

Abstract
BACKGROUND: CPAP is currently the treatment of choice for obstructive sleep apnea syndrome, but therapy adherence is poor. Many educational trials have been proposed to increase CPAP adherence. We tested the hypothesis that polysomnograph chart viewing by patients would improve CPAP adherence.
METHODS: A controlled parallel group study was performed with 206 newly diagnosed obstructive sleep apnea syndrome patients, randomized into 2 groups (n = 103 each): standard support group, and educational support group. Each educational support group subject viewed 2 consecutive polysomnograms on the computer screen: the first recorded during a standard diagnostic overnight polysomnography, and the second during a full-night polysomnography with nasal CPAP. The subject's attention was drawn only to the flow and oxyhemoglobin saturation curves. Clinical outcomes were assessed via polysomnography at CPAP initiation and after 1, 3, and 12 months.
RESULTS: After 12 months of CPAP, 76% of the educational support group and 52% of the standard support group returned for a follow-up visit (P < .001). Statistical significance had already been reached after 1 and 3 months. Moreover, CPAP use (measured as hours of use per night) was higher in the educational support group at each control visit.
CONCLUSIONS: Polysomnograph chart viewing by obstructive sleep apnea patients can increase CPAP adherence, as evaluated by rate of return for the follow-up visit and mean nightly CPAP use.
Introduction
Obstructive sleep apnea (OSA) is characterized by recurrent episodes of upper-airway obstruction during sleep, resulting in chronic intermittent hypoxia, sleep fragmentation, and daytime sleepiness.1 OSA is present in as many as 2% of females and 4% of males in the general population,2 and is burdened with substantial associated morbidity and mortality.3 CPAP is the primary treatment for OSA syndrome,4 and normalizes sleep architecture, reduces daytime sleepiness, improves daily function, decreases the risk of automobile accidents, improves quality of life,5 and decreases blood pressure and other cardiovascular events.6 Unfortunately, the data in the literature regarding CPAP adherence are not so encouraging.7,8 Current evidence suggests that only 61–69% of those prescribed CPAP adhere to it.9 Several studies tried to determine the percentage of patients who adhere to CPAP, and the estimated range is 46–80%.7,9–14 Perhaps many people mistakenly believe that CPAP use will cure their sleep breathing disorder, at which time they can discontinue CPAP.15 Moreover, some patients do not consider OSA as a serious health problem,16 and have a poor perception of OSA's risks.17
Many studies have found that patients' perceptions of the benefits and health value of CPAP are related to better adherence.18,19 Education20,21 and intensive support strategies22 improve long-term CPAP adherence. Given that the patient's awareness of the disease plays a decisive role in CPAP adherence, we tested the hypothesis that having the patients view the polysomnograph (PSG) chart would improve CPAP adherence.
QUICK LOOK
Current knowledge
CPAP is commonly used for the treatment of obstructive sleep apnea, but adherence to CPAP is poor because of discomfort and cumbersome application. Education programs to improve adherence have had varying results.
What this paper contributes to our knowledge
Patients who, with a clinician's guidance, reviewed their polysomnography SpO2 and flow curves were more likely to return for their follow-up appointments and had better CPAP adherence at 12 months.
Methods
This prospective, randomized, single-blind, controlled, parallel group study was approved by the institutional review board of Bari University General Hospital, Bari, Italy, and carried out in accordance with the principles of the Helsinki Declaration. All subjects gave written informed consent prior to participation in the study.
Subjects
We enrolled 206 adult subjects (≥ 19 y old) with newly diagnosed OSA (apnea-hypopnea index ≥ 15 events/h, with or without daytime symptoms). We excluded patients who had COPD or any global respiratory failure, central sleep apnea syndrome, previous diagnosis of congestive heart failure or cardiomyopathy, any chronic neurological disorder, or any severe mental or psychological impairment. All the subjects lived within 30 km of Bari. Randomization was via predetermined balanced blocks, generated by tossing a coin. The subjects were blinded to the group to which they were allocated.
Study Design
Subjects underwent standard diagnostic overnight PSG (E Series System, Compumedics, Victoria, Australia). The diagnosis night was followed directly by a second full-night PSG with nasal CPAP with manual titration.23 Then the subjects were randomly allocated to the standard support group (n = 103) or the educational support group (n = 103).
In the standard support group a sleep medicine physician gave each subject a full explanation of the need for and benefits of CPAP. This explanation required ≤ 10 min. Prior to CPAP titration the subjects received education from a nurse regarding operation of the CPAP machine and mask placement, and a 20-min period of auto-CPAP exposure during the afternoon, for CPAP acclimatization.
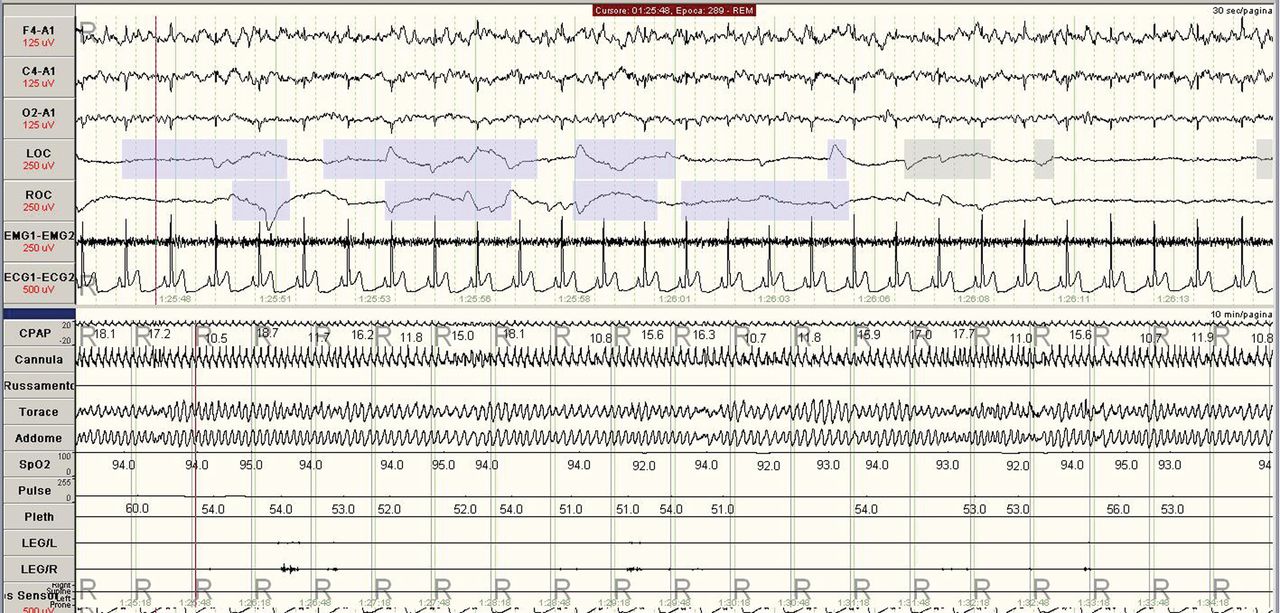
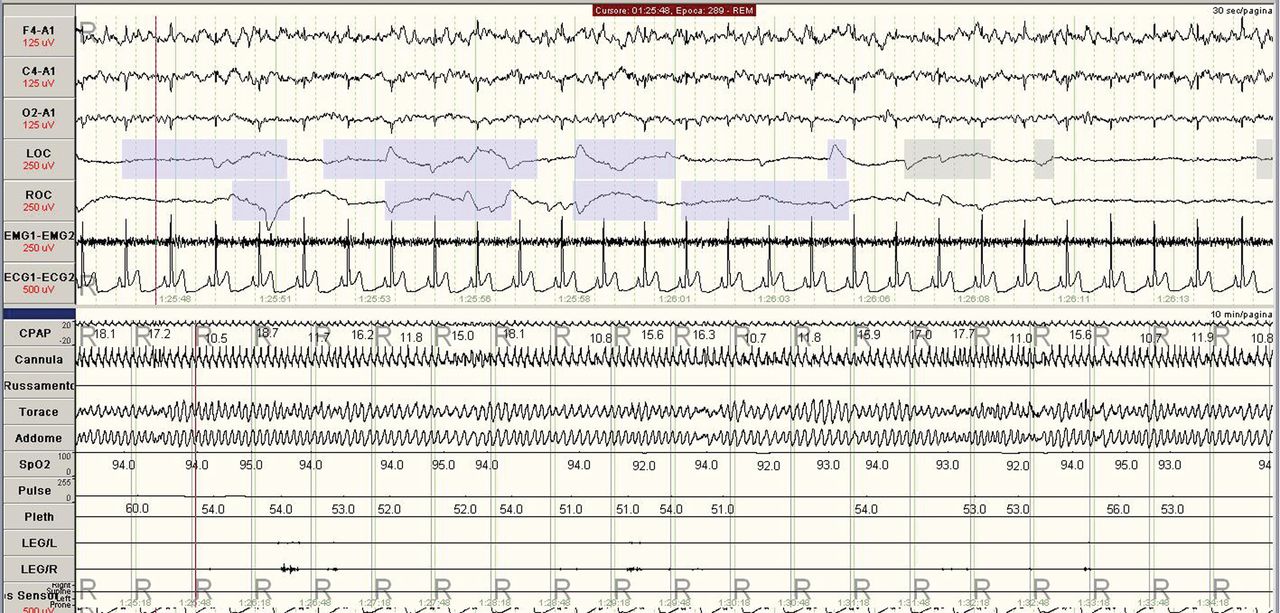
In the educational support group, as in the standard support group, all subjects received education about OSA and its risks. In addition, each educational support group subject viewed, simultaneously, on the computer screen, the first 10 min of the rapid-eye-movement phase of both the PSG charts: from the diagnosis PSG night (Fig. 1) and the CPAP titration PSG night (Fig. 2), and received explanations of the charts from a sleep medicine physician, to emphasize the PSG signs of apnea-hypopnea and the disappearance of those signs with CPAP. We drew the subject's attention only to the flow and oxyhemoglobin saturation curves. This standardized procedure, which took ≤ 5 min, was performed with all the educational support group subjects, by one of the 3 responsible sleep physicians in charge.

Example polysomnography chart of 10 min of the rapid-eye-movement phase during the obstructive sleep apnea diagnosis night.
Example polysomnography chart of 10 min of the rapid-eye-movement phase during the CPAP titration night.
In both groups, 3 follow-up visits were performed, at 1, 3, and 12 months after CPAP initiation. At diagnosis and at each follow-up we measured the Epworth Sleepiness Scale score.24 At each follow-up visit we calculated the retention rate (calculated as the number of subjects who returned for follow-up divided by the total number of subjects) and downloaded the CPAP use data from the CPAP device. Any problems with CPAP treatment were addressed, and the CPAP data were reviewed with the subject, without emphasizing the achievements. Subjects who did not return for a follow-up visit were considered non-adherent and dropped-out the study, so the Epworth Sleepiness Scale scores and CPAP use data in the Results section are only for the adherent CPAP users.
Statistical Analysis
The analyses were on an intention-to-treat basis. Data are presented as mean ± SD unless otherwise indicated. Differences between the groups were analyzed with the Student t test for independent samples for normally distributed variables, or the Mann-Whitney U test for non-normally distributed variables. The chi-square test was used to compare proportions between groups. P < .05 was considered significant.
Results
Figure 3 shows the study flow chart. The Table shows the cohort's baseline characteristics. There were no significant baseline differences between the 2 groups. Body mass index and neck and waist circumference did not change significantly during the study. During the CPAP PSG night the apnea-hypopnea index, oxygen desaturation index, and total sleep time with oxyhemoglobin saturation below 90% improved significantly in both groups and to a similar degree (data not shown).

Flow chart. OSA = obstructive sleep apnea.
Subject Characteristics at Baseline
Retention Rate
After 1 month of CPAP, 93% of the educational support group subjects and 78% of the standard support group subjects returned for follow-up (chi-square = 9.98, P = .002). At 3 months, 87% of the educational support group subjects came to the follow-up appointment, versus 69% of the standard support group subjects (chi-square = 10.26, P = .002). At 12 months, 77% of the educational support group came to the follow-up appointment, versus 52% of the standard support group subjects (chi-square = 13.26, P < .001) (Fig. 4).

Retention at follow-up visits at 1, 3, and 12 months.
CPAP Use
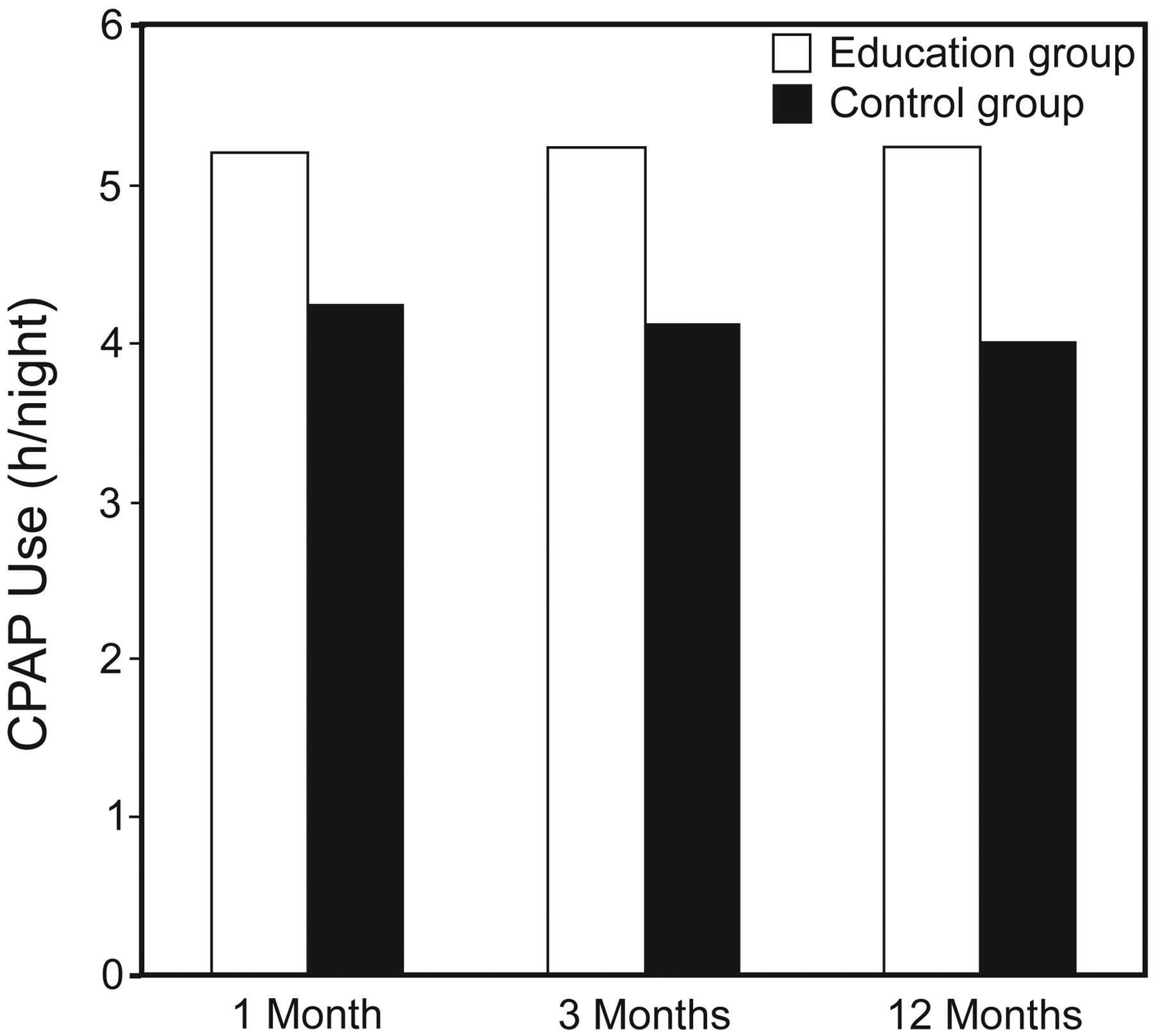
At 1 month the educational support group had higher mean CPAP use: 5.20 ± 1.29 h/night vs 4.24 ± 0.76 h/night (P = .008). At 3 and 12 months the significant differences in CPAP use between the 2 groups persisted: 5.25 ± 0.91 h/night versus 4.12 ± 0.57 h/night (P = .007), and 5.24 ± 0.85 h/night versus 4.02 ± 0.37 h/night (P = .005), respectively (Fig. 5).

Mean hours of nightly CPAP use at 1, 3, and 12 months.
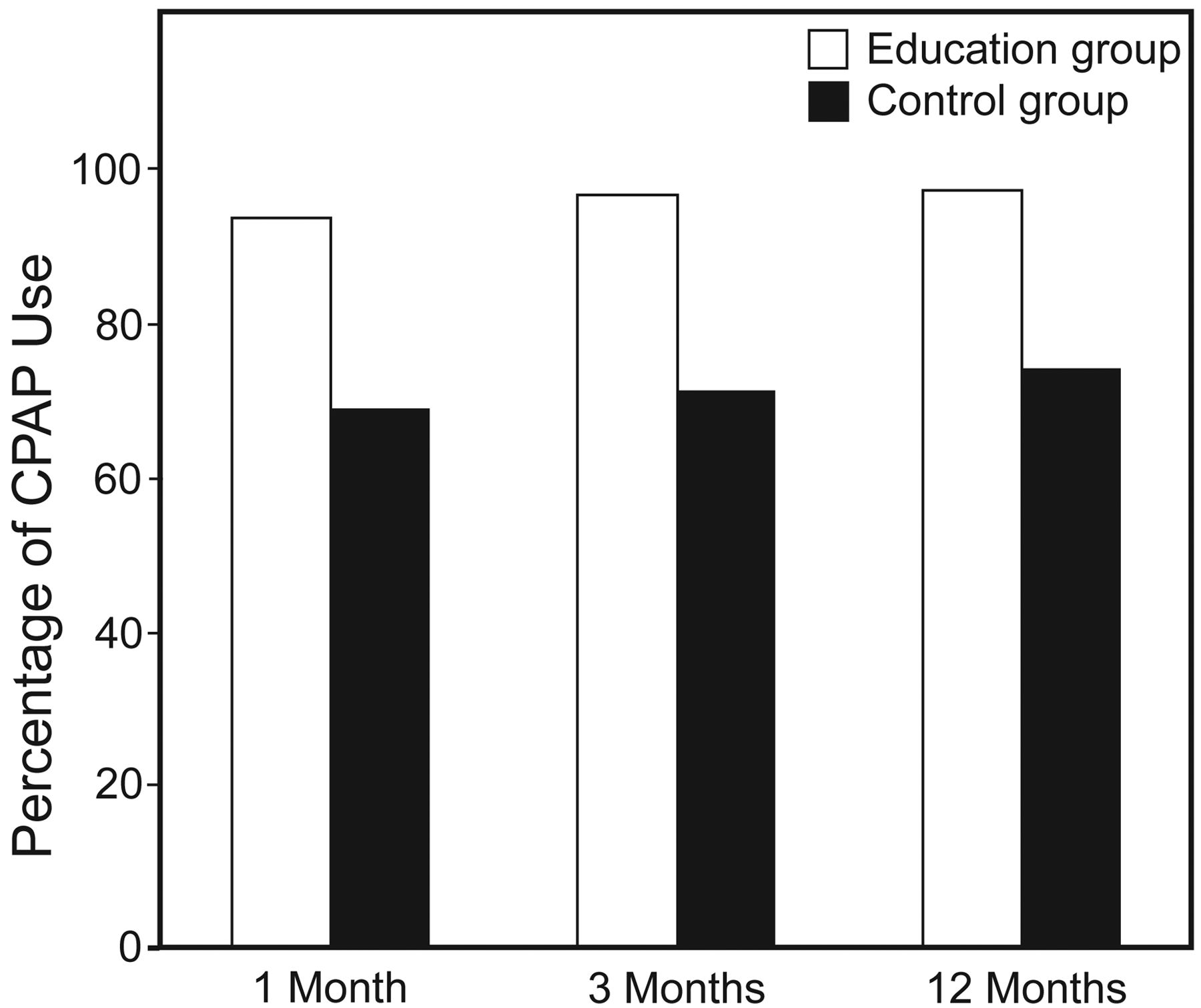
At 1 month, 94% of the educational support group and 69% of the standard support group had used their CPAP > 4 h/night for > 70% of all the nights (chi-square = 13.06, P < .001). At 3 and 12 months that significant difference persisted: 97% versus 71% (chi-square = 14.79, P < .001), and 97% versus 74% (chi-square = 12.66, P < .001), respectively (Fig. 6).
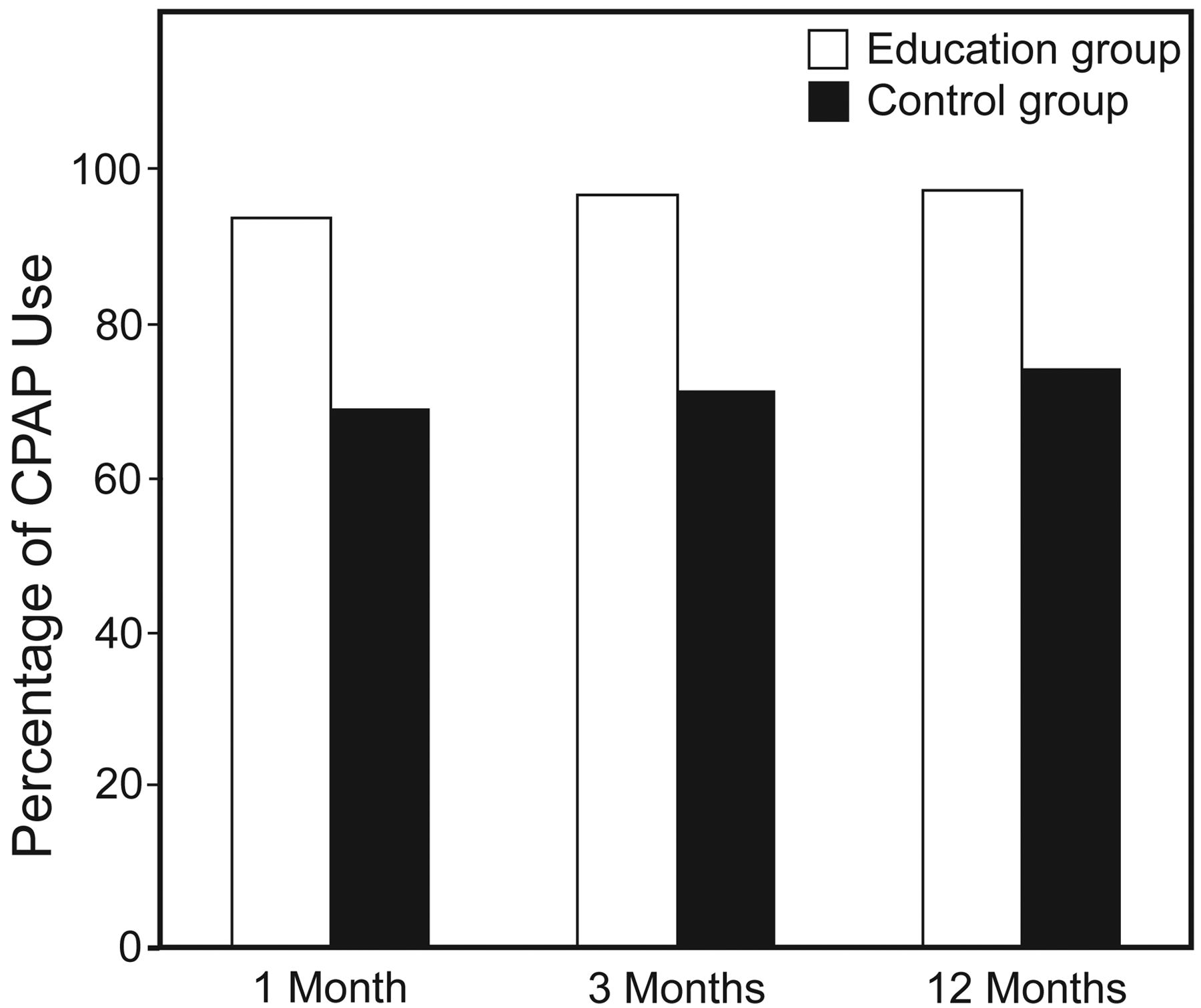
Percentages of subjects who used their CPAP machines for > 4 h/night for > 70% of all the nights, at 1, 3, and 12 months.
The mean Epworth Sleepiness Scale score was significantly and similarly reduced at 1 month in both groups: 4.37 ± 0.30 in the standard support group, and 4.30 ± 0.20 in the educational support group. At 3 and 12 months the mean Epworth Sleepiness Scale score remained substantially stable, and there were no significant differences between the groups: at 3 months 4.04 ± 0.23 vs 4.14 ± 0.31, at 12 months 3.30 ± 0.28 vs 3.10 ± 0.35.
Discussion
Our most important finding is that a significantly higher percentage of educational support group subjects returned for follow-up at 1, 3, and 12 months. This higher retention rate suggests that knowledge and awareness of OSA and its risks may be a key aspect of CPAP adherence. Some previous studies demonstrated the importance of education in CPAP adherence,21,22,25–27 but to our knowledge this is the first long-term study in which subjects viewed their own PSG charts with and without CPAP. Ninety-three percent of the subjects who viewed their PSG charts returned for follow-up at 1 month, and 76% returned at 12 months. There are 2 possible explanations for the difference in retention. First, viewing the PSG chart is certainly of paramount importance in realizing the pathophysiological changes and importance of OSA; indeed, even a more detailed explanation of OSA and/or CPAP cannot disregard the visual experience of the classic PSG signs of apnea/hypopnea, and their disappearance with CPAP. Second, it is conceivable that viewing the PSG charts has an important psychological impact, increasing the patient's awareness of their condition and therefore their motivation to adhere to CPAP. In support of this, in the recent study by Nadeem et al28 the subjects who viewed only the pathological PSG chart (without viewing the with-CPAP PSG chart that showed the resolution of the OSA events) did not improve CPAP adherence, compared to the control arm.
At every follow-up visit we observed higher CPAP use in the educational support group: mean 5 h/night versus 4 h/night. On the other hand, although a standard criteria to define the optimal nightly duration of CPAP use has not been established,26,29 some authors consider 4 h/night for 70% of nights acceptable.7,23,29,30 Using that definition we found better adherence in the educational support group (see Fig. 6).
Several randomized controlled trials have found significant clinical improvement with even the relatively low levels of CPAP use we found in our standard support group.31,32 This was confirmed in our study since we observed that CPAP treatment reduced the Epworth Sleepiness Scale score in both groups to a similar extent.
Education studies regarding CPAP adherence have often included multiple simultaneous interventions (“packages”).18 In the study by Hoy et al22 the subjects in the educational support group received home nursing, a 3-night CPAP trial, and educational support. In the study by Damjanovic et al27 the intensive support included optimizing the equipment, such as the correct use of humidifiers and mask fit, together with counseling and educational support. However, in the present study the educational support was based on a single and brief intervention in order to assess its specific contribution to CPAP adherence, avoiding potential confounding factors.
Here some limitations need to be taken into account. First, the expression “retention rate” should be used with caution. In fact, the design of this study does not allow us to know whether all the subjects who did not return for follow-up were really non-adherent to CPAP. On the other hand, it is likely that subjects who do not return to clinic are not adherent, since several insurance companies require proof of periodic clinic attendance for coverage of CPAP machine rental, and non-adherent subjects lose the use of the machine.21 Retention rate has been considered a key indicator of CPAP adherence by various researchers as well.21,27,30 Finally, in our study, CPAP adherence was not reinforced during the follow-up visits, so as not influence the outcome.
Second, only reduced daytime sleepiness was considered as a clinical outcome, and it is possible that there were significant differences in other symptoms, quality of life, cognitive function, and apnea-hypopnea index. However, daytime sleepiness is considered a key factor in the clinical evaluation of OSA patients,33 and we considered the mean nightly CPAP use adequate in both groups. These considerations to some extent counterbalance this limitation.
This study did not include a cost–benefit analysis. However, this educational procedure does not entail any additional cost except for adding 5 min to the standard protocol. Hence, it may be easily reproduced in any sleep medicine center.
To overcome the potential limit of the patients' ability to interpret the PSG chart, we focused their attention only on the flow and oxyhemoglobin saturation curves.
The present study included only subjects with moderate to severe OSA, so our results cannot be applied to patients with mild OSA.
Conclusions
We have demonstrated that having the patient view the PSG charts from both the OSA diagnosis night and the CPAP titration night can improve CPAP adherence, as evaluated by follow-up-retention rate and mean nightly CPAP use.
Footnotes
- Correspondence: Vito Antonio Falcone MD, Policlinico - Pneumologia, Università Degli Studi di Bari Aldo Moro, Piazzale Giulio Cesare 1, Bari 70124 Italy. E-mail: va.falcone13{at}gmail.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}