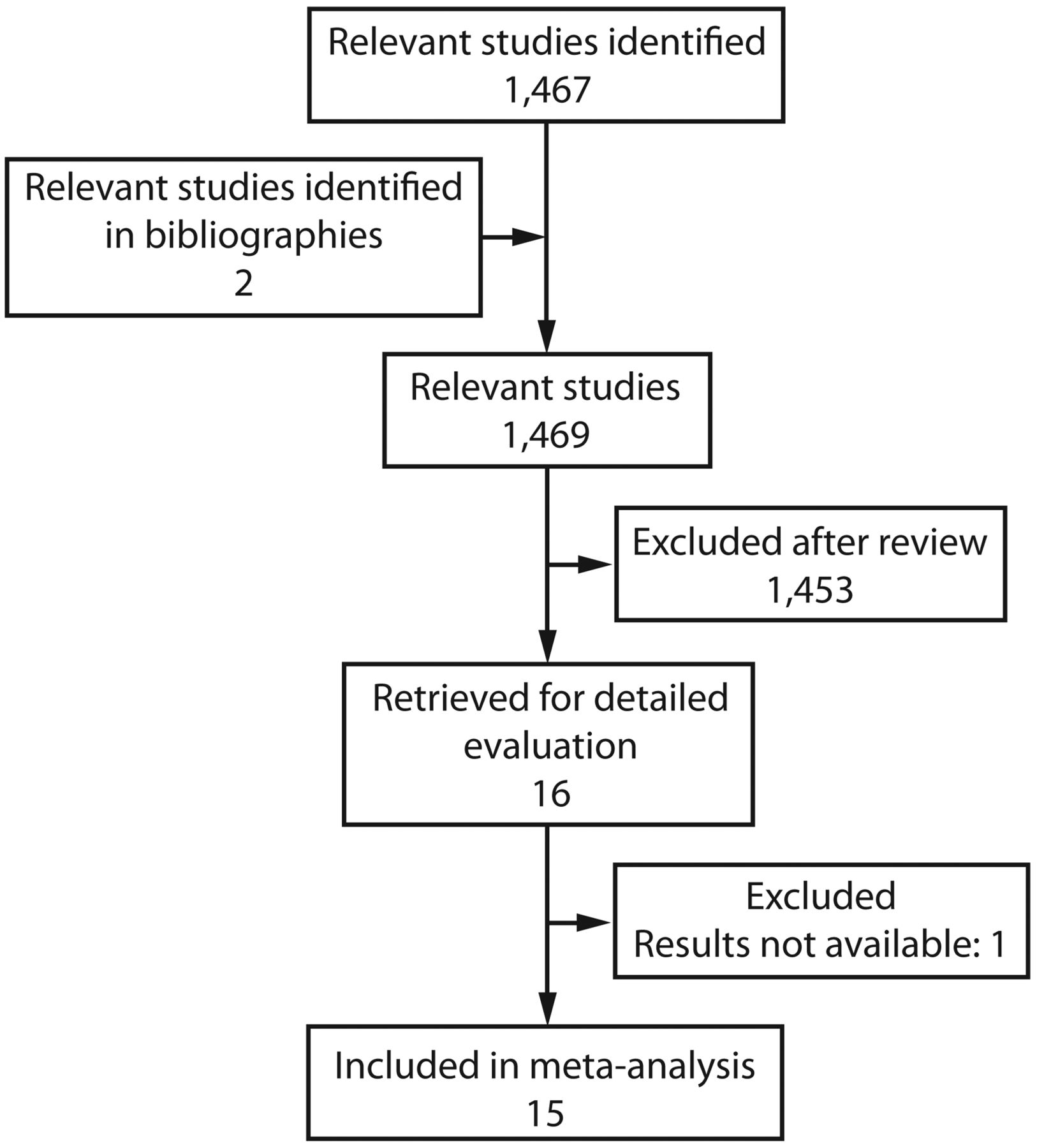
Figure 1 shows the study selection process. Sixteen RCTs comparing thrombolysis and anticoagulant therapy for subjects with moderate pulmonary embolism were identified. Nine of the 16 trials were published in a foreign language and enrolled ∼1,708 subjects7–15: one of them was excluded from this analysis because it was only a design and its results had not yet been published,15 and the other 8 trials involved 708 subjects (347 subjects treated with thrombolysis and 361 subjects treated with heparin). Seven of the 16 trials were Chinese documents involving 539 subjects with moderate pulmonary embolism16–22: 270 subjects treated with thrombolysis and 269 subjects treated with anticoagulant therapy. The designs of the studies included in the meta-analysis are summarized in Table 1.

Study flow chart.
Design of Studies Included in the Meta-Analysis
Study Quality
Table 2 shows the methodological quality of randomized studies of thrombolysis for moderate pulmonary embolism. Randomized treatment allocation sequences were generated with random number tables or programs in 5 studies.11–14,20, Information about proper concealment of the treatment allocation was provided in one trial.10 Both subjects and investigators were blinded to treatment allocation in 5 trials.7,8,11–13 The number of subjects lost to follow-up was reported in 3 of the 15 trials.14,16,22
Methodological Quality of Randomized Studies of Thrombolysis in Pulmonary Embolism
Efficacy Outcomes
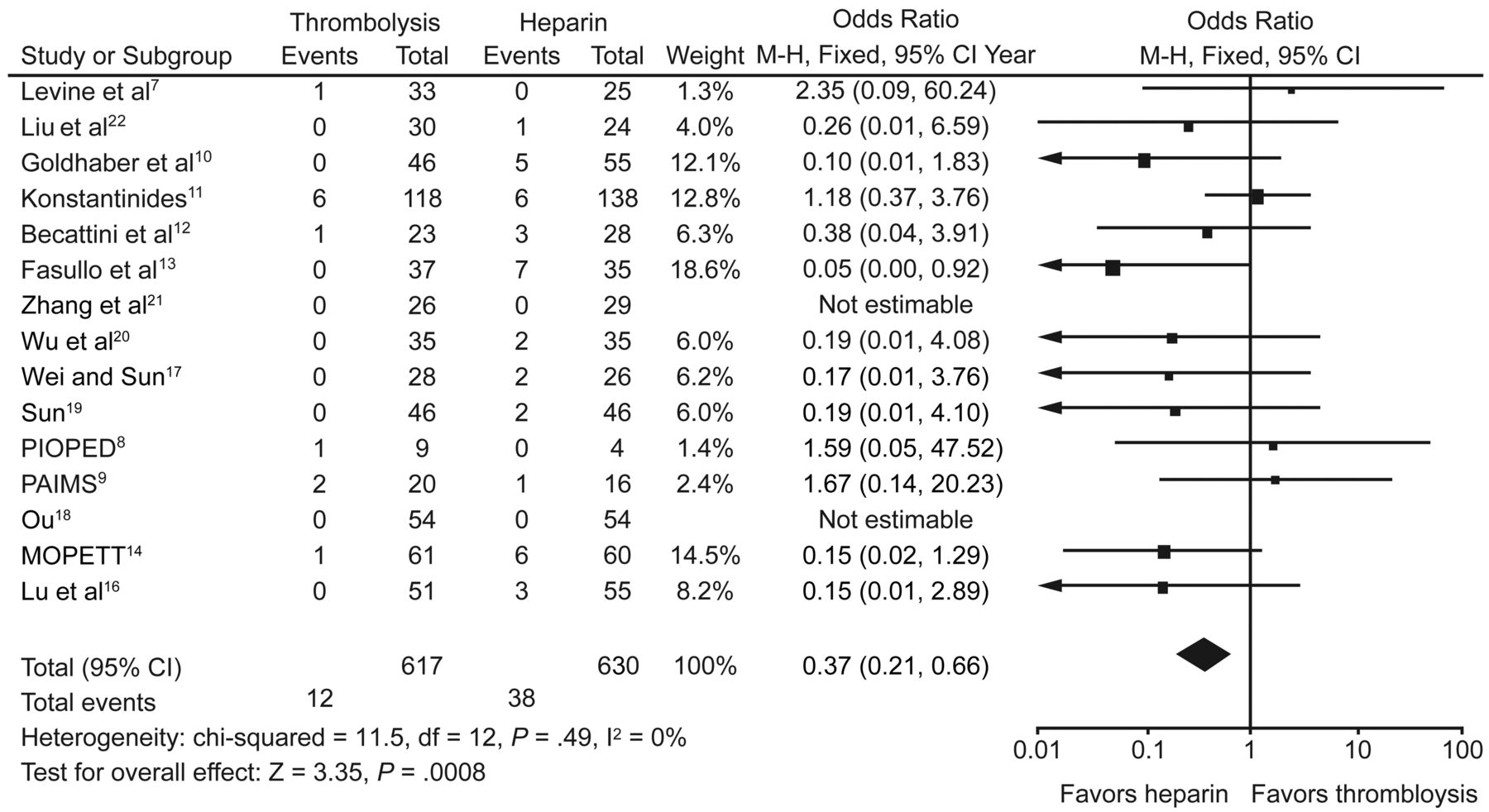
Data on the primary outcome of recurrent pulmonary embolism or death are presented in Figure 2, and individual components of this outcome are presented in Table 3. Nine of the 15 studies showed a reduction in recurrent pulmonary embolism or death with thrombolysis compared with anticoagulant therapy.10,12–14,16,18–20,22 The pooled estimate from all of the trials revealed a statistically significant reduction in recurrent pulmonary embolism or death (1.94% vs 5.87%, OR 0.37, 95% CI 0.21–0.66), with no statistical evidence of heterogeneity among the studies (P = .49). Similar estimates of treatment effect were obtained for death (1.46% vs 3.81%, OR 0.45, 95% CI 0.23–0.86) and recurrent pulmonary embolism (0.81% vs 3.65%, OR 0.32, 95% CI 0.14–0.70).
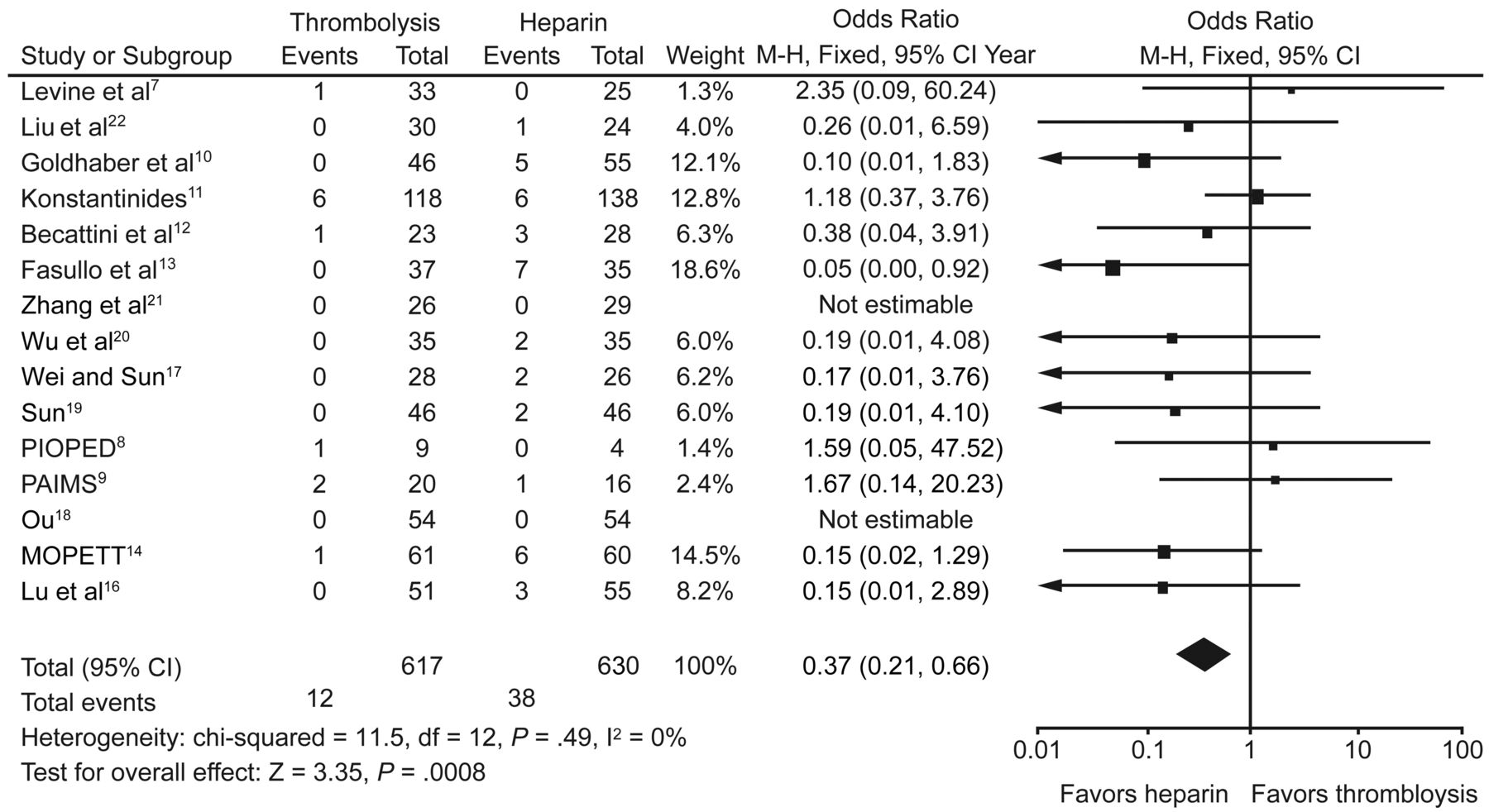
The primary outcome of recurrent pulmonary embolism or death for thrombolysis versus anticoagulant therapy for the initial treatment of moderate pulmonary embolism. PIOPED = Prospective Investigation of Pulmonary Embolism Diagnosis; PAIMS = Plasminogen Activator Italian Multicenter Study; MOPETT = Moderate Pulmonary Embolism Treated with Thrombolysis.
Data on Primary Outcome of Recurrent Pulmonary Embolism or Death
Safety Outcomes
Pooled data for safety outcomes are presented in Table 4. Eight of the 15 randomized trials suggested an increase in major bleeding for thrombolytic therapy compared with anticoagulant therapy.8–10,12,13,16,21,22 Nine of the randomized trials showed an increase in non-major bleeding with thrombolysis compared with heparin treatment.7,9,12,13,17,19–21,22 The pooled data revealed a nonstatistically significant increase in major bleeding (3.57% vs 2.67%, OR 1.34, 95% CI 0.70–2.58) but a statistically significant increase in non-major bleeding (12.78% vs 3.65%, OR 4.12, 95% CI 2.37–7.17).
Pooled Data for Safety Outcomes of Thrombolysis Versus Heparin Treatment
Subgroup Analyses
Table 5 provides a subgroup analysis comparing foreign and Chinese subjects. Compared with heparin treatment, thrombolytic therapy was associated with a significant reduction in recurrent pulmonary embolism or death in the 8 studies with 708 foreign subjects with moderate pulmonary embolism (3.46% vs 7.76%, OR 0.45, 95% CI 0.23–0.86) and in the 7 trials with 539 Chinese subjects (0% vs 3.72%, OR 0.18, 95% CI 0.05–0.73), with no statistical evidence of heterogeneity (P = .12). Similar estimates of treatment safety were obtained for major bleeding in foreign subjects (3.46% vs 2.77%, OR 1.19, 95% CI 0.51–2.79) and Chinese subjects (3.70% vs 2.23%, OR 1.59, 95% CI 0.57–4.45), with no statistical evidence of heterogeneity (P = .67).
Subgroup Analysis of Foreign and Chinese Subjects
Sensitive Analyses
Deletion of individual trials did not significantly change the primary outcome. Because this meta-analysis included randomized trials with small samples, most of scatter distributed at the bottom of the funnel plot (Fig. 3). The funnel plot of effect size versus study precision was comparatively symmetrical, with a similar number of studies on either side of the summary treatment effect for recurrent pulmonary embolism or death. This is consistent with a lack of major publication bias.

Funnel plot of effect size versus study precision of recurrent pulmonary embolism or death. OR = odds ratio.
Discussion
This meta-analysis of currently available RCTs showed some statistically significant benefits from thrombolytic therapy compared with anticoagulant therapy for the initial treatment of patients with moderate pulmonary embolism. Thrombolysis can reduce mortality or recurrence rate in patients with moderate pulmonary embolism. Compared with anticoagulation, thrombolytic therapy was associated with a significant reduction in recurrent pulmonary embolism or death in trials that also enrolled both foreign subjects with moderate pulmonary embolism and Chinese subjects. Nine studies10,12–14,16,18–20,22 showed a lower mortality or recurrence rate with thrombolysis compared with anticoagulation for the initial treatment of moderate pulmonary embolism. Compared with anticoagulation, thrombolytic therapy was associated with a significant increase in non-major bleeding but a nonsignificant increase in major bleeding.
Compared with previous meta-analyses, this study has provided conflicting conclusions about the benefits of thrombolysis in patients with moderate pulmonary embolism. A recent meta-analysis,6 which included only 5 randomized trials7–11 and involved 464 subjects, reported no significantly decreased mortality or recurrent pulmonary embolism, whereas we showed a significant benefit of thrombolysis compared with anticoagulation for the initial treatment of moderate pulmonary embolism. Our study included 15 trials involving 1,247 subjects and could lead to more valid results for the initial treatment of moderate pulmonary embolism. The subgroup analysis, which included 8 foreign studies involving 708 subjects, also showed that thrombolysis resulted in a significant reduction in pulmonary embolism recurrence or death compared with heparin treatment. The Pulmonary Embolism Thrombolysis (PEITHO) trial15 is a prospective, multi-center, international, randomized, double-blind comparison of tenecteplase versus placebo in subjects with moderate pulmonary embolism and is expected to enroll ∼1,000 subjects, to determine the benefits versus risks of thrombolysis in moderate pulmonary embolism, and to answer a query on the management of this patient population; the authenticity of the result of this meta-analysis can be further defined. Geibel et al23 pointed out that women with submassive pulmonary embolism might benefit less from thrombolytic treatment in terms of survival and pulmonary embolism recurrence and that they could be exposed to a higher bleeding risk compared with men. Compared with previous meta-analyses, this meta-analysis included more randomized trials, and the number of men compared with women in the Chinese studies included was larger. Perhaps the greater reduction in mortality and pulmonary embolism recurrence with thrombolysis was due to the larger number of male subjects. However, the ratio of male to female subjects in the foreign studies was close to 1:1, which supports the conclusion of this meta-analysis that thrombolytic therapy can reduce mortality and pulmonary embolism recurrence rate. Because the study by Geibel et al23 is not an RCT, it is necessary to use large RCTs to determine whether there are differences between males and females regarding the benefits and risks of thrombolytic therapy for moderate pulmonary embolism.
We conclude that thrombolysis can improve clinical outcome and is worth putting into clinical practice. Because the total hemorrhage rate of thrombolysis was 2 times that of anticoagulant therapy in subjects with moderate pulmonary embolism, the clinical application of thrombolytic therapy is still limited. Based on the conditions and weights of patients, reducing the dose of thrombolytic drugs can decrease the risk of major bleeding8,14; thus, we look forward to more clinical studies to determine the safe dose of thrombolysis for moderate pulmonary embolism. Of course, because of deterioration during anticoagulant therapy, upgraded treatment such as thrombolysis was selected, which can improve symptoms quickly, reduce pulmonary artery pressure, and improve right ventricle dysfunction.11,17 In addition, thrombolysis does cause a decline in the event-free survival rate after a 1-y follow-up compared with anticoagulation.16 The efficacy of thrombolysis could be confirmed by expanding the limited follow-up time.
This study has several potential limitations. First, in every study included, the number of subjects and the number of outcome events are low, so this meta-analysis has a limited statistical power. However, compared with previous meta-analyses, ours included more studies. Second, our meta-analysis included 7 Chinese studies. Although they clarified the consistent research group and control group at baseline, most of the literature did not show random distribution. Due to ethnic differences, we performed a subgroup analysis of foreign and Chinese subjects. Finally, the trials did not limit follow-up time. However, this does not preclude pooling of the results because it is only within the same studies that subjects are directly compared with each other. Because the trials that were included in this meta-analysis did not limit the type or dosage of thrombolytic drugs, this may be the major bias in this analysis. However, one previous meta-analysis24 concluded that different thrombolytic drugs share similar efficacy and safety.
Conclusions
Both mortality and pulmonary embolism recurrence are decreased by thrombolysis compared with heparin treatment in patients with moderate pulmonary embolism. Thrombolysis is worth putting into clinical practice. However, this study and the previous meta-analyses have reached conflicting conclusions regarding the efficacy of thrombolysis. Compared with heparin treatment, thrombolytic therapy increases the risk of non-major bleeding, but not major bleeding. Further evaluation of the efficacy and safety of thrombolysis for the treatment of moderate pulmonary embolism appears to be warranted.
Acknowledgements
We thank Zhenguo Zhai MD PhD for editing.
Footnotes
- Correspondence: Hong Chen MD PhD, Department of Respiratory Medicine, First Affiliated Hospital of Chongqing Medical University, No. 1, Yixue Road, Yuzhong District, Chongqing 400016, China. E-mail: hopehong2003{at}126.com.
This study was supported by the China Key Research Projects of the 12th National Five-Year Development Plan (2011BAI11BOO). The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}