

Introduction
Diaphragmatic injuries are relatively rare, and they are the result of penetrating or blunt trauma. Blunt diaphragmatic rupture occurs mainly from high-speed motor vehicle crashes. Sudden increase in intra-abdominal pressure may cause a diaphragmatic tear and visceral herniation. The magnitude of the pressure load on the inflexible central tendon by rapid deceleration may cause such catastrophic injury. The predicted outcome for these patients is associated with the severity of the disruption. However, diaphragmatic rupture may go unnoticed, and in many cases, diagnosis is delayed. In the delayed phase, symptoms are nonspecific and suggestive of other disorders, such as COPD and partial bowel obstruction. Clinical suspicion and a past history of multi-trauma are very important and useful to avoid diagnostic pitfalls. We present the case of a female patient with dyspnea due to delayed diagnosis of diaphragmatic rupture.
Case Summary
A 35-y-old woman presented to our department with severe and acute pain located in her left shoulder, lower thoracic region, and epigastrium, dyspnea, productive cough, and nausea and vomiting of 3 d duration. One y prior to presentation, the patient was involved in a car accident and hospitalized in an ICU for 2 months because of severe lung injury. Multiple left-sided ribs and both tibia were fractured. Diaphragmatic injury was not detected then.
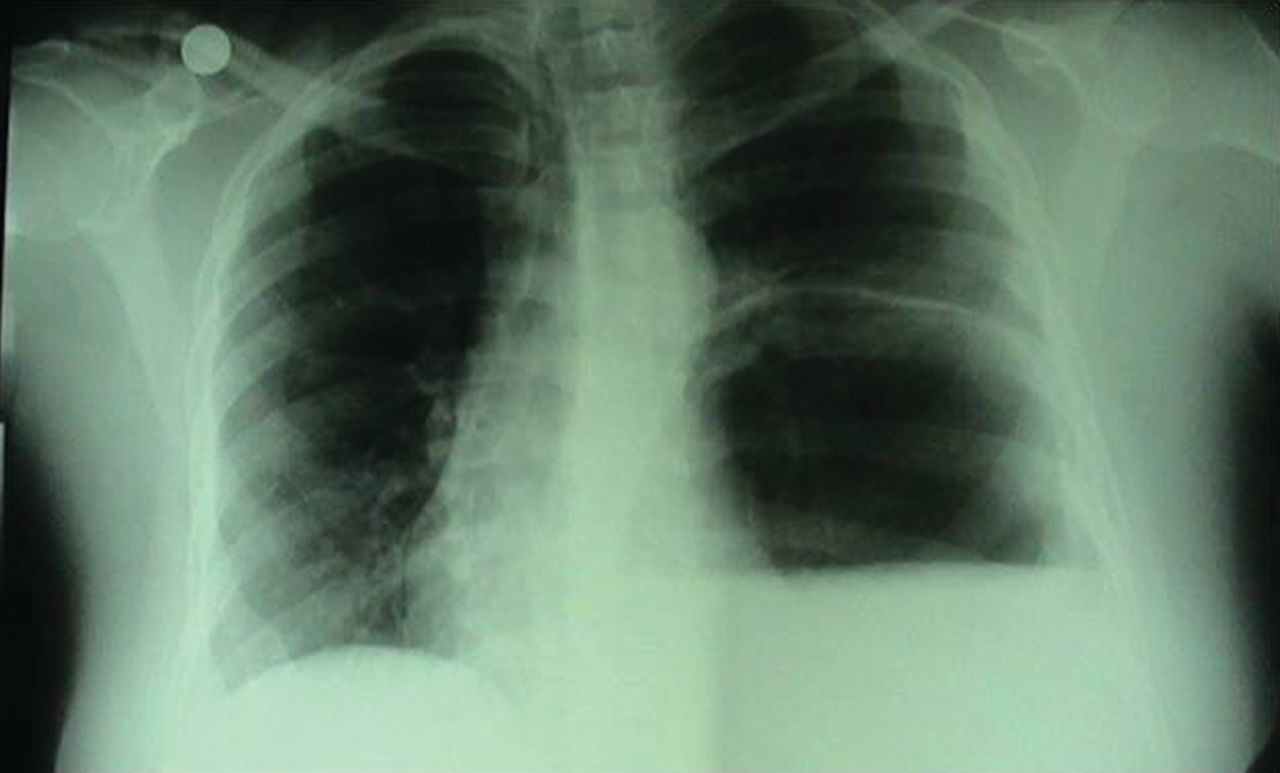
The patient was afebrile but distressed due to tachycardia and dyspnea. She was hemodynamically stable, with a heart rate of 110–120 beats/min and a breathing frequency of 20–25 breaths/min. Her PaO2 was 70–75 mm Hg on 4 L/min oxygen delivered via a nasal cannula. On examination, she was tender in the left upper quadrant. A stethoscope determined that there were no lung sounds in the left side. Chest x-ray showed a left-sided cavity with air-fluid level, multiple old fractured ribs in the left side, and an indistinct costophrenic angle (Fig. 1).

Left-sided cavity with air-fluid level.
Typically, thoracocentesis to obtain a sample of pleural fluid for diagnostic purposes would be the next step. Pleural fluid drainage would be the best management for dyspnea relief. However, the history of multi-trauma and the suspicion of diaphragmatic rupture prevented us from performing any invasive procedure before obtaining more imaging details.
A contrast-enhanced chest computed tomography (CT) scan revealed discontinuity of the left hemidiaphragm with gastric herniation and mild mediastinal shift to the right. The stomach abutted the left posterior ribs, which was a positive dependent viscera sign (Figs. 2⇓–4)

Computed tomograph shows gastric herniation (sagittal view).
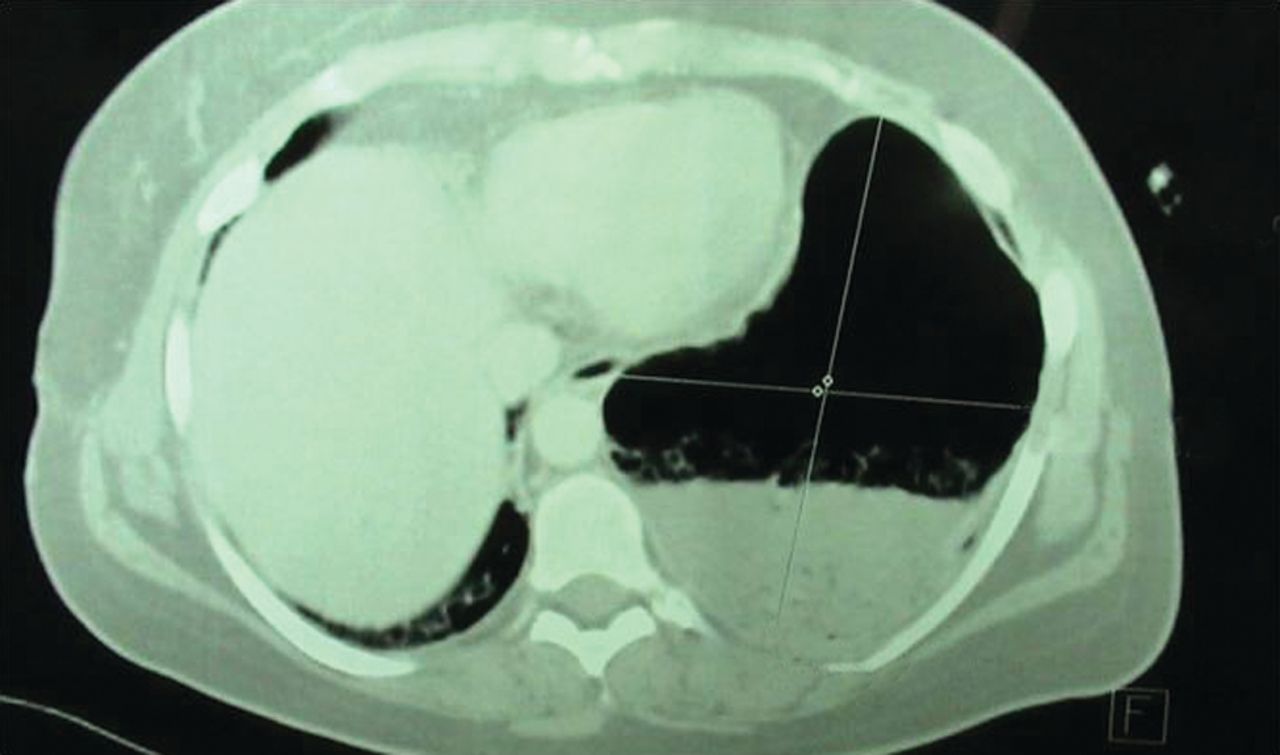
Stomach lies dependent on left posterior ribs, which is a positive dependent viscera sign.
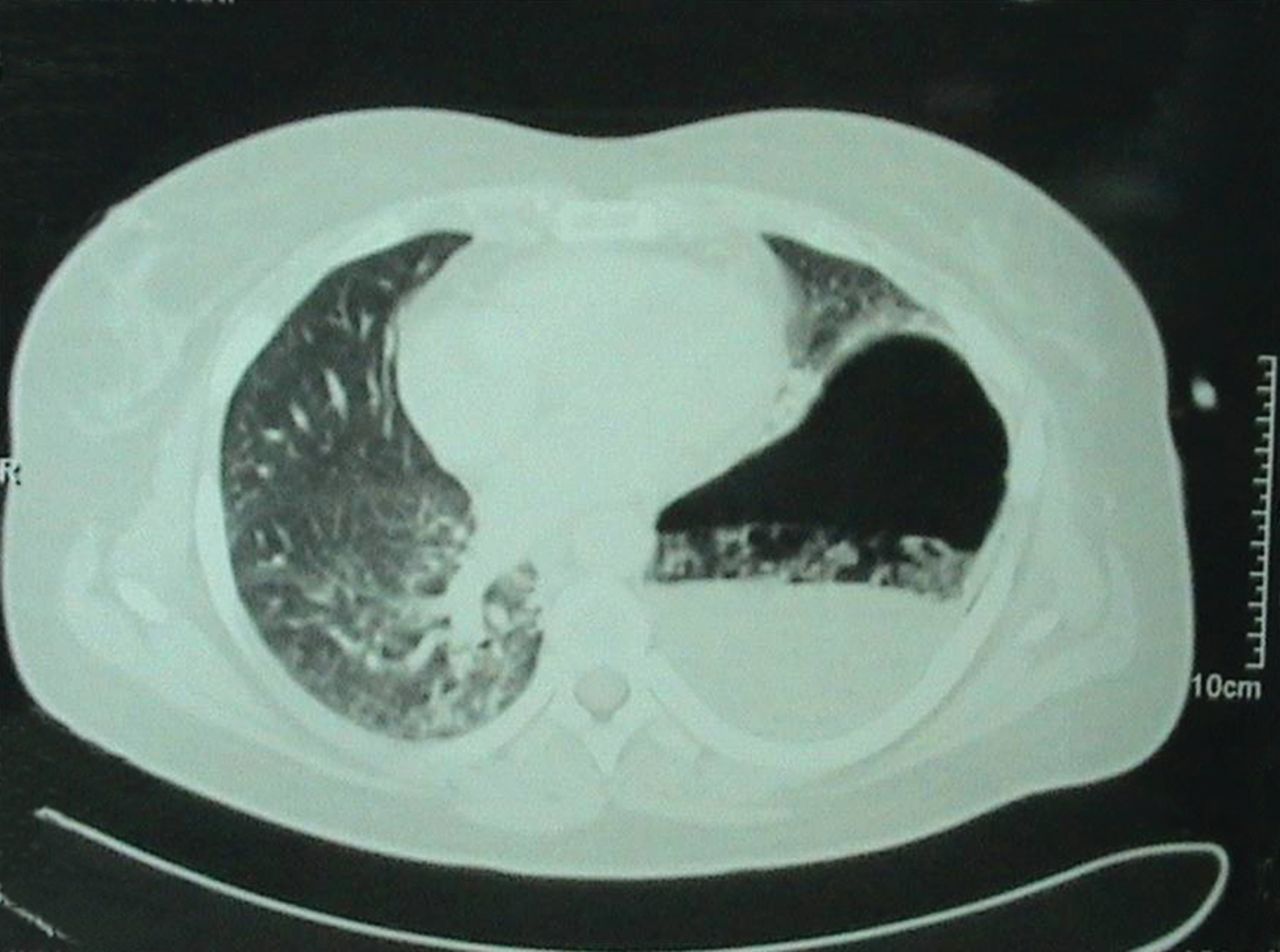
Axial computed tomography scan shows mild mediastinal shift to the right and a positive dependent viscera sign.
After confirming the diagnosis of delayed diaphragmatic rupture, surgical treatment was required to repair the defect. A left posterolateral thoracotomy was performed under general endotracheal anesthesia. Intrathoracic stomach herniation through a ruptured left hemidiaphragm was identified. The herniated content was returned to the abdominal cavity. The diaphragmatic defect was repaired primarily by interrupted full-thickness nonabsorbable sutures. The patient spent 1 d in the ICU, and her postoperative hospital stay and follow-up were uneventful.
Discussion
Diaphragmatic rupture may result from traumatic injury usually from thoracoabdominal trauma, with an incidence of 0.8–5%.1 It is estimated that up to 30% of blunt diaphragmatic ruptures may appear as late presentations, and < 2.7% are detected during the first 4 months after injury.2,3 Diaphragmatic rupture is more common in the left side because the liver protects the right hemidiaphragm. Only 13% of traumatic diaphragmatic hernias are right-sided.4 Bilateral injuries are not usual (2–6% of total cases). Ruptures are typically located in the posterolateral aspect of the hemidiaphragm because this area is embryologically weaker.5
Abrupt increases in intrathoracic and intra-abdominal pressure against the diaphragm (usually as a consequence of high-velocity trauma to the abdomen and chest) and diaphragm penetration by rib fracture fragments are the mechanisms of diaphragmatic injury. Blunt trauma to the abdomen increases the transdiaphragmatic pressure gradient between the abdominal compartment and thorax.6 Traumatic diaphragmatic hernia is a frequently missed diagnosis. There is often an interval between trauma and diagnosis.7 This delay has been reported to be > 10 y after the traumatic event.8 This can be explained by various hypotheses. The most likely explanation is that the diaphragmatic defect occurring with injury manifests only when herniation occurs.9 Delayed rupture may occur several days after the initial injury as a process of inflammation and necrosis of a devitalized diaphragmatic muscle.10,11 Small diaphragmatic tears may enlarge over time, allowing herniation of abdominal organs into the thoracic cavity, which may be another explanation for late diagnosis. Finally, in patients receiving mechanical ventilation with PEEP, positive intrathoracic pressure counterpoises intra-abdominal pressure, and only extubation precipitates the phenomenon of a diaphragmatic hernia.9
Grimes12 described the 3 phases of diaphragmatic rupture. The acute phase begins with the original trauma and ends with recovery from other injuries. During this phase, the diaphragmatic injury may be masked. Sixty percent of patients have nonspecific pain in the chest and left upper quadrant. Others may develop acute symptoms of dyspnea, hypotension, and cyanosis. The delayed (latent) phase is associated with transient herniation of the viscera and symptoms of COPD. Patients often present with nonspecific symptoms and may complain of chest and abdominal pain, dyspnea, tachypnea, cough, and vomiting. Finally, the obstructive phase may occur at any time when bowel obstruction occurs. The predominant manifestations are obstruction and strangulation, which may lead to necrosis and rupture if diagnosis and treatment are further delayed.12
Imaging plays a crucial role in diagnosis. Chest x-ray may demonstrate an elevated hemidiaphragm, distortion of the diaphragmatic margin, visceral content in the thorax, loculated left pneumothorax, mediastinal shift, and fracture of left lower ribs, and when a nasogastric tube is in place, it can be seen in the thorax. The sensitivity of chest radiographs is 46% for left-sided ruptures and 17% for right-sided ruptures.13
A chest CT scan has 61–71% sensitivity and 87–100% specificity for acute traumatic diaphragmatic ruptures.14 A spiral CT scan with the use of multiple detectors (4 and 16 detectors) has proven to be superior compared with conventional CT scans. Coronal and sagittal reformatted images are recommended, especially for diaphragmatic tear recognition.15 Diaphragmatic rupture can be diagnosed with CT by the presence of: direct visualization of injury, segmental diaphragm non-visualization, intrathoracic herniation of viscera, peridiaphragmatic active contrast extravasation, the collar sign (a waist-like diaphragmatic constriction of herniated organs), and the positive dependent viscera sign (the herniated viscera [bowel or solid organs] are no longer supported posteriorly by the injured diaphragm and fall to a dependent position against the posterior ribs upon CT examination).14,16 The CT collar sign has a reported low sensitivity (67% for left-sided ruptures and 50% for right-sided injuries) but a specificity of 100%.
The surgical approach to repair acute diaphragmatic injury or rupture depends on the mechanism of injury and the time of presentation. The transabdominal approach is indicated in acute settings in which concomitant abdominal injuries are known or possible. However, when patients with diaphragmatic rupture present in a delayed fashion, a posterolateral thoracotomy is the preferable approach. This provides excellent exposure and the advantage of facilitating the surgical release of adhesion between the herniated organ and lung parenchyma. A thoracotomy is preferred for all right-sided diaphragmatic defects, regardless of the timing of initial injury.17,18
Teaching Points
A high clinical index of suspicion and past history are the key factors for diagnosis and effective management of diaphragmatic ruptures.
Delayed diagnosis can be catastrophic because diaphragmatic defects do not heal and can eventually lead to visceral herniation.
Chest x-ray demonstrating a left-sided cavity with air-fluid level or loculated pneumothorax requires further investigation in patients with a past history of multi-trauma; insertion of a chest tube does not change the radiographic image.
Diaphragmatic rupture may be masked in patients on mechanical ventilation with PEEP.
Footnotes
- Correspondence: Charilaos-Panagiotis C Koutsogiannidis MD, Cardiothoracic Surgery Department, General Hospital G Papanikolaou, Exohi, 57010 Thessaloniki, Greece. E-mail: harisdoc76{at}yahoo.gr.
The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}