

Abstract
BACKGROUND: Protective lung ventilation requires calculating predicted body weight (BW) from height. Thus, inaccuracy of height data in the electronic health record (EHR) is a risk factor for ventilator-induced lung injury. Charted height data often have uncertain accuracy. Study purposes were (1) to evaluate the difference between patient height charted in the EHR and predicted height (PH) from ulnar length and (2) to determine how the height data source affects predicted BW and the resulting values for protective tidal volume (VT).
METHODS: Subject height data from the EHR were collected from several ICUs. Simultaneous ulnar data were collected by measuring ulnar length (cm): male PH (cm) = 79.2 ± 3.60 × ulnar length; female PH = 95.6 ± 2.77 × ulnar length. For each subject, BW (kg) was calculated from height charted in EHR and from predicted height: male BW = 50 ± 0.91 × (height − 152.4); female BW = 45.5 ± 0.91 × (height − 152.4). Then VT was calculated as 8 mL/kg BW. Bland-Altman analysis of height and VT differences (charted − predicted) determined the limits of agreement.
RESULTS: For white males (n = 27) the mean (SD) height from EHR was 177 (7.5); predicted height was 178 (6.9). The limits of agreement for height in males were −18.5 and 17.8 cm. The limits of agreement for females were −23.1 and 21.3 cm. The limits of agreement for VT in males were −1.8 and 1.8 mL/kg. The limits of agreement for VT in females were −3.0 and 2.9 mL/kg.
CONCLUSIONS: For overall populations, mean height calculated from values charted in the EHR is similar to that estimated from ulnar length. However, for individuals, differences in height between the 2 sources can be large, leading to large differences in predicted BW and resultant VT set in terms of mL/kg.
Introduction
The current standard of care for mechanically ventilated patients includes limiting tidal volume (VT) to protect a patient's lungs from ventilator-induced lung injury (VILI).1 VT is based on predicted body weight (PBW) (eg, between 6 and 8 mL/kg PBW). But to determine PBW, we typically use prediction equations based on the patient's height.2,3 Therefore, the ability to protect the lungs ultimately depends on the accuracy of height data. Inaccurate height data can be dangerous because overestimating a person's height would lead to a VT larger than necessary, therefore increasing the risk of VILI. In fact, a recent study4 illustrated the importance of controlling VT when it found that an increase of 1 mL/kg PBW in initial VT was associated with a 23% increase in ICU mortality risk.
Recognizing that height data charted in the patient's electronic health record (EHR) is a critical piece of patient information, we conducted an informal survey of nurses in various nursing units at the Cleveland Clinic to determine how height data are obtained upon a patient's admission. We found that height records are often based on patient self-reporting or visual estimates. However, visual estimates and even bedside tape measurements of height in ventilated patients may be inaccurate.5 A possible alternative source of data is the height predicted by ulnar length.6
The purposes of this study were (1) to evaluate the difference between patient height of unknown origin charted in the EHR and height based on ulnar length and (2) to determine the effect of the height difference in setting lung-protective VT during mechanical ventilation.
QUICK LOOK
Current knowledge
The current standard of care for mechanically ventilated patients includes limiting tidal volume (VT) to prevent ventilator-induced lung injury. VT is based on predicted body weight (PBW) as determined from patient height and gender. This highlights the need for accurate height data. Inaccurate height data may lead to excessive VT, increasing the risk of ventilator-induced lung injury.
What this paper contributes to our knowledge
In this study, mean height calculated from values charted in the electronic health record was similar to that estimated from ulnar length. However, for individuals, differences in height between the 2 estimates could be large, leading to large differences in PBW. These differences in PBW could in turn lead to clinically important differences in VT. In the absence of accurate height measurements, the height should be based on the primary goal of patient safety during mechanical ventilation.
Methods
The study was deemed quality improvement by our institutional review board. Subject height data were collected from the EHR for all patients from medical, neuro-, and surgical ICUs. Ulnar height data were collected by measuring the span between the styloid process and the olecranon process of the ulna (Fig. 1). An average of 3 measurements (all collected by the same person) was used in the prediction equations. Predicted height (PH)7 (cm) was calculated as follows: Male PH = 79.2 ± 3.60 × ulnar length (cm); Female PH = 95.6 ± 2.77 × ulnar length (cm).

Ulnar height data were collected by measuring the span between the styloid process (A) and the olecranon process of the ulna (B). Courtesy the Cleveland Clinic Foundation.
For each subject, BW (kg) was calculated from height recorded in the EHR and from the predicted height1: Male BW = 50 ± 0.9 1 × (height − 152.4); Female BW = 45.5 ± 0.91 × (height − 152.4).
To address the first study purpose, we evaluated the difference in height data, defined as: EHR height − ulnar-based predicted height. To address the second study purpose, we first calculated BW for each subject using the 2 estimates of height. We then calculated VT at 8 mL/kg (upper end of clinically acceptable range) as a worst case scenario in terms of the risk of VILI.
Data Analysis
We used Bland-Altman analysis (corrected for small sample size8) to describe the differences in height and VT expected for individuals (as opposed to populations). This analysis plots the estimated “true” value as the mean of each pair of individual EHR- and ulnar-based measurements versus the difference between the two. The average difference is called the bias, and the SD of the differences is used with the bias to define the limits of agreement between the 2 measurement methods. The limits of agreement that we calculated represent the range of values within which 95% of future individual measurements will lie with 99% confidence.
Results
We did not collect enough data to include Asian (n = 1) or African-American males (n = 7) or African-American females (n = 4). For white males (n = 27), the mean (SD) height from the EHR was 177 (7.5) cm. The mean predicted height (from ulnar measurement) was 178 (6.9) cm. For white females (n = 24), the mean height from the EHR was 162 (9.3) cm. The mean predicted height (from ulnar measurement) was 163 (5.5) cm.
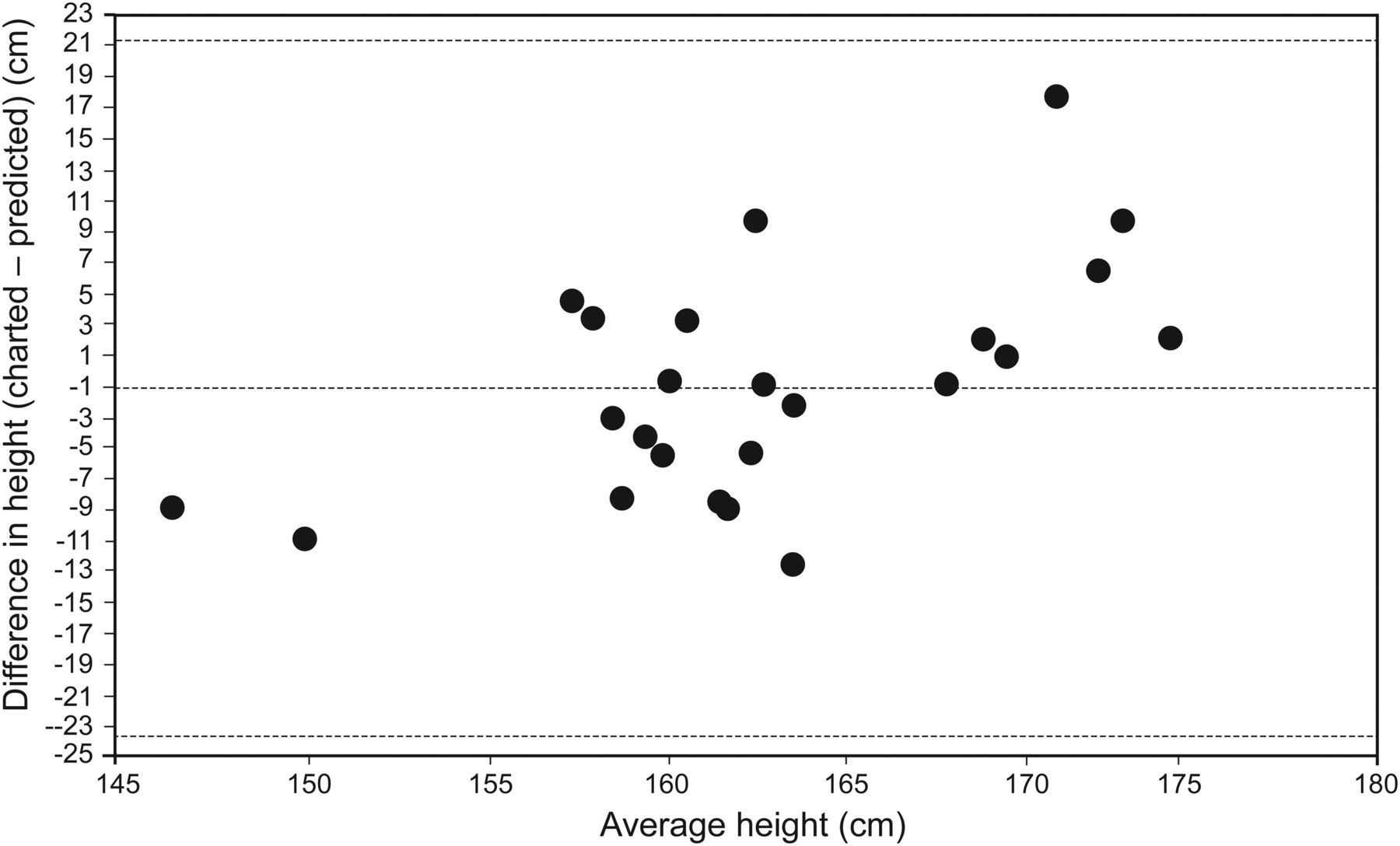
The limits of agreement for height in males were −18.5 and 17.8 cm (Fig. 2). The limits of agreement for females were −23.1 and 21.3 cm (Fig. 3). Ulnar-based height was less than charted height for 14 of 27 males (52%) and 10 of 24 females (42%).

Bland and Altman analysis of heights for males. Outside dashed lines denote the upper and lower limits of agreement, and the center dashed line shows the mean.

Bland and Altman analysis of heights for females. Outside dashed lines denote the upper and lower limits of agreement, and the center dashed line shows the mean.
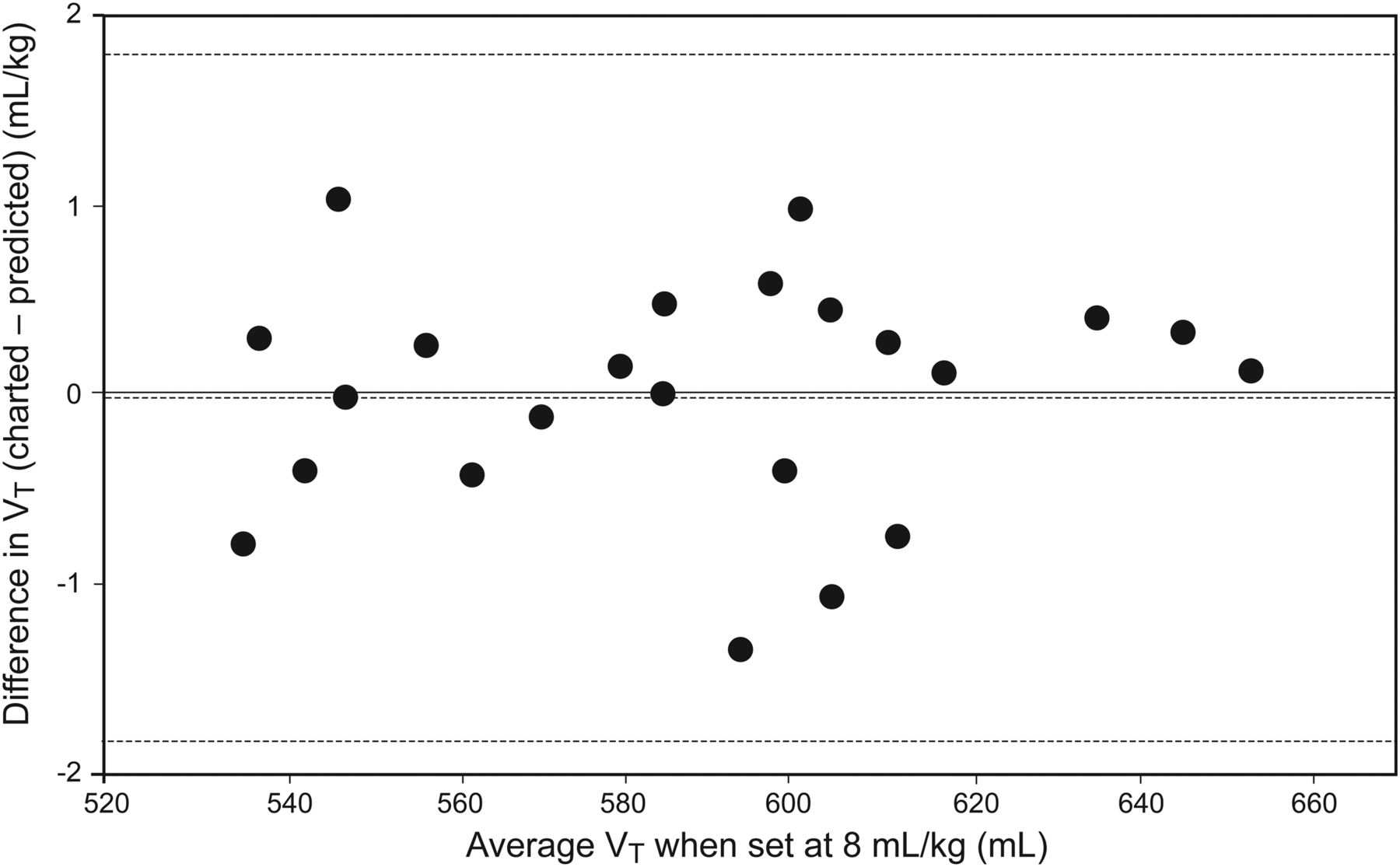
The vertical axes of the Bland-Altman plots for VT are labeled in units of mL/kg to be more clinically relevant. Two different axes are possible, depending on which estimate of weight is used as the reference (ie, based on charted height vs predicted height). For example, we found that in males, the mean difference was −0.07 (based on charted height) versus −0.02 mL/kg (based on predicted height), whereas the upper limit was 1.8 versus 1.8 mL/kg, and the lower limit was −1.9 versus −1.8 mL/kg. For females, the mean difference was −0.2 versus −0.1 mL/kg, the upper limit was 2.8 versus 2.9 mL/kg, and the lower limit was −3.2 versus −3.0 mL/kg. Because these values were so close, we graphed only the values using the data based on the predicted heights (Figs. 4 and 5).

Bland and Altman analysis of VT for males. Outside dashed lines denote the upper and lower limits of agreement, and the center dashed line shows the mean.

Bland and Altman analysis of VT for females. Outside dashed lines denote the upper and lower limits of agreement, and the center dashed line shows the mean.
The horizontal axes for the Bland-Altman plots for VT are given in mL because units of mL/kg would have yielded only 1 point (ie, the values for average VT are those calculated as 8 mL/kg based on the 2 estimates of weight).
Discussion
The differences in mean values for height (1 cm) or BW (−0.3 kg) were clinically unimportant. This is similar to the results of Bojmehrani et al5 (visual height = 169.6 cm, tape measure height = 169.4 cm, ulnar-based height =167.2 cm). Their study concluded that in comparison with the reference method, estimating the height visually and using the tape measure (potential sources of our EHR data) were less accurate than ulnar-based measurements. However, those conclusions were made for populations of subjects and did not address expected results for individuals.
When using BW to set VT (in this case at 8 mL/kg), we observed clinically important differences, depending on whether the weight was derived from charted height values in the EHR or from estimated height based on ulnar length. The difference in VT (EHR-based minus ulnar-based) could be about 2 mL/kg for white males and about 3 mL/kg for white females (based on the limits of agreement). The problem is that the Bland-Altman analyses tell us only the potential magnitudes of expected differences, not the direction for any specific subject. For an individual patient, the most appropriate VT is based on the most accurate height. The most accurate height might be the one charted in the EHR, the one predicted from ulnar length, or some other value. This study postulates that the clinician has only 2 values for height and must decide which one to use. The uncertainty indicated by our study results is large enough to cause clinical concern. For example, if the clinician thought the VT was set at 8 mL/kg but it was actually 10 or 11 mL/kg, this would be a cause for concern in terms of the risk of VILI. On the other hand, if the true VT was actually 4 or 5 mL/kg, this might be a concern in terms of patient-ventilator asynchrony.9 Therefore, which height estimate to use for BW and setting VT would presumably be based on the primary clinical goal of mechanical ventilation (ie, safety or comfort) for a particular patient.
The major limitations of our study were the small sample size and the fact that only white males and females were included. The small sample size leads to large values for the limits of agreement. Alternative methods to obtain patients' height have been based on lower leg and ulnar measurements and are useful to facilitate lung-protective ventilation. We only studied the ulnar length method because we found more references and better operational instructions for it, and it has been referenced frequently in nutrition studies.
Conclusions
For the population of subjects in this study, mean height calculated from values charted in the EHR is similar to that estimated from ulnar length. However, for individuals, differences in height between the 2 estimates can be large, leading to large differences in BW. These differences in BW lead to clinically important differences in VT when set in mL/kg. In the absence of known accurate height measurements, which height estimate to use for BW and setting VT should be based on the primary clinical goal of mechanical ventilation (ie, safety or comfort) for a particular patient.
Footnotes
- Correspondence: Matthew C Jurecki RRT, Cleveland Clinic, 9500 Euclid Ave., M56, Cleveland, Ohio 44195. E-mail: jureckm{at}ccf.org.
Mr Jurecki presented a version of this paper as an Editors' Choice abstract at the Open Forum of the American Association for Respiratory Care 60th International Respiratory Convention and Exhibition, held December 9–12, 2014, in Las Vegas, Nevada.
Mr Chatburn has disclosed relationships with Hamilton, Invacare, and IngMar.
See the Related Editorial on Page 1852
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}