

Abstract
BACKGROUND: Exercise training improves both exercise tolerance and quality of life in patients with COPD. The intensity of exercise training is crucial to achieve a true physiologic effect. However, in COPD patients, exertional dyspnea and leg fatigue mean that the patient cannot maintain intensity of training for enough time to yield a physiologic training effect. The use of noninvasive ventilation (NIV) support has been proposed as an alternative strategy to improve exercise tolerance and respiratory and cardiovascular performances. The first aim of our meta-analysis was to evaluate exercise training with NIV in terms of physiologic effects after the completion of a pulmonary rehabilitation program. The second aim was to investigate the dose-response relationship between physical improvement and training intensity.
METHODS: Literature research was performed using MEDLINE, Embase, and CINAHL. Meta-analysis and meta-regressions were performed using random effects models.
RESULTS: Eight studies provided a proper description of a training schedule in stable COPD patients. A similar effect between NIV and placebo was observed for the outcomes considered despite differences between studies. However, subjects experienced a relevant and statistically significant improvement after rehabilitation for almost all of the outcomes considered. Heart rate (6 beats/min [95% CI 0.94–11.01], P = .02), work load (9.73 W [95% CI 3.78–15.67], P < .001), and oxygen consumption (242.11 mL/min [95% CI 154.93–329.9], P < .001) significantly improved after training. Improvements in heart rate and work load were significantly correlated to training intensity.
CONCLUSIONS: Given the small number of available studies, the small sample sizes, and the complete absence of power calculation, we think that this topic deserves a more in-depth investigation. Randomized clinical trials with larger sample sizes based on statistical power calculations and designed to investigate the effect of training duration and intensity on rehabilitation are needed to confirm results in this important field.
Introduction
Exercise training is a key component of pulmonary rehabilitation. It significantly improves both exercise tolerance and quality of life in patients with COPD.1–3 The intensity of exercise training is crucial to achieve a true physiologic effect. However, in patients with severe COPD, exertional dyspnea and leg fatigue mean that the patient cannot maintain intensity of training for enough time to yield a physiologic training effect.4 The use of noninvasive ventilation (NIV) support during training sessions has been proposed as an alternative strategy to improve exercise tolerance5–9 and respiratory and cardiovascular performances10,11 in patients with mild-to-severe COPD. Previous studies have suggested that the application of NIV delivered via different devices (CPAP device, Proportional Assisted Ventilation [PAV], pressure support ventilation [PSV]) during exercise in patients with COPD results in an immediate improvement in exertional dyspnea and exercise endurance.9 Few studies up to now have compared the effect of using NIV during a pulmonary rehabilitation program in COPD patients and in a control group. Bianchi et al12 and Hawkins et al13 used PAV in their studies. Bianchi et al12 did not observe any significant post-rehabilitation differences in exercise tolerance or cardiorespiratory response to an incremental test between an NIV group and a control group. Hawkins et al13 reported a significant increase in the maximal incremental cycle exercise and greater training intensities in the NIV group compared with controls but not in the constant work rate test. During the constant work rate test, there was no difference in the physiologic response in terms of exercise duration, heart rate, and lactate concentration between the groups. When considering studies using PSV, Costes et al14 observed a greater improvement in peak oxygen consumption (V̇O2) and reduced ventilatory requirements for maximal exercise in the NIV group compared with the control group. After training, the change in the work rate exercise duration and the isotime decrease in blood lactate were similar in both groups. A small but significant difference in the NIV group after 6 weeks of training in terms of walking endurance, maximal work load metabolic equivalents, and heart rate was observed by Johnson et al.15 Borghi-Silva et al16 showed that, at peak exercise in the incremental exercise test after 6 weeks of training, only the NIV group showed significant changes in walking speed, heart rate, carbon dioxide production and V̇O2 peak, and breathing frequency. Moreover, there was a significant reduction in the lactate/speed ratio only in the NIV group. In the study by Reuveny et al,17 8 weeks of training with NIV produced significant physiologic changes in terms of V̇O2 maximum, anaerobic threshold, tidal volume, minute ventilation, and oxygen pulse. No physiologic improvement was found in any of the cardiorespiratory parameters in the control group patients. The authors did not observe any change in the maximal work load in the incremental test performed after training in either group.
van 't Hul et al18 observed a statistically significant difference in favor of the group that trained with an inspiratory pressure of 10 cm H2O in terms of improvement in exercise tolerance (shuttle test), intensity of training, cycle endurance, and reduction in minute ventilation isotime. Toledo et al19 observed that, after 12 weeks of training, the group that trained with NIV had a significant improvement in heart rate, systolic blood pressure, and V̇O2 after training compared with the control group. A significant reduction in blood lactate was observed at identical levels of exercise in the NIV group compared with the control group.
For the moment, it is difficult to draw any firm conclusions about the potential physiologic effects of the use of NIV during exercise training for many reasons: small size of the studies, differences in the pathophysiologic characteristics of the enrolled patients, differences in the devices used, and outcome measures assessed. In this context, the first aim of our meta-analysis was to evaluate the effectiveness of supporting exercise training with NIV in terms of physiologic effects after the completion of a pulmonary rehabilitation program in patients with COPD. The second aim was to investigate the dose-response relationship between physical improvement and total training time in the NIV arm.
QUICK LOOK
Current knowledge
Exercise training improves exercise tolerance and quality of life in patients with COPD. Exercise tolerance is limited, however, by dynamic hyperinflation, which results in submaximal exercise. Noninvasive ventilation (NIV) has been proposed as a method to improve exercise tolerance.
What this paper contributes to our knowledge
The evidence supporting the use of NIV to improve exercise tolerance in COPD is based on small single-center studies that are underpowered. The current evidence cannot demonstrate the superiority of NIV to improve exercise tolerance. Randomized clinical trials with appropriate sample sizes should be designed to investigate the effect of training duration and intensity.
Methods
Data Source
Articles to be included in the study were identified through a search of electronic databases and by scanning reference lists of articles. This search was applied to MEDLINE, Embase, and CINAHL using “noninvasive ventilation,” “training exercise,” and “chronic obstructive pulmonary disease” as key words. In addition, we made a manual search of reference lists of included studies, reviews, meta-analyses, and guidelines on NIV and pulmonary disease.
Study Selection
The literature search was conducted independently and in duplicate by 2 investigators (MG and CR). The same authors independently selected potentially eligible studies for inclusion. Disagreements between reviewers were resolved by consensus; if no agreement could be reached, the opinion of a third senior author (FG) was requested, and his decision was considered final.
Data Extraction and Quality Assessment
Study papers were included if they: (1) provided comparative data investigating the effect of NIV and exercise training in stable COPD patients; (2) reported one or more of the following outcomes: lactate production, heart rate, walking or physical exercise performance, respiratory outcomes, and training characteristics (number of training sessions, training duration per session, and overall rehabilitation schedule); and (3) were published in English. Methodological quality was independently assessed by 2 investigators (MG and AS) using the Physiotherapy Evidence Database (PEDro) scale. This scale has 11 dichotomous items concerning the study design, statistical analysis, and intention to treat. The PEDro score was calculated by counting the number of checklist criteria that were satisfied in the trial report.
Data Synthesis and Analysis
We developed a data extraction sheet. This was pilot-tested on 3 randomly selected articles and modified accordingly. The following data were extracted from selected studies and entered into a data extraction form by one investigator (ST): author, study year, participants, country, outcomes, training schedule characteristics, and number of dropouts. A second investigator (CR) checked the extracted data to ensure accurate reporting. Disagreements were resolved by discussion between the 2 investigators; if no agreement could be reached, it was planned that a third investigator would make the final decision (AD). Baseline characteristics (age, gender, and FEV1) were compared by means of random effects comparison, and then the comparisons between NIV and placebo at isotime were reported. To account for ventilation setting, this analysis was also performed comparing results between PAV and PSV. Afterwards, we investigated variable modification at isotime after training in the NIV arm. A meta-analytical approach was used for both analyses. If the heterogeneity evaluated by I2 was > 50%, the random effects model described by DerSimonian and Laird20 was selected over the fixed effects model. The small study and publication bias effect was assessed by funnel plot visual inspection. Both Harbord and Egger21 tests were applied if at least 5 studies were included. Finally, to investigate to what extent training duration influenced changes in outcome in the NIV arm, a random effects meta-regression approach was used. The random effects meta-regression model used evaluated training duration as explanatory covariate. Study weight resulting from meta-analysis was used in the regression analysis as a weight variable. P = .05 was considered statistically significant, and all statistical tests were two-tailed. Funnel plots were obtained using RevMan 5 (The Cochrane Collaboration, Copenhagen, Denmark). Meta-analysis, meta-regressions, and Harbord and Egger asymmetry tests were performed using the SAS 9.2 software package (SAS Institute, Cary, North Carolina).
Results
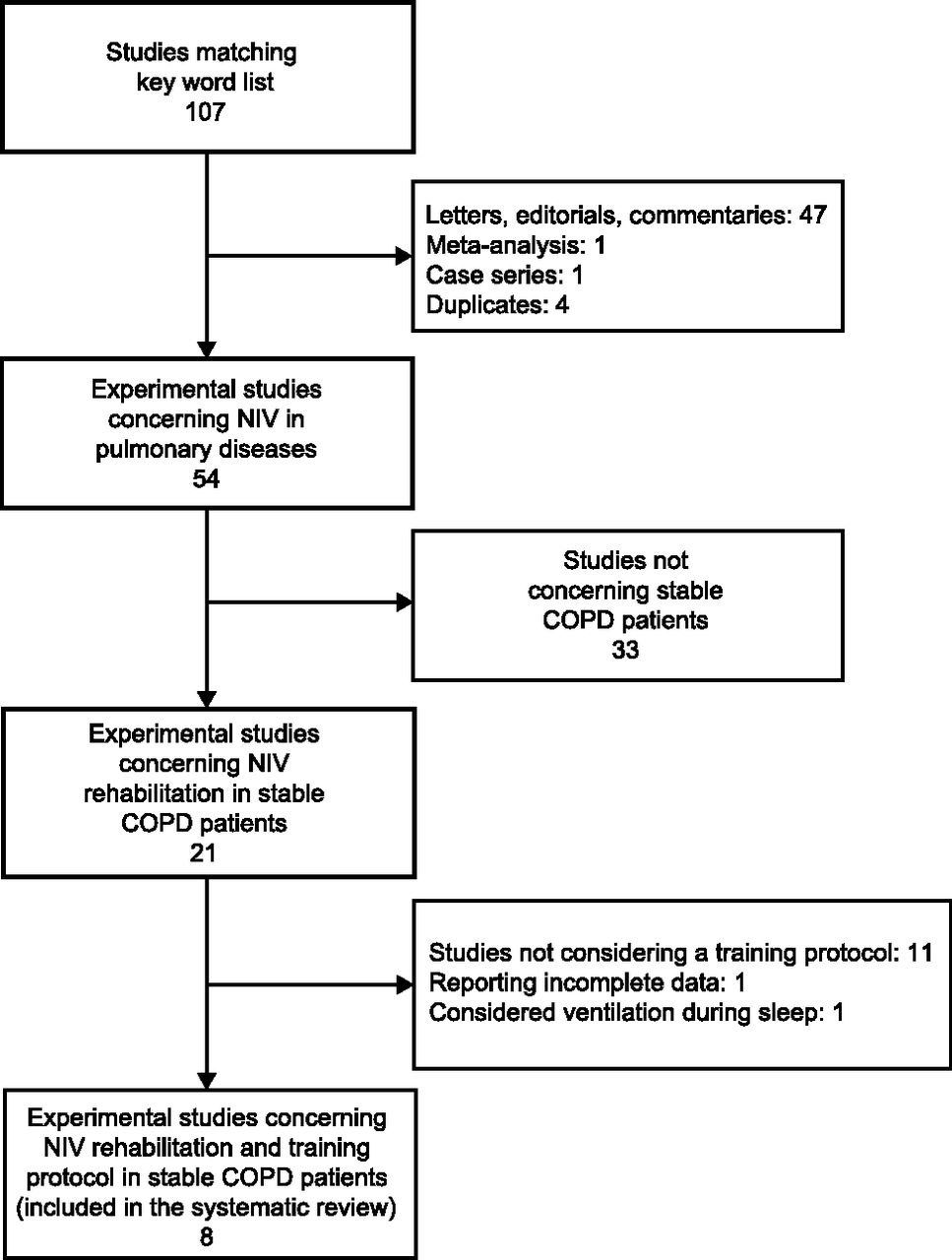
A total of 107 results were selected after examining titles and abstracts; of these, 53 were excluded because they were duplicates or were not designed as comparative studies. Of the 54 papers remaining, 33 were excluded because they did not concern stable COPD patients. Among the 21 papers remaining, only 8 used and properly described a physical training schedule. Figure 1 shows the flow chart of study selection. Tables 1 and 2 summarize study characteristics. Among the 8 studies considered, the United Kingdom and Brazil provided 2 studies each, whereas France, Italy, Israel, and The Netherlands provided one study each. All selected studies were controlled trials. The studies by Costes et al14 enrolled consecutive patients, whereas the others were randomized controlled trials. At the end of the training protocol, the sample size in each study varied between 7 and 15 patients, and the number of dropouts varied between zero and the 50% reported by Bianchi et al.12 Mean age was similar between studies, whereas FEV1 could be considered heterogeneous even if not statistically significant. Women were included in all of the studies considered except in that by Bianchi et al.12 When considering the study quality, we noticed that all studies obtained a satisfactory score on the PEDro scale and that the agreement between the 2 people evaluating this was satisfactory, being > 95%. The duration of training protocols was homogeneous, ranging from 6 to 8 weeks, whereas session duration could be considered heterogeneous, ranging from 20 to 60 min. Training exercises consisted of treadmill training, endurance walking, or cycling using a cycle ergometer. Finally, ventilation protocols in the NIV arm followed different approaches. Funnel plot visual inspection and Harbord and Egger asymmetry test results did not exclude the hypothesis of a small study or publication bias effect.
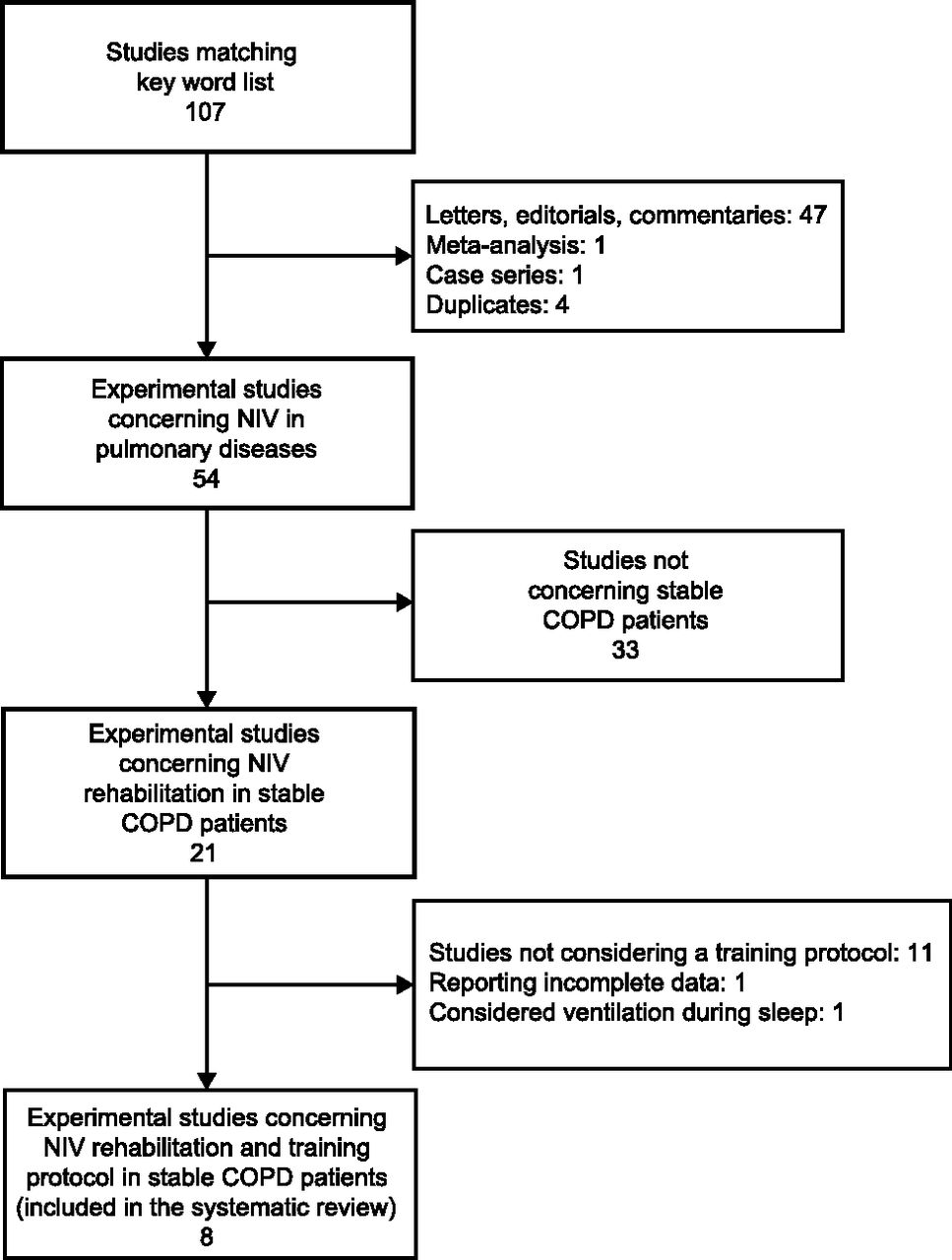
Flow of study selection. NIV = noninvasive ventilation.
General Characteristics of Examined Studies
Comparisons Groups and Ventilation Technical Details
NIV Versus Placebo
When considering the comparison between NIV and placebo, some slight and not statistically significant differences between groups were found. In particular, when looking at the heart rate as an outcome, we noticed that Costes et al14 and Toledo et al19 observed a similar difference between NIV and placebo, showing a slightly better outcome in the NIV group (a reduction of 5.0 [95% CI −16 to 25] and 5.8 beats/min, respectively). This effect was not confirmed in the study by Hawkins et al13 regarding work load and lactate as outcome variables, so firm conclusions could not be drawn. On the other hand and as expected, the difference in V̇O2 as outcome is clearer (167 [95% CI −15 to 350], P = .07) even if this was not statistically significant. Two studies (Bianchi et al12 and Hawkins et al13) used PAV, whereas other studies employed PSV. Sub-analysis considering stratification by ventilation protocol did not result in any statistically significant difference from the pooled analysis.
Post-Training Evaluation in the NIV Arms
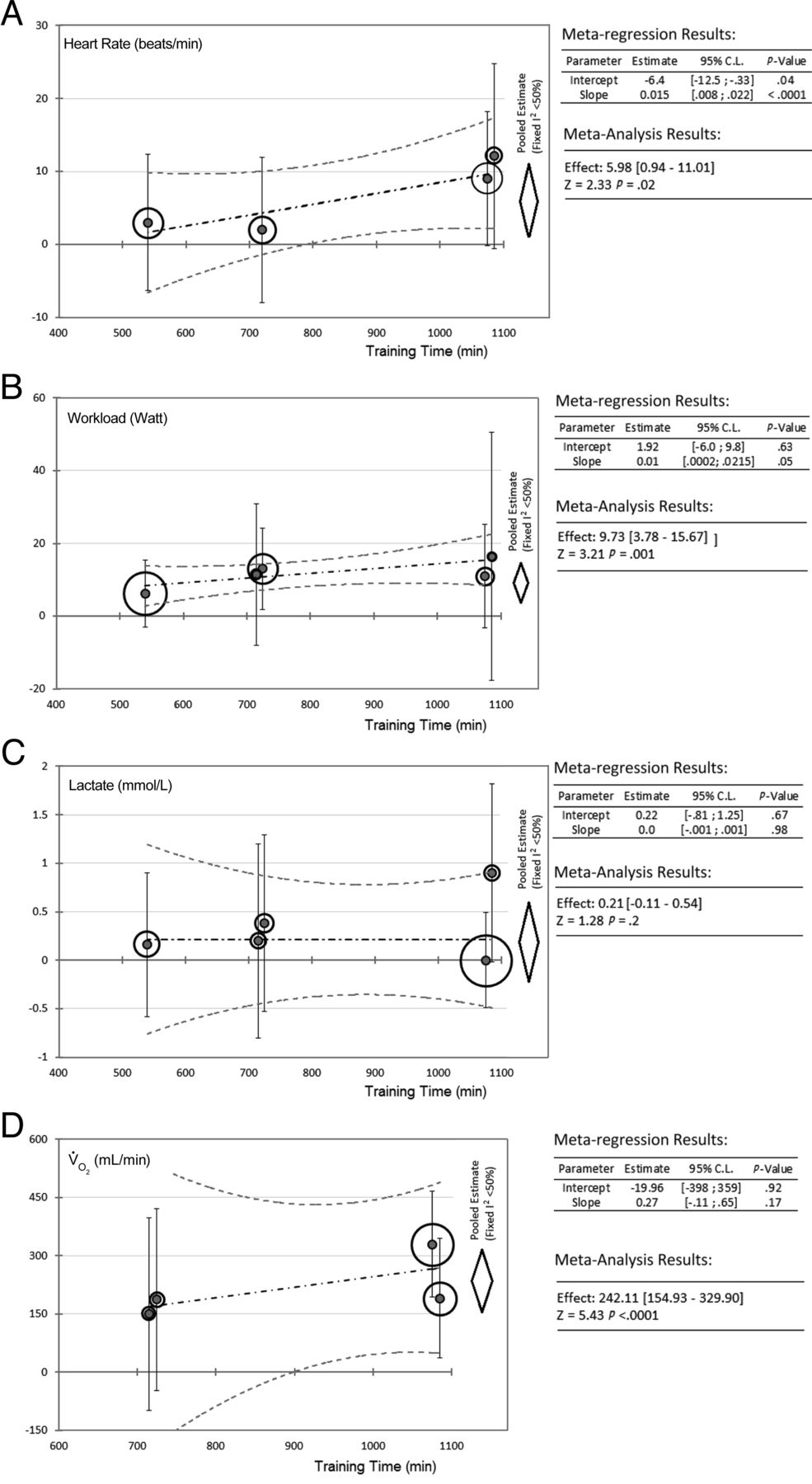
After the training schedule, clear improvements in performance were observed. The prevalence of the variable considered resulted in a clinically relevant modification after training. Heart rate at isotime improved by ∼6 beats/min (95% CI 0.98–11.01, P = .02) after training, as did work load (fixed effect mean change 9.73 [95% CI 3.78–15.67], P < .001) and V̇O2 (fixed effect mean change 242.11 [95% CI 154.93–329.9], P < .001). Even if not statistically significant, there was also a big change in lactate production after training (fixed effect mean change 0.21 [95% CI −0.1 to 0.54], P = .205).
Effect of Training Intensity on Patient Performance
The meta-regressions reported in Figure 2 show a positive relationship between variable modification and total training time for all of the outcomes considered. A statistically significant effect on slope was found when considering heart rate and work load as response variables; the random effects estimates of these slopes were 0.015 (95% CI 0.008–0.22) and 0.01 (95% CI 0.0002–0.0215) for heart rate and work load, respectively.

Random effects meta-regressions and paired comparison effect estimate in the noninvasive ventilation (NIV) arm. Evaluation of the relationship between the random effect estimate of outcome modification after training and the overall training time. Bubble diameters show study weights from meta-analysis. A: Heart rate meta-regression considered references 13, 14, 16, and 19. B: Workload meta-regression considered references 12–14, 16 and 17. C: Lactate meta-regressions considered references 13, 14, 16, 17, and 19. D: V̇O2 meta-regression considered references 12, 14, 16, and 17.
Discussion
In the articles selected, patients were trained with treadmill exercises16,17,19 or cycle ergometer12–14 with comparable outcome variables and measurement methods. Therefore, the characteristics of the rehabilitation programs were almost similar, and no evidence of biases due to any relevant difference in training method was considered as a potential confounder. On the other hand, the ventilation protocol used were objectively not homogeneous; only the studies by Bianchi et al12 and Hawkins et al13 used PAV, whereas other studies used PSV. In the studies included in our meta-analysis, the dropout rate was heterogeneous, ranging from 7.1% (4 patients of 28; 14 completed the study) in the study by Borghi-Silva et al16 to 50% (9 patients of 18) and 33% (5 patients of 15) for NIV patients and controls, respectively, in the study by Bianchi et al.12 Nevertheless, within-study dropout rates were comparable according to treatment group, and no effect due to dropout bias could be assumed as relevant. Baseline clinical and demographic variables were considered to be comparable despite a heterogeneous FEV1 at baseline. Even if the effect of these confounders was not found to be relevant from a statistic viewpoint between studies, heterogeneity could affect our results, showing a distorted effect on estimates. Regarding the comparison between the NIV and control groups, the analysis showed no clear superiority of the NIV treatment. In fact, whereas NIV showed beneficial effects on heart rate and V̇O2, these effects were not statistically significant. On the other hand, NIV treatment seems to be equivalent to the control only in terms of effects on work load and production of lactate. However, it seems that training duration could positively influence the effect of physical rehabilitation and so lead to better results. This finding is in line with previous results suggesting that a longer duration of pulmonary rehabilitation programs has a more favorable effect on exercise capacity.22–25 These last results seem to be in contrast to the general idea that NIV could improve the ability of a patient to endure an intensive exercise training session. Moreover, since no differences were found between NIV and placebo, it could be speculated that training could produce benefits regardless of NIV. On the other hand, the effect of NIV on V̇O2 and heart rate leads us to suppose that ventilation is in some way useful. In the NIV arm of our meta-analysis, patients had lower heart rates, higher work load, and improved V̇O2 after rehabilitation compared with initial values. No firm conclusion could be drawn from our results regarding the production of lactate and CO2 volume. In particular, when considering lactate, a clinical improvement was observed in all studies except in that by Borghi-Silva et al.16
In the conclusions of the articles, most authors were favorable toward the use of NIV during rehabilitation, whereas only one study12 concluded that NIV gave no additional physiologic benefit in comparison with exercise training alone. In the NIV arm of that study, the result regarding work load had the broadest CI compared with those found in the other studies; however, that study did not have an appreciable weight in the analysis (3.0%) and had only a marginal effect on the overall result. Moreover, the study by Bianchi et al12 included less severely ill patients considering the baseline FEV1. An interesting finding regarding the effect of NIV on heart rate and work load is that it seems to increase parallel to the duration of training. This trend did not emerge in the analysis regarding the number of sessions per week or the number of weeks in the training schedule. Some limitations regarding ventilation approaches arise from our work. First, it remains unclear how to define the best technique for NIV to be used to enhance exercise capability in COPD patients since different ventilation modes were used. Second, the ventilators used in the selected studies are not specifically designed to be used during physical exercise, when ventilation demand is increased. In fact, it can be assumed that the problem of patient-ventilator synchronization is more marked during exercise. In the 8 studies retained, patients were ventilated with low inspiratory pressures, which cannot produce important effects, especially during exercise; a higher inspiratory pressure may allow more firm conclusions to be made in a field that appears to be of primary importance from both a clinical and an epidemiological point of view.26–31
Moreover, PEEP is an important factor for reducing the work of breathing. PEEP was not tested in a few studies, and PEEP adjustment was never adapted to intrinsic PEEP, which has never been determined correctly. It is well known that using patient sensation for setting PEEP is not adequate33; this also could be considered as a limit.
Two more limitations could be hypothesized. First, most studies in which NIV was applied during exercise to COPD patients had no indication for long-term NIV. Second, patients with hypercapnia are more likely to benefit from NIV during the night and probably also during other different physiologic/real-life conditions such as exercise. It is to be hoped that future studies could define which subgroups of patients may benefit from NIV in view of its effects on exercise. Further studies should also be aimed at clarifying which mode and ventilator settings are most beneficial in improving exercise capability in COPD patients. In parallel, ventilator manufacturers should improve the ability of the ventilator to detect inspiratory effort in the presence of intrinsic PEEP. Some methodological limitations regarding study design arise from this work. In all of the studies considered, the number of patients who completed the study protocols was generally small, and some studies drew conclusions from extremely small samples. For example, in the study by Costes et al,14 the 7 patients enrolled in each group were assigned consecutively to one group or the other, thus generating a possible bias. Moreover, none of the studies included took into consideration the power of statistical tests performed. Furthermore, the most commonly used outcome for evaluating exercise performance in COPD patients is the 6-min walk distance. Unfortunately, only one study12 considered this test as an outcome variable.
Conclusions
Considering the small number of available articles and the technical heterogeneity regarding the ventilation protocols and the small sample sizes, we believe that this topic deserves further investigation. Randomized clinical trials with larger sample sizes based on statistical power calculations should be especially designed to investigate also the effect of training duration and intensity. In conclusion, our meta-analysis suggests that, for the moment, there is no clear evidence of superiority for the use of NIV. On the other hand, it seems that training duration could positively influence the effect of physical rehabilitation, leading to better results as reported previously.2
Footnotes
- Correspondence: Dr Cristian Ricci PhD, Department of Epidemiology and Preventive Medicine, University of Regensburg, 93053 Regensburg, Germany. E-mail: cristian.ricci{at}klinik.uni-regensburg.de.
The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}