

Abstract
BACKGROUND: Ventilation with low tidal volume is recommended for patients with acute lung injury. Current guidelines suggest limiting plateau pressure (Pplat) to < 30 cm H2O for septic patients needing mechanical ventilation. The aim of this study was to determine whether Pplat within the first 24 h of ICU admission is predictive of outcome and whether Pplat < 30 cm H2O is associated with lower mortality rates.
METHODS: This study was a retrospective analysis of prospectively acquired clinical data from an ICU of a tertiary referral hospital in central Taiwan. Subjects were included if they were admitted due to sepsis and respiratory failure requiring mechanical ventilation from April 2008 to November 2009.
RESULTS: There were 220 subjects (188 males, 32 females) with a median age of 76 y and a mean Acute Physiology and Chronic Health Evaluation II score of 25.0 ± 6.5. Pneumonia was the major cause of sepsis (85.5%). The hospital mortality rate was 39.1%. Pplat was higher throughout the first 24 h of ICU admission in nonsurvivors. Higher Pplat was associated with higher mortality rates regardless of acute lung injury. In multivariate regression analysis, Pplat > 25 cm H2O at 24 h after admission was an independent risk factor for mortality (adjusted odds ratio of 2.33, 95% CI 1.10–4.91, P = .03 for hospital mortality).
CONCLUSIONS: Pplat within the first 24 h of ICU admission is predictive of outcome, with lower Pplat associated with lower mortality rates. There is no safety margin for Pplat. Limiting Pplat should be considered even at < 30 cm H2O in septic patients with acute respiratory failure.
Introduction
Acute respiratory failure is common in severe sepsis. Patients with severe sepsis have increased risk of developing ARDS,1 as sepsis is also the leading cause of ARDS.2,3 Avoiding ventilator-induced lung injury4,5 by limiting pressure and volume can effectively reduce the mortality of ARDS.6,7 However, despite recent advances in understanding the mechanism and treatment of ARDS, mortality remains high.8
An international survey of adult patients receiving mechanical ventilation showed that plateau pressure (Pplat) ≥ 35 cm H2O is associated with increased ICU mortality.9 A recent study also demonstrated that limiting Pplat to < 30 cm H2O is significantly associated with increased survival.10 Current guidelines recommend limiting Pplat with an initial ceiling of < 30 cm H2O when applying mechanical ventilation to septic patients with ARDS.11,12 However, the guidelines also suggest limiting Pplat to < 20 cm H2O in patients with normal lung function in the ICU or undergoing major abdominal surgery with high risk of complications.13 Thus, it is unclear if lowering Pplat further below 30 cm H2O is beneficial. There are also limited data regarding mechanical ventilation in septic patients without ARDS.
The aim of this retrospective study was to determine whether Pplat is a surrogate marker for mortality and if initial Pplat lower than < 30 cm H2O is associated with better outcome for patients admitted to an ICU for severe sepsis or septic shock with acute respiratory failure (ARF).
QUICK LOOK
Current knowledge
Lung-protective ventilation includes low tidal volume ventilation (6 mL/kg of predicted body weight) and limiting plateau pressure (Pplat) to < 30 cm H2O. Early application of a lung-protective approach may prevent acute lung injury.
What this paper contributes to our knowledge
Lower Pplat was associated with a decreased mortality, even at levels below 30 cm H2O, in subjects with sepsis and respiratory failure. There is no absolute safety margin of Pplat in septic patients with ARF, although Pplat within the first 24 h after ICU admission is a valuable outcome predictor.
Methods
Subjects
This study was a retrospective analysis of prospectively acquired data on a cohort of subjects with sepsis and ARF admitted to the 24-bed ICU at Taichung Veterans General Hospital between April 2008 and November 2009. The hospital's ethics committee/institutional review board approved the study protocol, and the requirement for informed consent was waived. Inclusion criteria were severe sepsis or septic shock of either pulmonary or extrapulmonary origin, bundled treatment based on the Surviving Sepsis Campaign Guidelines,11,12 and respiratory failure requiring mechanical ventilation. Exclusion criteria were deviation from the treatment protocol for any reason, respiratory failure for causes other than sepsis, use of noninvasive mechanical ventilation, and incomplete data records.
Sepsis Bundle Treatment Protocol and Data Records
A protocol was set up to implement bundle treatment based on the guidelines for managing and monitoring septic patients within the first 24 h of ICU admission. If a subject had a suspected site of infection, 2 or more systemic inflammatory response syndrome criteria, and one or more organ dysfunction criteria, resuscitation procedures were applied. In this protocol, the initial resuscitation bundle included lactate measurement, antibiotic and infection source control, pathogen identification and cultures, hemodynamic stabilization, stress dose steroid use, appropriate glycemic control, and limiting inspiratory Pplat for ventilated subjects.
Hemodynamic stabilization procedures included fluid resuscitation, blood product transfusion, and inotropic agent use. Fluid resuscitation was done by monitoring and achieving 4 goals: mean arterial pressure > 65 mm Hg, central venous pressure 11–16 cm H2O, central venous oxygen saturation > 70%, and urine output > 0.5 mL/kg/h.
Pplat was recorded at the beginning of the first 24 h of sepsis bundle treatment and every 4 h thereafter. Respiratory mechanics, including tidal volume (VT), peak inspiratory pressure, Pplat, and PEEP, at each time point were also recorded. Pplat was recorded by breath-holding at the end of inspiration for 0.5 s while the subject was sedated with muscle relaxant. Lung compliance was calculated as VT/(Pplat − PEEP). VT (mL/kg) was normalized to ideal body weight: male, (height [in cm] − 80) × 0.7; and female, (height − 70) × 0.6.
The subjects' demographic and hemodynamic data, diagnosis and indication of sepsis bundle treatment, results of resuscitation goals achieved, and mechanical ventilation parameters were recorded. The degree to which the resuscitation goals were achieved was defined as the percentage of subjects who achieved all 4 goals by 6 h after admission. The Acute Physiology and Chronic Health Evaluation II (APACHE II) score was calculated on the day of admission. Chart review and chest radiograph readings were conducted by 2 intensive care physicians.
Statistical Analysis
Subjects were divided into survivor and nonsurvivor groups upon discharge from the hospital. Univariate analyses using Student t test and the chi-square test were conducted to compare the demographic, hemodynamic, and laboratory variables and the mechanical ventilation parameters between these 2 groups.
In the subgroup analysis, the cohort was divided into ARDS and non-ARDS groups according to the Berlin definition.14 Subgroup analysis was also performed based on the cause of sepsis.
A Cochran-Mantel-Haenszel chi-square test was used to compare the relationship between different Pplat levels and mortality. Multivariate analyses using a logistic regression model were done to evaluate the power of Pplat at 24 h after the start of sepsis bundle treatment (Pplat-24) for predicting hospital mortality. It was adjusted by relevant factors that influence Pplat measurement (ie, VT and PEEP) and variables with borderline significance in univariate analysis (defined as P < .2). Analysis was performed using SPSS 15.0.0 (SPSS, Chicago, Illinois). Statistical significance was set at P < .05 (2-tailed test).
Results
Subjects
A total of 279 subjects with sepsis and respiratory failure were admitted to the respiratory ICU during the study period. Fifteen subjects were excluded due to the use of noninvasive ventilation, 18 subjects were excluded because sepsis was not the main reason for respiratory failure, and another 26 subjects were excluded for deviating from the sepsis bundle treatment protocol. The remaining 220 subjects were enrolled for analysis. Based on their demographic data (Table 1), their median age was 76 y (range of 22–94 y), and 188 subjects (85.5%) were male. Pneumonia was the major cause of sepsis (85.5%), and the mean APACHE II score was 25.0 ± 6.5. The sepsis bundle goal completion rate was 55.0%. Thirty-four subjects (15.5%) had a history of chronic lung disease, including 2 subjects with asthma, 3 subjects with bronchiectasis, and 29 subjects with COPD. No subject had interstitial lung disease. The ICU and hospital mortality rates were 29.5% and 39.1%, respectively.
Demographic Data
Subject Characteristics and Outcomes
Univariate analyses of hospital survival (Table 2) showed that nonsurvivors had significantly higher APACHE II scores than survivors at hospital discharge (26.2 ± 6.8 vs 24.2 ± 6.1, P = .02). At hospital discharge, subjects with diabetes had lower mortality rates (16.3% vs 29.9%, P = .03). Baseline hemodynamic and oxygenation status, sepsis bundle goal completion (including central venous oxygen saturation, mean arterial pressure, central venous pressure, and urine output), and cause of sepsis did not significantly correlate with subject outcomes. The mean values of central venous oxygen saturation in both survivor and nonsurvivor groups were higher than the criteria desired according to the Surviving Sepsis Campaign.15 The subjects were then divided into ARDS and non-ARDS groups according to baseline oxygenation status to evaluate the power of outcome prediction of Pplat. In the ARDS group (baseline PaO2/FIO2 < 300, n = 191), nonsurvivors had significantly higher Pplat levels than survivors (Fig. 1B). P values were significant after 4 h of admission for hospital survival. In the non-ARDS group (baseline PaO2/FIO2 ≥ 300, n = 29), nonsurvivors also had significantly higher Pplat levels, and their P values were significant at all time points (Fig. 1C).
Univariate Analysis of ICU and Hospital Survival

Plateau pressure (Pplat) within 24 h of ICU admission and outcomes. Survivors had lower Pplat during the first 24 h of ICU admission both overall (A) and in subgroups (B: PaO2/FIO2 < 300; C: PaO2/FIO2 ≥ 300; D: extrapulmonary sepsis; and E: pulmonary sepsis). All points P < .05, survival versus nonsurvivors.
In subjects with sepsis caused by pneumonia (n = 188), nonsurvivors had significantly higher Pplat at baseline at all time points within the first 24 h of admission (Fig. 1D). In subjects with extrapulmonary sepsis (n = 32), the nonsurvivors seemed to have higher Pplat, but this was not statistically significant (Fig. 1E).
Pplat and Outcomes
Univariate analyses of Pplat and outcomes (Table 3) showed that, for hospital survival in the overall population, nonsurvivors had significantly higher Pplat at baseline and at all time points within the first 24 h of admission (Fig. 1A). For factors that might influence Pplat measurement, including VT and PEEP, our analysis showed that nonsurvivors had lower VT and higher PEEP (Table 3).
Pplat, VT, PEEP, and Outcomes
The receiver operating characteristic was constructed to evaluate different levels of Pplat at 24 h after admission for predicting hospital mortality (Fig. 2). The area under the receiver operating characteristic was 0.668. Using a cutoff level of 24.5 cm H2O, Pplat had 69.8% sensitivity and 56.7% specificity for hospital mortality.
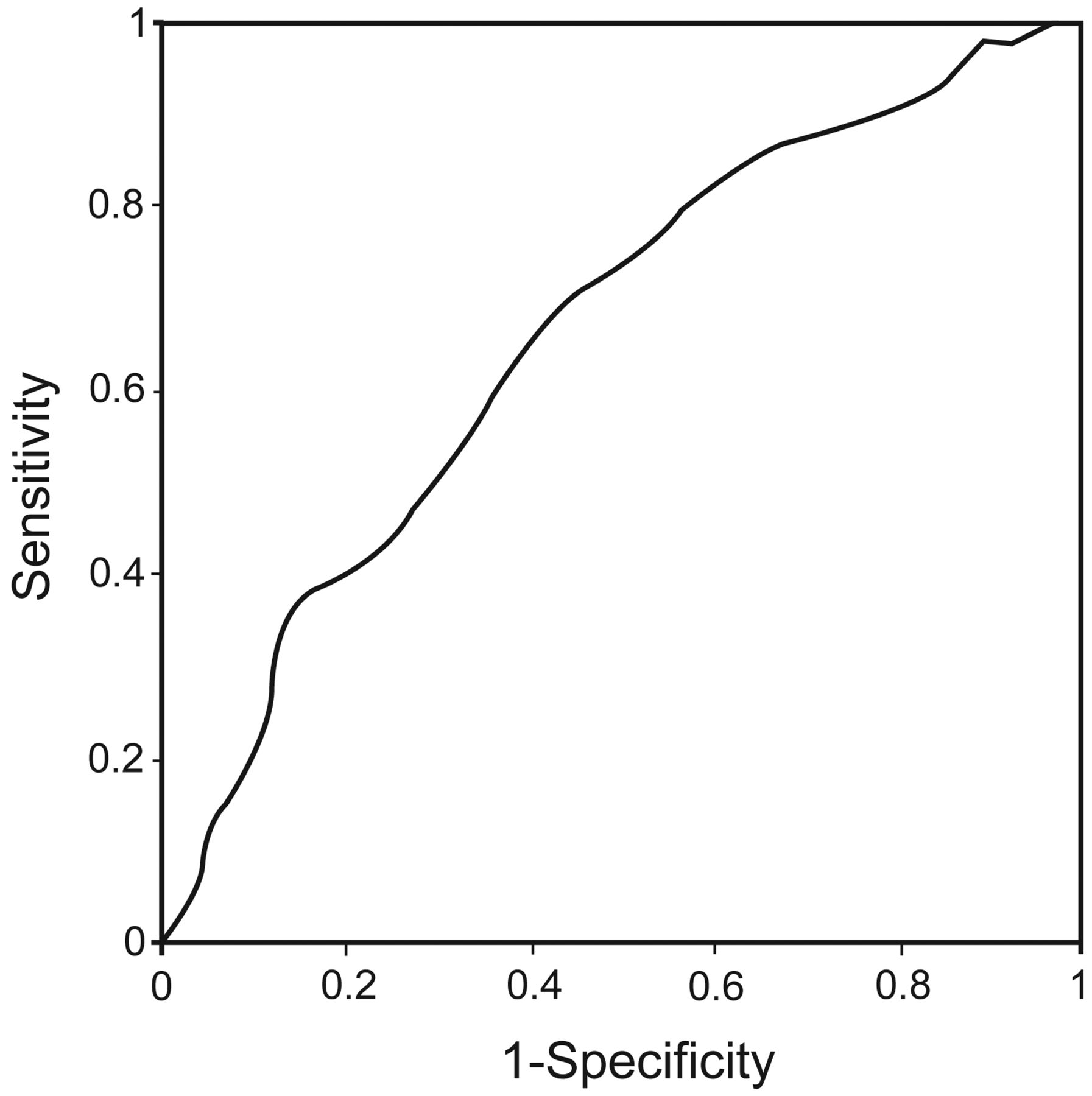
Receiver operating characteristic curves for various cutoff values of plateau pressure (Pplat) in differentiating hospital survival and mortality. The area under the receiver operating characteristic was 0.668 for hospital mortality. Using a cutoff level of 24.5 cm H2O, Pplat had 69.8% sensitivity and 56.7% specificity for hospital mortality.
The power of outcome prediction of Pplat-24 was further evaluated using a logistic regression model (Table 4). Subjects with Pplat-24 > 25 cm H2O were associated with higher hospital mortality (adjusted odds ratio of 2.89, 95% CI 1.65–5.06, P < .001). When the results were adjusted by potential confounders, including VT, PEEP, age, APACHE II score, underlying diabetes, baseline central venous pressure, goal of urine output at 6 h after admission, and causes of sepsis for ICU mortality as well as VT, PEEP, age, APACHE II score, underlying diabetes, and goals of urine output and central venous pressure at 6 h after admission for hospital mortality, Pplat-24 > 25 cm H2O remained an independent outcome predictor (adjusted odds ratio of 2.33, 95% CI 1.11–4.87, P = .03 for hospital mortality). Survivors (37.6 ± 36.0 mL/cm H2O) had better calculated lung compliance at 24 h after admission than nonsurvivors (28.1 ± 9.0 mL/cm H2O, P = .02).
Logistic Regression of Pplat at 24 h After ICU Admission in Septic Subjects With Respiratory Failure
Subjects were also grouped based on Pplat-24 ≤ 20, 21–25, and 26–30 cm H2O and ≥ 30 cm H2O. Both lower Pplat at admission (Pplat-0) and Pplat-24 were associated with lower mortality rates even when < 30 cm H2O (Fig. 3 [linear-by-linear association], panel A, chi-square value of 9.5 and P = .002 for Pplat-0; and panel B, chi-square value 16.1 and P < .001 for Pplat-24).

Lower plateau pressure (Pplat) is associated with lower mortality. Subjects were divided into 4 groups (Pplat ≤ 20, 21–25, and 26–30 cm H2O and > 30 cm H2O) according to A: Pplat at admission (P = .002) and B: Pplat at 24 h after admission (P < .001).
Discussion
This study shows that Pplat within 24 h of ICU admission was an independent predictor of outcome in subjects with severe sepsis and ARF. Higher Pplat was associated with increased mortality, even in subjects without ARDS. Moreover, lower Pplat was associated with decreased mortality rates, even at levels below 30 cm H2O.
Mechanical ventilation with a protective strategy of limiting pressure and volume to prevent ventilator-induced lung injury is the cornerstone of ARDS management. A recently published retrospective analysis of an international multi-center database showed that the presence of acute lung injury in sepsis is associated with increased mortality, whereas Pplat < 30 cm H2O is associated with increased survival.10 In this study, as determined by multivariate analysis, Pplat ≥ 25 cm H2O was an independent risk factor for hospital mortality (see Table 4). Furthermore, the increase in Pplat over the first 24 h was not related to the magnitude of mortality risk (see Table 3). Although this demonstrates that Pplat is an independent predictor of outcome in septic patients with ARF, it does not necessarily mean that Pplat < 25 cm H2O is safe.
In a previous study, decreased respiratory system compliance was independently associated with increased risk of death.16 As compliance is calculated from Pplat, PEEP, and VT, these original values can be more representative. However, Pplat measurement can be influenced by numerous factors, including PEEP, VT, and chest wall and abdominal pressure. For better estimation of transpulmonary pressure, measurement of esophageal pressure can help in setting PEEP to achieve better oxygenation and compliance.17 However, esophageal balloon estimation of pleural pressure can be influenced by several factors, including body position, intra-abdominal pressure, and different lung conditions.18 Thus, Pplat measurement remains important and practical, and its interpretation should take these factors into consideration.
Limiting Pplat to < 30–35 cm H2O is a commonly accepted concept for management of patients with respiratory failure requiring mechanical ventilation. By analyzing data from the ARDS Network trial with lower versus higher VT,7 Hager et al19 demonstrated that subjects ventilated with lower VT had lower mortality rates even when Pplat was < 30 cm H2O. In our study, most of the subjects had Pplat < 30 cm H2O, and lower Pplat-0 and Pplat-24 were associated with lower mortality rates. During positive-pressure ventilation, low VT can still augment lung injury when airway pressure is not high.20 In ARDS, because the recruitability of lung tissue is highly variable,21 the benefits of higher PEEP and recruitment maneuvers may be offset by harm from higher airway pressure.22,23 Because there is no absolutely safe level of airway pressure, management of mechanical ventilation in ARDS should aim to minimize ventilator-induced lung injury rather than target a certain Pplat level.
Currently, there is no consensus on how to ventilate patients without ARDS. A meta-analysis showed that protective ventilation with lower VT was associated with better outcomes in subjects without ARDS.24 Using lower VT and limiting Pplat for patients at risk to develop ARDS is suggested.25 Patients with sepsis and ARF are vulnerable and under constant threat of developing acute lung injury1 because they have a variety of risk factors, such as profound local and systemic inflammation, transfusion,26 mechanical ventilation,27 and massive fluid resuscitation.28 In a recently published study, ventilation with low VT of anesthetized abdominal surgery patients with high risk of pulmonary complications was associated with improved clinical outcomes.29 In non-ARDS patients, a lung-protective strategy can increase the chance of eligible and harvested lungs in brain-dead donors.30 In contrast, mechanical ventilation with VT >10 mL/kg is a significant risk for subsequent organ failure and prolonged ICU stay.31 In our study, not all of the subjects met the criteria of ARDS, and the results show that even in subjects with PaO2/FIO2 ≥ 300, the nonsurvivors had higher Pplat. To this end, prospective studies are needed to evaluate optimal ventilator strategy for patients without ARDS.
Timely and early intervention to achieve hemodynamic stabilization targeting predefined goals can reduce mortality in patients with severe sepsis.32 In this study, the rate of achieved resuscitation goals was > 50% that in a large international survey.15 The rates of resuscitation goals achieved were not different between survivors and nonsurvivors. Moreover, the mean values of central venous oxygen saturation in both groups were high, fulfilling the criteria of the Surviving Sepsis Campaign.15 This may be due to the fact that these subjects had already been resuscitated in the emergency room. Several studies have shown that conservative fluid management in subjects with ARDS can improve patient outcomes.33 Ware and Matthay34 demonstrated that impaired alveolar fluid clearance was associated with increased hospital mortality in ARDS subjects. Our results show that nonsurvivors had more positive fluid balance during the first 24 h after ICU admission. This may reflect worse hemodynamic stability and lead to increased lung edema in ARDS. However, taking fluid balance into consideration, Pplat was still an independent factor for determining subject mortality.
An interesting finding is that hospital mortality was lower in subjects with diabetes. Hyperglycemia is common in critically ill patients and is associated with increased morbidity and mortality in a variety of diagnoses.35–37 However, in severe sepsis, the presence of diabetes does not influence outcome.38 In contrast, nondiabetic patients who are hyperglycemic on admission have increased mortality rates.39 Furthermore, patients with diabetes are less likely to develop acute lung injury and have better outcomes than nondiabetic patients.40,41 Nonetheless, the relationship and mechanism of diabetes in terms of outcome in septic patients with ARDS warrant further studies.
This study has a few limitations. This is a retrospective study without blinding, and pre-specified end points may be biased by known and unknown confounders. We cannot conclude that lowering Pplat further would be helpful. Pplat may be a marker of severity of underlying illness. However, Pplat can serve as an outcome predictor in septic patients with ARF. We noted that VT was slightly lower in nonsurvivors compared with survivors. This may be because nonsurvivors had worse respiratory conditions, so we tried to better manage these subjects with regard to maintaining lung-protective ventilation goals. Another issue that should be addressed is the use of neuromuscular blockade for measurement of Pplat and management of ARDS. Currently, as it is not a standard of care, the applicability of these medications should be considered.
Conclusions
In summary, lower Pplat is associated with decreased mortality rates, even at levels below 30 cm H2O, in septic patients with respiratory failure. There is no absolute safety margin of Pplat in septic patients with ARF, although Pplat within the first 24 h after ICU admission is a valuable outcome predictor.
Acknowledgments
We thank Mr Kuang-His Chang (Department of Medical Education and Research, Taichung Veterans General Hospital, Taichung, Taiwan) for his help with statistical analysis. We are also grateful to Dr Gene Alzona Nisperos (Asia Training Solutions, Taiwan) for his help with language editing.
Footnotes
- Correspondence: Yu Ru Kou PhD, Institute of Physiology, School of Medicine, National Yang-Ming University, Taipei 11221, Taiwan. E-mail: yrkou{at}ym.edu.tw.
This study was supported by National Science Council of Taiwan Grant NSC 101-2320-B-010-042-MY3 and a grant from Aim for the Top University Plan, Ministry of Education, Taiwan. The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 147
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}