

Article Figures & Data
Figures
- Fig. 1.
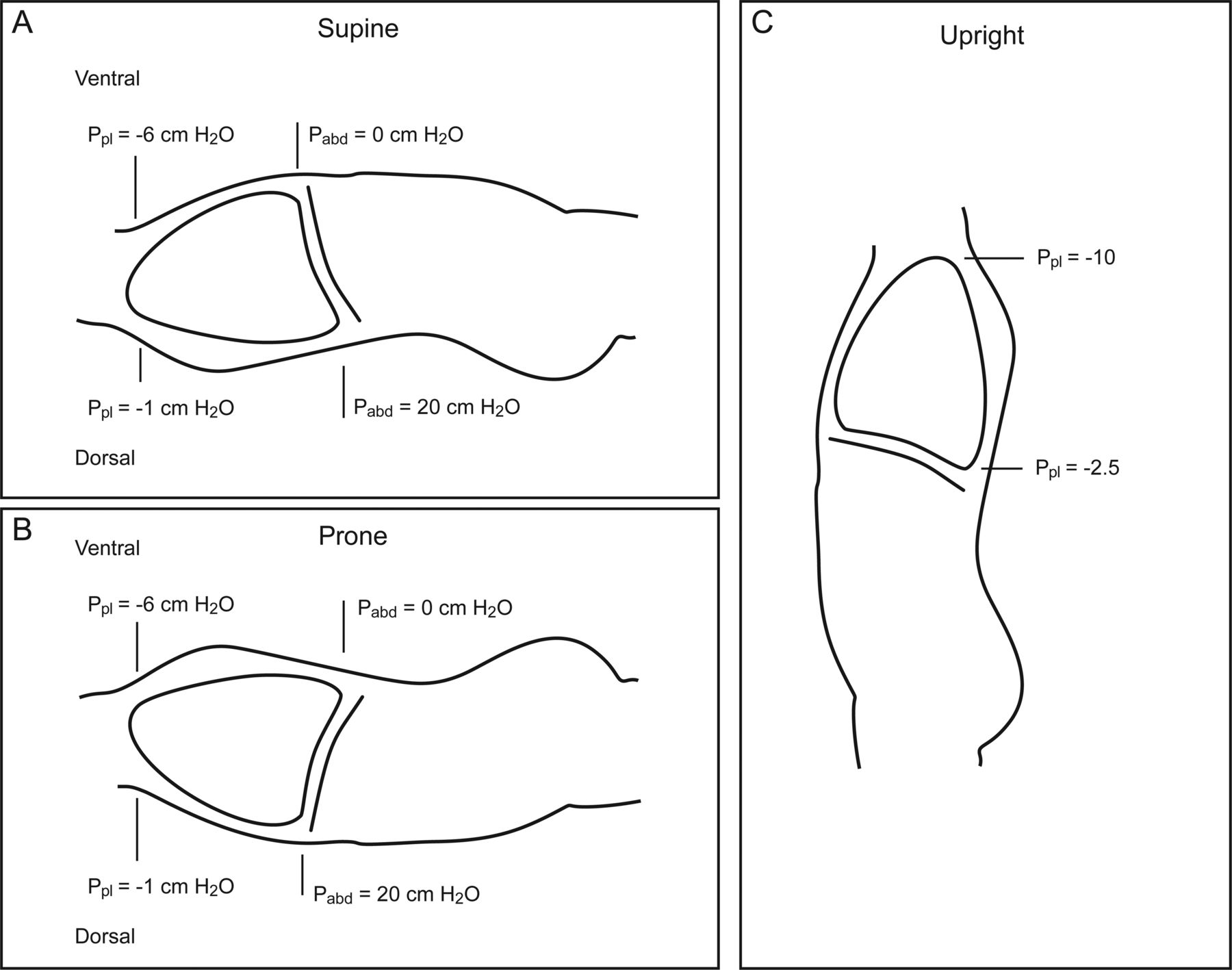
Schematic representation of vertical pleural pressure (Ppl) distribution from the apex to the bases in the upright position and their respective diminishment in the recumbent supine and prone position. Numeric values for pleural pressure and hydrostatic intra-abdominal pressure (Pabd) are based on values provided by Bryan,5 whereas those in the upright position are based upon values provided by West.16 The actual values are subject to debate due to measurement techniques and the impact of lung disease. Agostoni,17 for example, estimated slightly lower ventral-dorsal values in the recumbent supine and prone position (−4 to 0 cm H2O, respectively). Moreover, he cited evidence that increased lung density in respiratory disease may enhance the vertical gradient.
- Fig. 2.
Lateral chest radiograph of a dog with a fixed, external plumb bob to demonstrate marked improvement in dorsocaudal aeration in the prone position (top) versus the supine position (bottom). From Reference 53, with permission.
- Fig. 3.
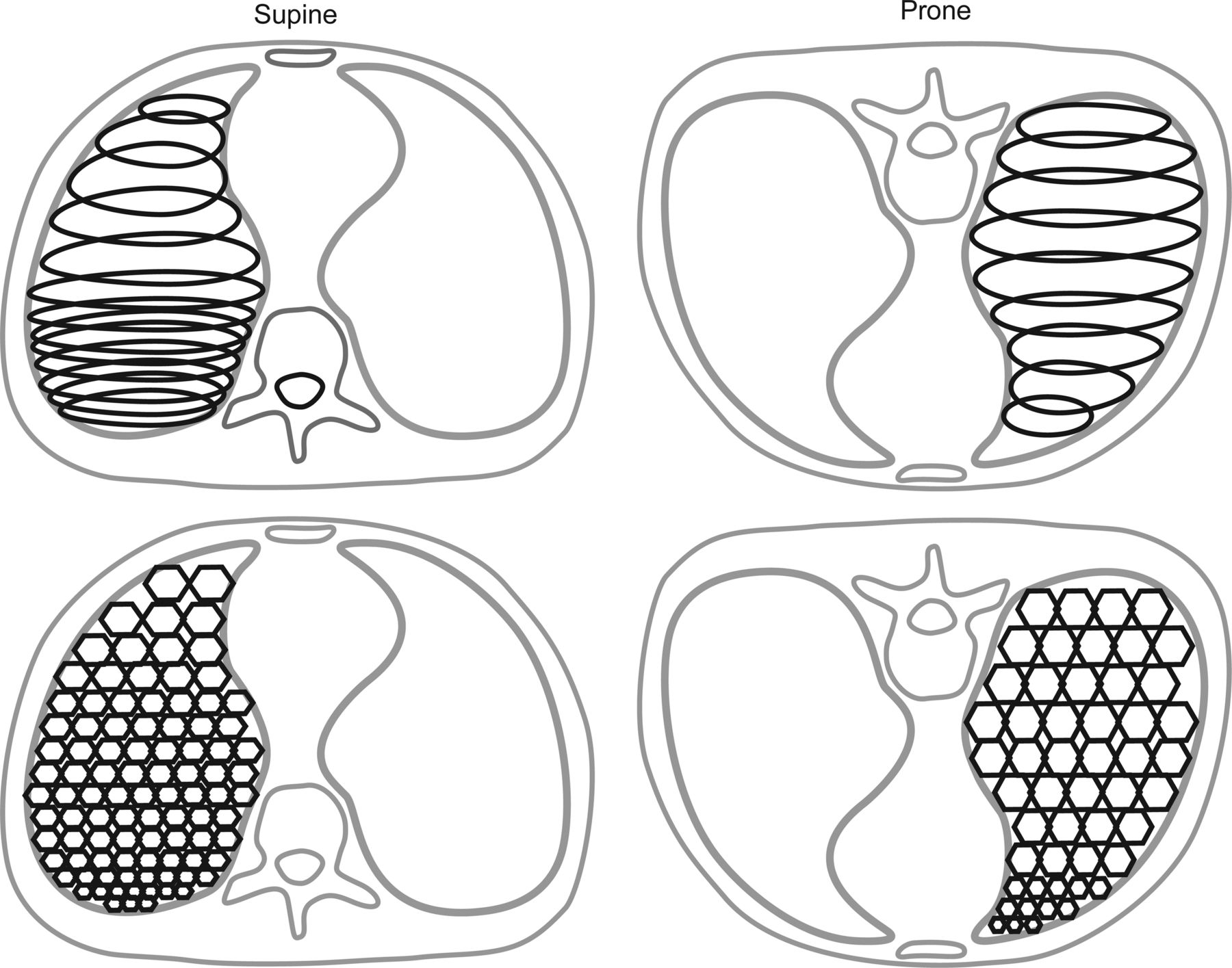
Schematic representation of strain-stress distribution and its impact on alveolar size distribution between the supine and prone position. The Slinky effect of a triangular-shaped spring suspended from its apex (supine position) causes higher strain and larger variation in the distribution of alveolar sizes due to the effects of gravity and a steeper stress production during mechanical inspiration in the upper lung regions. In contrast, suspending the spring by its base across a wider surface area (prone position) produces a more even strain and more homogeneous distribution of alveolar size that lessens inhomogeneity in stress development throughout the lungs during mechanical inspiration.
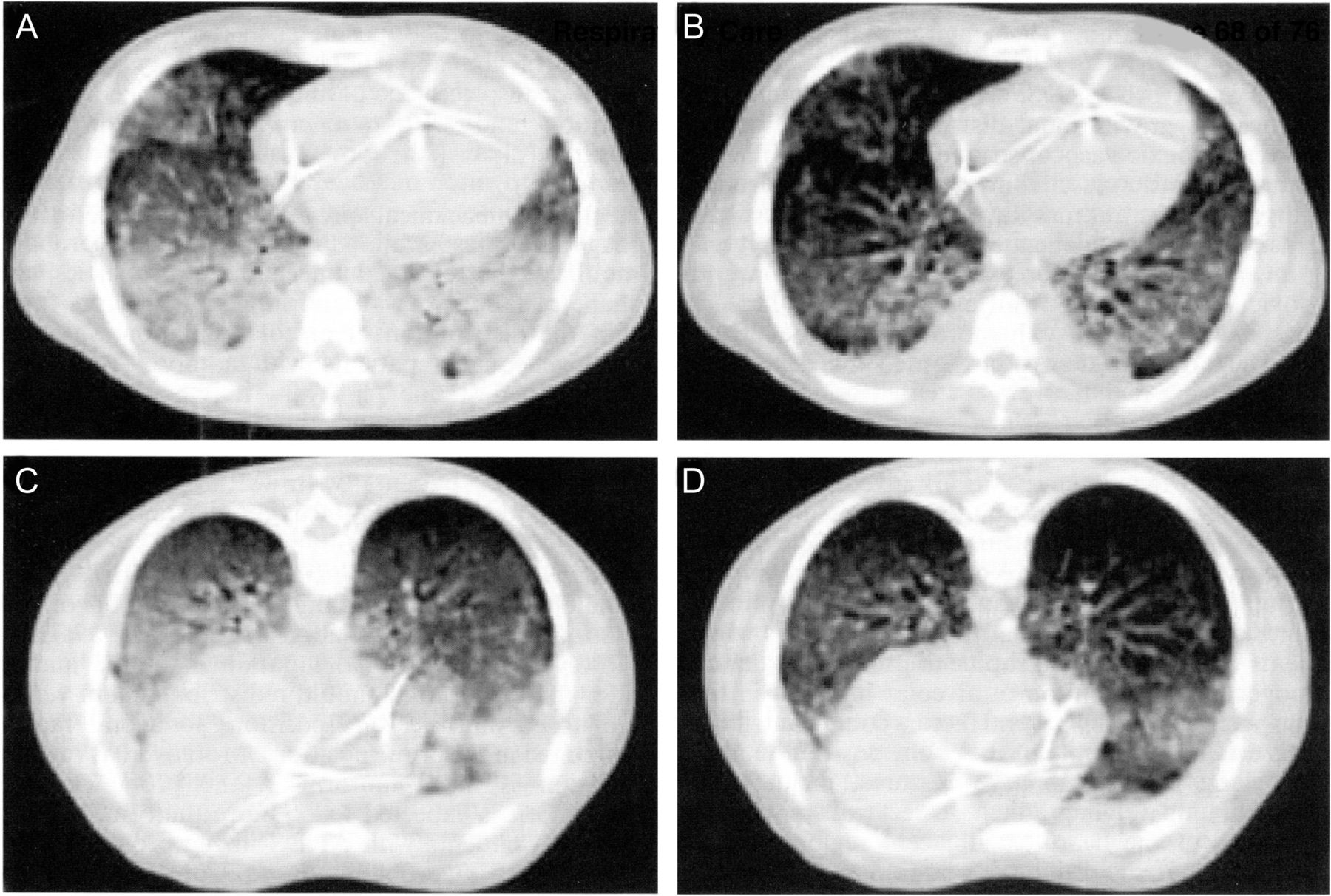
- Fig. 4.
Differences in the distribution of lung densities in a patient with ARDS on a computed tomography scan between supine position (top) and prone position (bottom). A: Image taken at end expiration in the supine position. B: Image taken at end inspiration in the supine position. Images C and D were taken from the same lung volumes in the prone position. Note the improved aeration in the dorsal lungs both at end expiration and end inspiration in the prone position compared with the supine position. From Reference 116, with permission.
- Fig. 5.
Differences in mean apoptotic index scores between the supine and prone position in an animal model of high-stretch, ventilator-induced lung injury. * = P < .05. Data from Reference 155.
- Fig. 6.
A 39-y-old obese male (body mass index of 32.2 kg/m2) with aspiration-induced ARDS developed hypotension on ARDS day 9 and suffered lobar collapse. Despite an FIO2 of 1, PEEP of 14 cm H2O, and the use of paralytics and maximal aerosolized prostacyclin (50 ng/kg/min), the PaO2 was 56 mm Hg and increased to only 63 mm Hg following a recruitment maneuver (RM) using pressure control ventilation of 45 cm H2O and PEEP of 25 cm H2O for 3 min. Although PaO2 improved minimally, physiologic dead-space ventilation (VD/VT) decreased from 0.64 to 0.60, suggesting lung recruitment. Once placed prone, the PaO2 acutely deteriorated to 49 mm Hg. In contrast, VD/VT continued to improve (0.55). At this point, the patient underwent a slow, step-wise recruitment maneuver using a fixed driving pressure of 20 cm H2O as PEEP was increased in steps of 2–3 cm H2O over 30 min to 30 cm H2O with a plateau pressure of 50 cm H2O. Thirty min later, the PaO2 increased to 128 mm Hg. At 4 and 10 h, the PaO2/FIO2 increased to >300 and >500 mm Hg, respectively. The initial prone session was maintained for 16 h. To facilitate visualization of the corresponding changes in oxygenation and VD/VT, the ratio of arterial to alveolar oxygen tension P(a/A)O2 is used. For reference, a PaO2/FIO2 <100 mm Hg corresponds to a ratio of arterial to alveolar oxygen tension of <0.15, whereas a normal value would reach 0.85. Oxygenation improvements were sustained after returning to supine position. The patient was successfully extubated 18 d later and subsequently discharged alive from the hospital.
- Fig. 7.
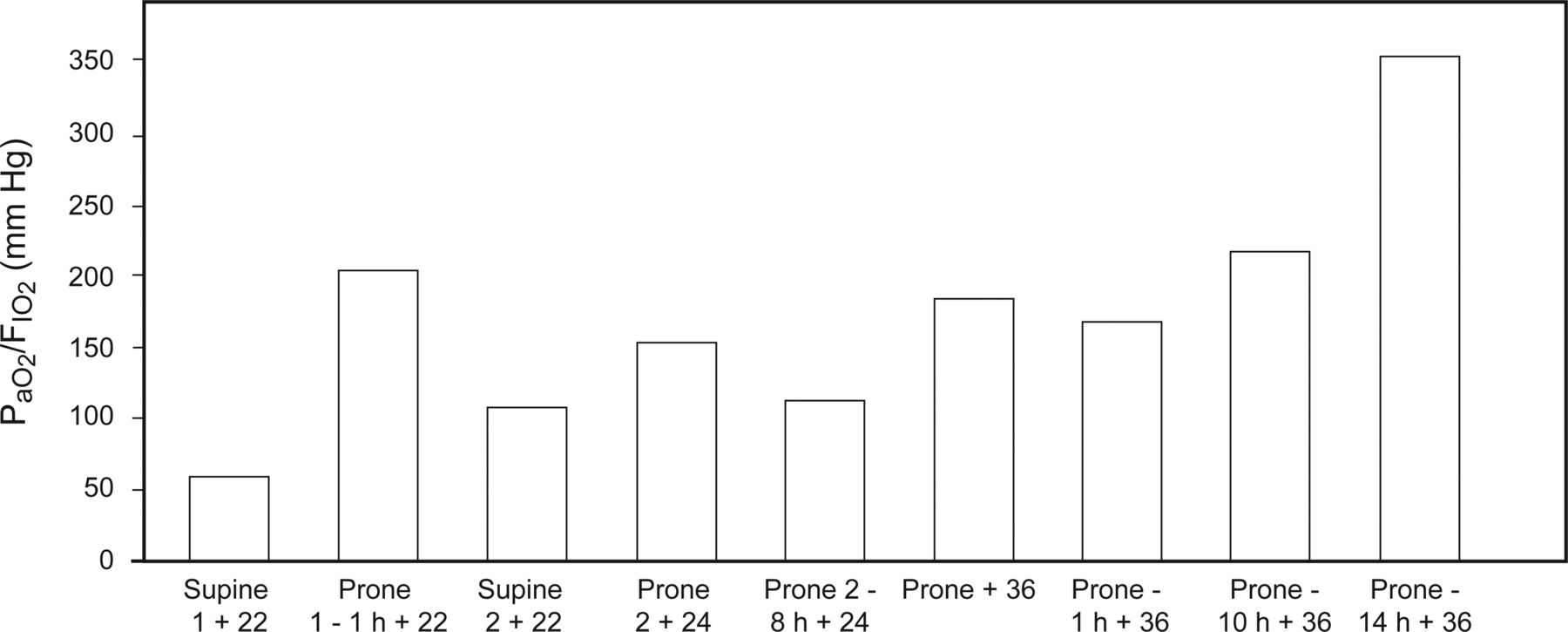
A 39-y-old pregnant female (body mass index of 36.2 kg/m2) in her third trimester who developed ARDS secondary to H1N1 influenza pneumonia underwent emergency cesarean section in the ICU for severe hypoxemia (SpO2 of 74%) with loss of fetal heart rate. She was successfully managed in SP on PEEP of 16 cm H2O until ARDS d 3, when her PaO2 fell to 48 mm Hg on an FIO2 of 1 and PEEP of 22 cm H2O (SP1+22). An hour after her first prone session, her oxygenation improved substantially (PP-1H+22) until she was returned to supine 5 h later for wound care. Her oxygenation again deteriorated despite an FIO2 of 1 and PEEP of 22 cm H2O (SP2+22). Returning her to prone resulted in transient improvement in oxygenation over the following 16 h despite increasing PEEP to 24 cm H2O (PP2+24; PP-2–8H+24). A prolonged super-PEEP recruitment maneuver as described previously (Fig 6) was implemented with a plateau pressure (Pplat) of 55 cm H2O, PEEP of 36 cm H2O, VT of 7–8 mL/kg, and breathing frequency of 30 breaths/min. Within 30 min, there was a marked improvement in PaO2/FIO2 (PP+36) that slowly increased to >200 mm Hg at 10 h (PP-10+36) and >300 mm Hg 4 h later (PP-14H+36). Despite continued episodes of derecruitment when turned to supine, the patient was managed successfully in prone at lower levels of PEEP (15 cm H2O) and without the use of paralytics over the next several days. Unfortunately, 10 d later, the patient developed severe cor pulmonale secondary to a massive pulmonary embolus and died shortly thereafter.






Tables
Online data supplement
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Effects of PP on Chest Mechanics
- Ventilation/Perfusion Relationship
- Distribution of Ventilation in PP
- Pulmonary Perfusion in PP
- Airway Closure and VA/Q Matching in Experimental ARDS and PEEP During PP
- Effects of PP on Oxygenation in ARDS
- Prevalence of Positive Oxygenation Response
- Magnitude of Oxygenation Response
- Temporal and Etiological Aspects of Oxygenation Response
- Alveolar Ventilation and Recruitment During PP in ARDS
- Effects of PP on Airway Secretion Clearance and Ventilator-Associated Pneumonia
- Effects of PP on Alveolar Fluid Clearance
- Hemodynamic Effects of PP
- Hemodynamic Effects of IAP During PP
- Effects of PP on Right Heart Function in ARDS
- Effects of PP in Acute Brain Injury
- Effects of PP on VILI in Experimental and Clinical ARDS
- Randomized Controlled Trials of PP
- Meta-Analysis of RCTs
- Adverse Events Associated With PP
- Incorporating PP Into Bundled Care
- High-Level PEEP and Recruitment Maneuver
- Inhaled Vasodilators
- Extracorporeal Membrane Oxygenation
- Practical Considerations: Indications, PEEP Strategy, Deescalating Therapy
- Manual Versus Automated PP
- Incorporating Continuous Rotational Therapy With PP
- Summary
- Footnotes
- REFERENCES
- Figures & Data
- Supplemental
- Info & Metrics
- References