

Abstract
BACKGROUND: Previous bench studies suggest that dynamic hyperinflation may occur if intrapulmonary percussive ventilation (IPV) is superimposed on mechanical ventilation in volume controlled continuous mandatory ventilation (VC-CMV) mode. We tested the hypothesis that pressure controlled continuous mandatory ventilation (PC-CMV) can protect against this risk.
METHODS: An ICU ventilator was connected to an IPV device cone adapter that was attached to a lung model (compliance 30 mL/cm H2O, resistance 20 cm H2O/L/s). We measured inspired tidal volume (VTI) and lung pressure (Plung). Measurements were first taken with IPV off and the ICU ventilator set to VC-CMV or PC-CMV mode with a targeted VTI of 500 mL. For each mode, an inspiratory time (TI) of 0.8 or 1.5 s and PEEP 7 or 15 cm H2O were selected. The experiments were repeated with the IPV set to either 20 or 30 psi. The dependent variables were differences in VTI (ΔVTI) and Plung with IPV off or on. The effect of VC-CMV or PC-CMV mode was tested with the ICU ventilators for TI, PEEP, and IPV working pressure using repeated measures of analysis of variance.
RESULTS: At TI 0.8 s and 20 psi, ΔVTI was significantly higher in VC-CMV than in PC-CMV. PEEP had no effect on ΔVTI. At TI 1.5 s and 20 psi and at both TI values at each psi, mode and PEEP had a significant effect on ΔVTI. With the ICU ventilators at TI 1.5 s, PEEP 7 cm H2O, and 30 psi, ΔVTI (mean ± SD) ranged from −27 ± 25 to −176 ± 6 mL in PC-CMV and from 258 ± 369 to 369 ± 16 mL in VC-CMV. The corresponding ranges were −15 ± 17 to −62 ± 68 mL in PC-CMV and 26 ± 21 to 102 ± 95 mL in VC-CMV at TI 0.8 s, PEEP 7 cm H2O, and 20 psi. Similar findings pertained to Plung.
CONCLUSIONS: When IPV is added to mechanical ventilation, the risk of hyperinflation is greater with VC-CMV than with PC-CMV. We recommend using PC-CMV to deliver IPV and adjusting the trigger variable to avoid autotriggering.
- intrapulmonary percussive ventilation
- volume controlled continuous mandatory ventilation
- pressure controlled continuous mandatory ventilation
- bench study
- hyperinflation
- lung model
- mechanical ventilation
Introduction
Intrapulmonary percussive ventilation (IPV) delivers very small bursts of tidal volume (VT), usually less than the amount of physiologic dead space, at a high frequency, within the range of 60–600 cycles/min.1 Furthermore, by providing a convective front of gas to the distal airways, IPV helps to move and clear respiratory secretions,2,3 resulting in: (1) increased mucus clearance, (2) better diffusion of oxygen and carbon dioxide into and from the alveoli, (3) higher values and more homogeneous distribution of alveolar ventilation, and (4) potential promotion of alveolar recruitment. It has been demonstrated using 3-dimensional lung imaging that a single IPV session in stable patients with COPD decreased airway resistance and increased airway volume regionally.4 As recently reviewed,5 IPV can be used either as a single treatment in spontaneously breathing patients6 or as adjunct therapy to mechanical ventilation. Five single-center randomized controlled trials testing IPV have been completed in different settings (Table 1). In patients with a COPD exacerbation, IPV was associated with a significant reduction in the need for noninvasive ventilation7 but with no change in the intubation rate for those who were treated by noninvasive ventilation.8 In patients with tracheotomies under mechanical ventilation, IPV was associated with better oxygenation and higher maximum static expiratory pressure.9 In patients with burn injury, IPV compared with volume controlled continuous mandatory ventilation (VC-CMV) improved oxygenation10 but did not reduce ventilator-free days.11 Although IPV is an unproven therapy regarding patient outcome, it is still used and, as such, should demonstrate greater benefit than harm.
ΔVTI, ΔPlung,I, and ΔPlung,E Values With Inspiratory Time Set to 1.5 s and Intrapulmonary Percussive Ventilation Set to 30 psi Working Pressure for PC-CMV and VC-CMV Modes at 2 Levels of PEEP
When used in addition to conventional mechanical ventilation, a previous bench study warned about the risk of volutrauma.12 However, in this study, conventional mechanical ventilation was done in VC-CMV mode. Pressure controlled continuous mandatory ventilation (PC-CMV) mode should better accommodate IPV13 and is the mode recommended by the manufacturer.14 The rationale relies on the basic functioning of a VC or PC breath15–17 and how PEEP is regulated. Because no study has systematically compared both modes with IPV added, we performed a bench investigation to compare VC-CMV and PC-CMV modes delivered by ICU ventilators with IPV superimposed. Our working hypothesis was that PC-CMV mode would be associated with a lower risk of volutrauma than VC-CMV mode.
QUICK LOOK
Current knowledge
Intrapulmonary percussive ventilation (IPV) may improve secretion clearance in mechanically ventilated patients. During volume controlled ventilation, the addition of IPV has been shown to increase lung volumes and cause dynamic hyperinflation, potentially risking lung injury.
What this paper contributes to our knowledge
When IPV is added to mechanical ventilation, the risk of hyperinflation is greater with volume controlled ventilation compared with pressure controlled ventilation. IPV pressure changes can also trigger the ventilator in both modes. Adjusting the trigger variable to avoid excessive triggering may also limit hyperinflation.
Methods
Equipment
Our set-up comprised the following items: (1) a sliding air-entrainment percussive device (IPV2C, Phasitron, Percussionaire Corporation, Sandpoint, Idaho), which has been regularly used by the author (Guérin) in the ICU; (2) 5 ICU ventilators labeled A–E (Avea, CareFusion, San Diego, California; Engström Carestation, GE Healthcare, Madison, Wisconsin; Evita XL, Dräger, Lübeck, Germany; NPB 840, Covidien, Mansfield, Massachusetts; and Servo-i, Maquet, Wayne, New Jersey), respectively; (3) a single-lung configuration test lung (TTL, Michigan Instruments, Grand Rapids, Michigan) with adjustable compliance and resistance and port to directly measure the pressure inside the lung (Plung); (4) a data acquisition system containing a bidirectional linear pneumotachometer (3813 series, Hans Rudolph, Shawnee, Kansas) for air flow (V̇) measurement and a straight connector (VBM Medizintechnik GmbH, Sulz am Neckar, Germany) to measure pressure at the airway opening (Pao). The pneumotachometer was linear over the 0–800 L/min V̇ range. The V̇, Plung, and Pao ports were connected to piezoresistive transducers (BD Gabarit, Vogt Medical Vertrieb GmbH, Karlsruhe, Germany). The signals were amplified, sent to analog-digital hardware (Biopac MP150, Biopac Systems, Goleta, California), and recorded at 200 Hz (AcqKnowledge, Biopac Systems).
Protocol
The experiments were conducted over a 1-d period for each ICU ventilator in our laboratory at room temperature in ambient air. The piezoresistive transducers were calibrated before the measurements were taken using a rotameter flow meter (Martin Médical, Lyon, France) for V̇ and a manometer (Fluke Corporation, Everett, Washington) for Pao and Plung.
The lung model was set to 30 mL/cm H2O compliance and 20 cm H2O/L/s resistance. The inspiratory and expiratory lines of the ICU ventilator and IPV device were plugged into the cone adapter (Fig. 1). The latter was attached to the measurement set-up (Fig. 1). For each ICU ventilator, measurements were taken while IPV was randomly set either to on or off. Two levels of the IPV device working pressure were used (20 and 30 psi) and applied randomly. VC-CMV and PC-CMV modes were randomly applied to the ICU ventilator. In VC-CMV mode, constant flow inflation, a breathing frequency of 15 breaths/min, and targeted VT of 500 mL were used. In PC-CMV mode, the pressure was adjusted to reach the same targeted VT of 500 mL. In both modes, FIO2 was set to 0.21, the heated humidifier was off, no heat-and-moisture exchanger was inserted, and the trigger was adjusted to avoid autotriggered breaths (to 2–5 L/min). In each mode, PEEP of 7 and 15 cm H2O, and TI of 0.8 and 1.5 s were tested in a random order. Therefore, 4 combinations of IPV and ventilator mode were investigated: IPV off volume controlled, IPV on volume controlled, IPV off pressure controlled, IPV on pressure controlled. Furthermore, 4 combinations of TI and PEEP were applied to each of these initial combinations (Fig. 2). For each condition (ie, each cell in Fig. 2), V̇, Pao, and Plung signals were recorded for 10 breaths after a 1-min stabilization period.
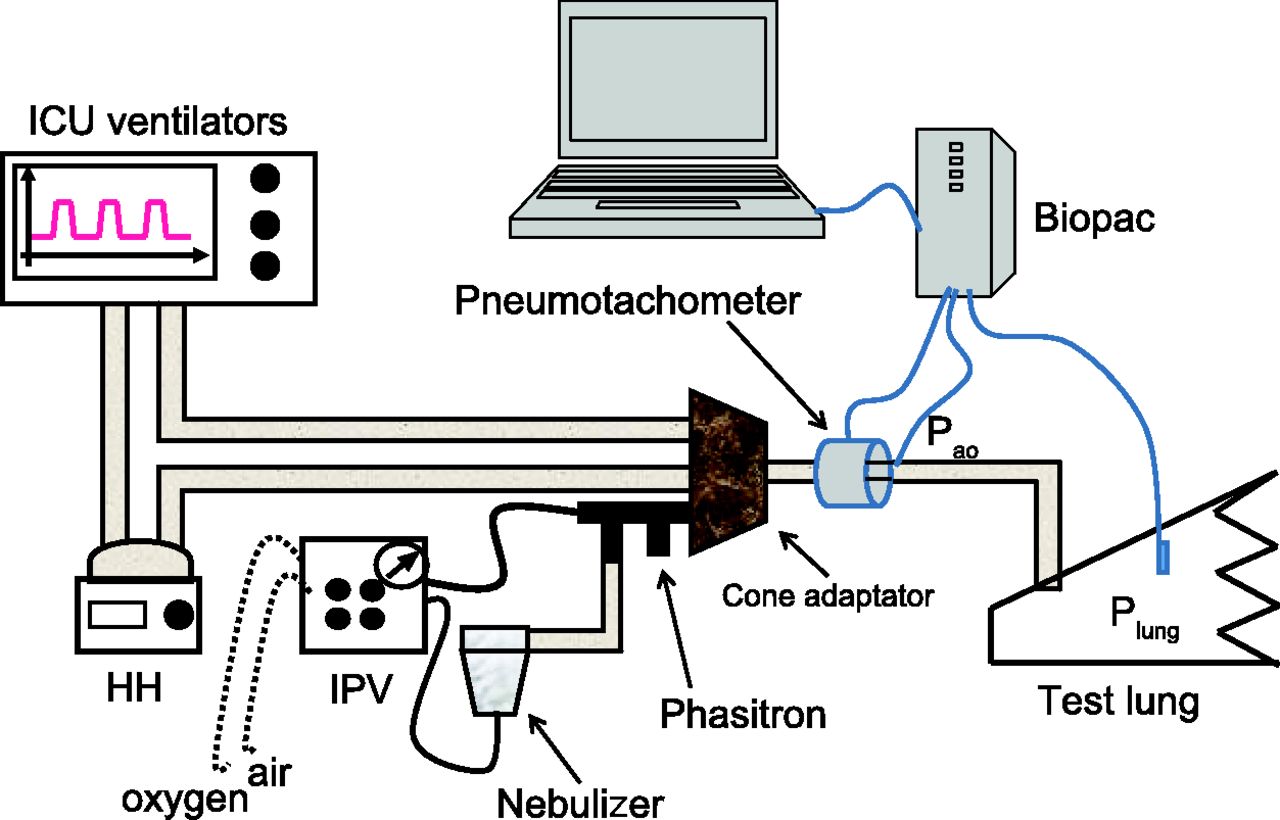
Experimental set-up used in the present study. IPV = intrapulmonary percussive ventilation. HH = heated humidifier. Plung = lung pressure. Pao = pressure at the airway opening.

Study design. IPV = intrapulmonary percussive ventilation. PC-CMV = pressure controlled continuous mandatory ventilation mode.VC-CMV = volume controlled continuous mandatory ventilation mode. TI = inspiratory time.
Data Analysis
The last 3 respiratory cycles were retained for the analysis (Fig. 3). For each ICU ventilator, 24 combinations were generated (3 IPV working pressures [0 psi with IPV off, 20 and 30 psi with IPV on] × 2 ICU ventilator modes × 2 TI × 2 PEEP levels) with 3 repetitions, making a total of 72 measurements. Inspired VT (VTI) was obtained by digitally integrating the V̇ signal.

Records of pressure at the airway opening (blue lines) and of lung pressure (red lines) obtained in pressure controlled continuous mandatory ventilation (PC-CMV) or volume controlled continuous mandatory ventilation (VC-CMV) mode with intrapulmonary percussive ventilation (IPV) either off or on. A: VC-CMV mode with IPV off. B: VC-CMV mode with IPV on. C: PC-CMV mode with IPV off. D: PC-CMV with IPV on. Inspiratory time of 1.5 s, 30 psi, and PEEP of 7 cm H2O were selected.
The main outcome measure was the difference in VTI (ΔVTI) between each IPV working pressure of 20 or 30 psi and 0 psi (IPV off). Negative values for ΔVTI indicate that VTI is lower with IPV on than with IPV off. Conversely, positive values for ΔVTI indicate that VTI is higher with IPV on than with IPV off. The secondary outcome measures were the corresponding differences in peak end-inspiratory Plung (ΔPlung,I) and end-expiratory Plung (ΔPlung,E) and in the mean airway pressure measured over the whole breath cycle. The same interpretation of the sign for ΔVTI values also applies to the sign of the values for ΔPlung,I and ΔPlung,E.
Statistical Analysis
Four different experiments were compared: TI 0.8 and 1.5 s, each with 20 and 30 psi working pressure IPV. For each of these experiments, the dependent variables ΔVTI, ΔPlung,I, and ΔPlung,E were compared between ventilator modes, taking into account interaction with the ventilator and the PEEP level using a 3-factor analysis of variance.
The values for ΔVTI, ΔPlung,I, and ΔPlung,E were expressed as mean ± SD. Statistical analysis was carried out using R2.9.0 software.18 P < .05 was set as the threshold for statistical significance.
Results
TI 1.5 s and 30 psi Working Pressure
As expected, the effect of the different factors investigated (mode, PEEP, and ventilator) was most striking for this part of the experiment because the longest TI and the highest IPV working pressure applied increased the differences between them. Therefore, these results are presented first. The mean values for ΔVTI were systematically positive in VC-CMV mode and systematically negative in PC-CMV mode (see Table 1). Therefore, ΔVTI was significantly higher with VC-CMV mode than with PC-CMV mode. The magnitude of the difference in ΔVTI between VC-CMV and PC-CMV modes and the absolute value of ΔVTI in VC-CMV mode were both clinically relevant for each ICU ventilator and PEEP. The ICU ventilator and PEEP had a statistically significant effect on ΔVTI, as did their interaction with ventilator mode.
ΔPlung,I was significantly higher with VC-CMV mode than with PC-CMV mode (Table 1). The magnitude of the difference in ΔVTI between VC-CMV and PC-CMV modes and the absolute value of ΔPlung,I in VC-CMV mode were both clinically relevant for each ICU ventilator and PEEP. The ICU ventilator and PEEP had a statistically significant effect on ΔPlung,I, as did their interaction with ventilator mode. Mode had a significant effect on mean airway pressure. (See the supplementary materials at http://www.rcjournal.com.)
Ventilator mode had no statistically significant effect on ΔPlung,E, whereas the ICU ventilator and PEEP did. There was a statistically significant interaction between the ventilator mode and the ICU ventilator.
Other Combinations of TI and Working Pressure
ΔVTI was significantly higher with VC-CMV mode than with PC-CMV mode for the 3 remaining combinations of TI and IPV working pressure (0.8 s and 20 psi, 0.8 s and 30 psi, and 1.5 s and 20 psi). (See the supplementary materials at http://www.rcjournal.com.) The ICU ventilator and PEEP (except for TI 0.8 s and 20 psi working pressure) had a significant effect on ΔVTI. The same held true for the interaction between mode and ventilator and between mode and PEEP.
The values for ΔPlung,I were statistically significantly different between ICU ventilator modes. (See the supplementary materials at http://www.rcjournal.com.) Some of these differences may be clinically important. The ICU ventilator and PEEP both had a statistically significant effect on ΔPlung,I, with a statistically significant interaction between mode and ICU ventilator and between mode and PEEP.
The same was true for ΔPlung,E, except for a lack of interaction between mode and PEEP at TI 1.5 s and 20 psi IPV working pressure. (See the supplementary materials at http://www.rcjournal.com.) However, the differences between the ICU ventilator modes for any given PEEP and ICU ventilator may not be clinically relevant, except for the highest IPV working pressure. Mode had no significant effect on mean airway pressure at TI 0.8 s and 20 psi working pressure. (See the supplementary materials at http://www.rcjournal.com.)
Discussion
We found that the risk for lung hyperinflation at the end of inspiration can be greater when IPV is used with VC-CMV mode compared with PC-CMV mode, thus confirming our working hypothesis. This result was predictable given the basic functioning of VC-CMV and PC-CMV modes as briefly summarized below. The equation of motion of the respiratory system is an appropriate tool to better understand the interaction between CMV and IPV:
 (1) where PRS is the total pressure applied to the respiratory system, Pmus is the pressure generated by the contraction of inspiratory muscles, Pvent is the ventilator pressure, E is the elastance of the respiratory system, V is the change in lung volume above end-expiratory lung volume, and RRS is the resistance of the respiratory system. In a sedated and paralyzed patient, Pmus = 0, and hence, PRS is equal to Pvent.
(1) where PRS is the total pressure applied to the respiratory system, Pmus is the pressure generated by the contraction of inspiratory muscles, Pvent is the ventilator pressure, E is the elastance of the respiratory system, V is the change in lung volume above end-expiratory lung volume, and RRS is the resistance of the respiratory system. In a sedated and paralyzed patient, Pmus = 0, and hence, PRS is equal to Pvent.
In VC-CMV mode, the ventilator flow is controlled, not the pressure (which depends on lung compliance and resistance); thus, adding IPV (a source of flow) should affect the VTI delivered: the more flow, the more VTI, the more pressure. By adding an IPV device to a ventilator in VC-CMV mode, the ventilator will have issues measuring and adjusting the VTI delivered. This is particularly true if the flow is inserted after the inhalation valve. In fact, as demonstrated by this study, the ventilators could not adjust it.
In PC-CMV mode, the mechanical breath pressure (Pvent in Equation 1) is controlled, not the VTI and flow (which are dependent on lung compliance and resistance); thus, adding IPV (a source of flow) should not affect Pvent but will affect the flow and VTI delivered. In this study, we found that actually adding IPV decreased flow and VTI delivered. By adding IPV to a ventilator in PC-CMV mode, the ventilator will try to maintain the preset airway pressure (Pvent in Equation 1). Thus, the addition of flow and pressure to the ventilator circuit will lead the ventilator to decrease flow to maintain Pvent, and the VTI delivered will decrease.
Changes in VTI and Plung,I
In VC-CMV mode, the magnitude of the absolute changes in VTI and Plung,I regularly increased with increasing TI and working pressure. In contrast, in PC-CMV mode, the changes in VTI were consistently negative, as were those pertaining to Plung,I except in some rare instances: the longer the TI, the longer the exposure to V̇ and hence the longer the exposure to the considerations discussed above.
The risk of hyperinflation at the end of inspiration is greater with VC-CMV than with PC-CMV, and hence, the ICU ventilator should be set to PC-CMV mode when IPV is used in conjunction with mechanical ventilation. We found statistically significant differences among the 5 ICU ventilators tested, although these differences may not be clinically relevant. However, with ICU ventilator A, there was a risk of reducing alveolar ventilation and promoting alveolar derecruitment once IPV was turned on, in particular with the longest TI and highest working pressure IPV. Tsuruta et al13 superimposed IPV on PC-CMV in 10 obese subjects who exhibited refractory compression atelectasis and hypoxemia after abdominal surgery. PaO2/FIO2 went up from 189 ± 63 to 243 ± 67 mm Hg 3 h after IPV onset, an improvement that was maintained over 24 h. As shown on the lung computed tomography scan done after 24 h of IPV, the dorsal lung regions, which were atelectatic before IPV, became re-aerated. Therefore, the improvement in oxygenation could be due to dorsal lung recruitment induced by IPV. Because this study was not controlled, these findings could also be explained by other factors such as the spontaneous resolution of atelectasis over time. Dellamonica et al12 argued that these results could stem from an increase in lung volume. Our present data indicate that this would not be the case, as the VTI did not increase with IPV when used in PC-CMV mode.
Change in Plung,E
In this study, we did not use PEEP of 0 cm H2O. This decision conforms to the results of previous bench studies12 and with the manufacturer's recommendations (http://www.percussionaire.com/A50474-2alog.asp). Once IPV was started, Plung,E systematically increased for each mode, with a statistically but probably not clinically significant difference between VC-CMV and PC-CMV. For the TI 1.5 s/30 psi IPV working pressure combination (Table 1), the ventilator mode had no statistical effect on the change in Plung,E, a result that could be explained by the high lung elastance set, which may have minimized the increase in Plung,E. The differences in Plung,E were statistically significant across the ventilators and these differences were clinically relevant. In particular, ventilator A was associated with the highest value of change in Plung,E in PC-CMV mode.
We noted that the effect on PEEP was not different between VC-CMV and PC-CMV modes. The reason is that PEEP is a pressure controlled phase. Thus, the ventilator will drop the pressure to the set PEEP and will attempt to maintain the pressure at the same level. Thus, the fluctuations by the IPV would result in a decrease in Pvent to maintain the same PEEP. Thus, examination of several levels of PEEP had no clear effect.
Clinical Implications
The present data recommend setting the ventilator mode to PC-CMV rather than VC-CMV using TI 0.8 s when IPV is added. The reader should be aware that once IPV is superimposed on conventional mechanical ventilation, the monitoring of delivered volume is no longer reliable. This was the case with each of the 5 ICU ventilators we tested.
Limitations
The main limitation of this study is that as an in vitro investigation, the results cannot be translated to patients. In particular, this type of study cannot assess the hemodynamic effects of the different combinations tested. Another limitation is that we tested a single combination of lung compliance and resistance. It has been shown that pressure and volume delivered by IPV are influenced by changes in lung compliance and resistance.19
In conclusion, as suggested by this bench study, when the trigger of the ICU ventilators is adjusted to avoid any autotriggered breath, the PC-CMV mode should be selected when using IPV in combination with conventional mechanical ventilation.
Footnotes
- Correspondence: Claude Guérin MD PhD, Service de Réanimation Médicale, Groupement Hospitalier Nord, CHU de Lyon, 103 Grande Rue de la Croix-Rousse, 69004 Lyon, France. E-mail: claude.guerin{at}chu-lyon.fr.
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}