

Abstract
BACKGROUND: Measuring diffusing capacity of the lung for carbon monoxide (DLCO) is complex and associated with wide intra- and inter-laboratory variability. Increased DLCO variability may have important clinical consequences. The objective of the study was to assess instrument performance across hospital pulmonary function testing laboratories using a DLCO simulator that produces precise and repeatable DLCO values.
METHODS: DLCO instruments were tested with CO gas concentrations representing medium and high range DLCO values. The absolute difference between observed and target DLCO value was used to determine measurement accuracy; accuracy was defined as an average deviation from the target value of < 2.0 mL/min/mm Hg. Accuracy of inspired volume measurement and gas sensors were also determined.
RESULTS: Twenty-three instruments were tested across 3 healthcare systems. The mean absolute deviation from the target value was 1.80 mL/min/mm Hg (range 0.24–4.23) with 10 of 23 instruments (43%) being inaccurate. High volume laboratories performed better than low volume laboratories, although the difference was not significant. There was no significant difference among the instruments by manufacturers. Inspired volume was not accurate in 48% of devices; mean absolute deviation from target value was 3.7%. Instrument gas analyzers performed adequately in all instruments.
CONCLUSIONS: DLCO instrument accuracy was unacceptable in 43% of devices. Instrument inaccuracy can be primarily attributed to errors in inspired volume measurement and not gas analyzer performance. DLCO instrument performance may be improved by regular testing with a simulator. Caution should be used when comparing DLCO results reported from different laboratories.
Introduction
The single-breath diffusing capacity of the lung for carbon monoxide (DLCO) is a common and clinically useful test providing a quantitative measure of gas transfer in the lungs. It is important for diagnosing and managing patients with respiratory disease and monitoring those exposed to drugs and toxins.1–5 Because clinical decisions are made based on absolute values and changes in DLCO, it is important to minimize intra-laboratory and inter-laboratory variability in test measurement. DLCO test variability can be attributed to both technical (instrument, technician, test gases) and biological factors.6,7 Significant intra-laboratory variability has been primarily attributed to inaccuracy of gas or volume measurement with variations in temperature, barometric pressure, and breath-hold time contributing less to measurement inaccuracy.6,8–11 Significant inter-laboratory variability in DLCO measurement has been reported and attributed to differences in devices, software, test gases, and testing procedure.6,7,9,12,13 This study was designed to assess DLCO instrument performance and quantify inter-laboratory variability in DLCO measurement in Utah and southern Idaho. Our hypothesis was that inter-laboratory variability is large and that poorly performing instruments could be identified using a DLCO simulator (Hans Rudolph, Inc, Kansas City, Missouri) that are not identified with use of standard laboratory quality control measures. Some of these results have been published in abstract form.14
QUICK LOOK
Current knowledge
The single-breath diffusing capacity for carbon monoxide (DLCO) is a common useful test providing a quantitative measure of gas transfer in the lungs. It is important for diagnosing and managing patients with respiratory disease and monitoring those exposed to drugs and toxins. Because clinical decisions are made based on absolute values, it is important to minimize intra-laboratory and inter-laboratory variability in test measurement.
What this paper contributes to our knowledge
DLCO instrument accuracy was unacceptable in 43% of tested devices. Instrument inaccuracy was primarily due to errors in inspired volume measurement, not gas analyzer performance. DLCO instrument performance may be improved by regular testing with a simulator. Caution should be used when comparing DLCO results reported from different laboratories.
Methods
We tested 23 DLCO devices in 15 hospital-based pulmonary function testing (PFT) laboratories in Utah (22 instruments) and southern Idaho (1 instrument) using the same simulator over an 18-month period from 2009 to 2011; all measurements were made by 2 experienced technicians. The PFT laboratories were operated by 3 separate health systems (Intermountain Healthcare, University of Utah Health Systems, and Veterans Administration). The instrument manufacturers were: SensorMedics/Viasys/Carefusion Healthcare (Yorba Linda, California) for 13 devices, Collins/nSpire (Louisville, Kentucky) for 8 devices, and Medgraphics (Saint Paul, Minnesota) for 2 devices.
All instruments were maintained according to manufacturer instructions and calibrated according to manufacturer specifications on test days. Quality control measures used by the laboratories varied, but all included regular bio-control testing. Bio-control testing procedures were not standardized in most laboratories.
Simulator Testing
All DLCO simulations were performed using a single-breath DLCO simulator (Hans Rudolph) as previously described.7 Previous reports indicate the simulator produces a precise and highly repeatable DLCO value in any instrument. The DLCO simulator utilizes 2 precision syringes containing precision gases with 2 concentrations of CO and tracer gas (methane, helium, or neon). For each simulation, a syringe is used to manually withdraw (inhale) a precise volume (VI = 4.5 L) of gas from the DLCO instrument. After approximately 10 s, the second syringe is used to manually inject (exhale) the precision test gas mixture into the PFT instrument. The target DLCO value is then calculated using the EasyLab QC software provided with the simulator, while accounting for the breath-hold time, ambient temperature, and barometric pressure, using the following formula7:
 [1] in which CorrVI (corrected inhaled volume) is the measured VI minus instrument dead space, PB-47 is the barometric pressure minus water vapor pressure (saturated at 37°C), FITR is the inspired tracer concentration, and FETR is the expired tracer concentration, t is the breath-hold time (recorded for each measurement), 60/t adjusts the breath-hold time from seconds to minutes, STPD is the factor converting DLCO to standard temperature and pressure dry (STPD) conditions, FICO is the inspired CO concentration, and FECO is the expired CO concentration.
[1] in which CorrVI (corrected inhaled volume) is the measured VI minus instrument dead space, PB-47 is the barometric pressure minus water vapor pressure (saturated at 37°C), FITR is the inspired tracer concentration, and FETR is the expired tracer concentration, t is the breath-hold time (recorded for each measurement), 60/t adjusts the breath-hold time from seconds to minutes, STPD is the factor converting DLCO to standard temperature and pressure dry (STPD) conditions, FICO is the inspired CO concentration, and FECO is the expired CO concentration.
The CO and tracer gas concentrations used corresponded to a DLCO target of approximately 34 mL/min/mm Hg and 45 mL/min/mm Hg. Four simulations were performed at each gas concentration (8 total for each instrument); the first simulation from each gas concentration for an instrument was discarded to assure that each instrument system had been completely flushed.
Statistical Analysis
The absolute difference between the observed and calculated target DLCO value was used as the measure of accuracy. The 3 differences for each instrument were averaged, and unacceptable instrument accuracy was defined as an average difference greater than 2.0 mL/min/mm Hg from the target.7 VI accuracy was also measured by determining the absolute percent error for each device. Average volume measurement percent errors greater than 3.5% were considered unacceptable.15 Accuracy of device gas sensors were assessed for carbon monoxide (CO) and inert gas (methane, helium, or neon) by measuring absolute percent error. Gas measurement errors exceeding 10% on average were considered unacceptable. Device reproducibility was assessed by determining the SD of the raw differences between each measured DLCO value and the target value from each individual simulation and the raw percent errors for VI, CO, and inert gas. The SD was calculated for all instruments, by hospital PFT laboratory volume and by manufacturer. High volume laboratories were defined as performing more than 20 DLCO tests per week. Chi-square tests for equality of proportions were used to compare the proportions of acceptable and unacceptable instruments by hospital volume and instrument manufacturer.
Results
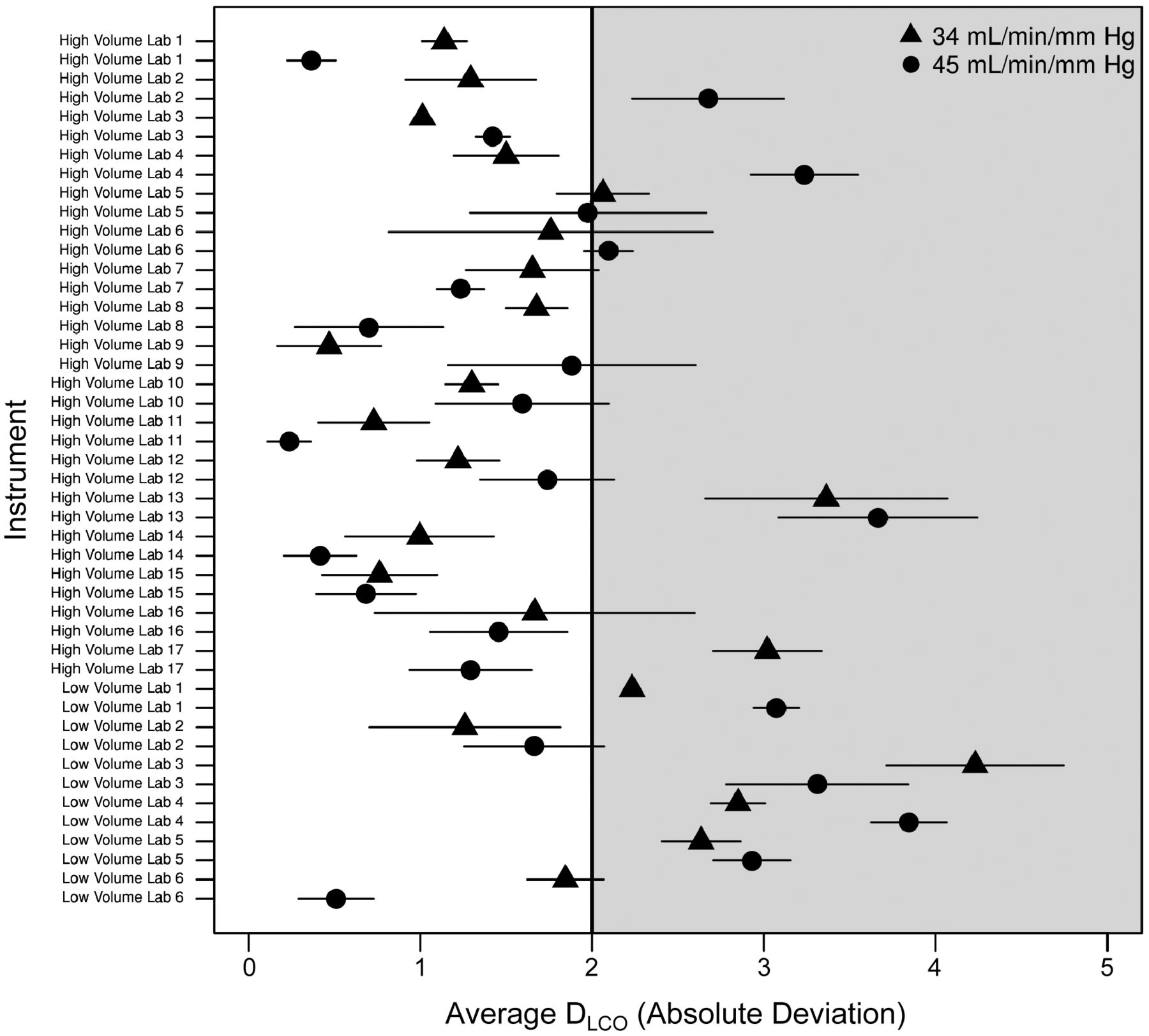
Twenty-three DLCO instruments were tested in 15 hospital-based PFT laboratories across 3 separate healthcare systems. The instruments tested encompassed approximately 60% of all those in hospital-based PFT laboratories in Utah. Overall, 10 of 23 devices (43%) failed to meet the standard for accuracy established for this study (average absolute deviation from one or both target values greater than 2.0 mL/min/mm Hg) (Fig. 1). For the 23 devices tested, the mean absolute deviation from the medium target value (approximately 34 mL/min/mm Hg) was 1.77 mL/min/mm Hg (range 0.47–4.23; SD 0.93) and the mean absolute deviation from the high target value (approximately 45 mL/min/mm Hg) was 1.83 mL/min/mm Hg (range 0.24–3.85; SD 1.11). Five devices failed to accurately measure both the medium and high target values, 3 devices failed in measurement of the high target value only, and 2 devices inaccurately measured only the medium target value. Most of the inaccurate instruments underestimated the target value (8 of 10 inaccurate devices). High volume laboratories performed better than low volume laboratories with 11 of 17 (65%) devices from high volume laboratories meeting the accuracy standards compared with 2 of 6 (33%) devices from low volume laboratories. The difference in proportions was not statistically significant (P = .39), although this may be attributable to the small sample size. The proportion of devices achieving accurate results was not significantly different by manufacturer (P = .33). However, the small numbers of instruments from some manufacturers precluded a conclusive determination of whether there was a significant difference in accuracy between manufacturers.

The mean absolute deviation from the 2 DLCO target values is listed by instrument. Error bars represent standard error of mean. Acceptable accuracy is defined as a deviation < 2.0 mL/min/mm Hg. The gray shaded area shows unacceptable deviation.
Overall, inspired volume (VI) measurement did not meet accuracy criteria: 11 of 23 devices (48%) had an average absolute percent error greater than 3.5%. The mean absolute percent error for VI measurement for all machines was 3.69% (range 0.17–15.78; SD 3.24) (Fig. 2).

The mean absolute percent error in inhaled volume (VI) measurement is listed by instrument. Bars represent standard error of mean. Acceptable accuracy is defined an error < 3.5%. The gray shaded area shows unacceptable deviation.
The instrument gas analyzers performed adequately. All instruments had average CO measurements within 10% of the target value, with a mean absolute percent of 3.26% (range 0.33–8.37; SD 2.10) (Fig. 3). Average inert gas measurements were also acceptable with a mean absolute percent error of 1.52% (range 0.17–5.50; SD 1.28).

The mean absolute percent error in CO measurement is listed by instrument. Bars represent standard error of mean. Acceptable accuracy is defined as an error < 10%. The gray shaded area shows unacceptable deviation.
Device reproducibility, determined using actual differences between measured and target values for each measurement and expressed in SD, is listed in Table 1. The instruments were less variable at the high target values for all test parameters. Variability among the high and low volume laboratories and manufacturers was not consistent across the measured parameters.
Standard Deviation for DLCO Test Parameters
Discussion
This is the first study, to our knowledge, to test DLCO instrument accuracy in clinical pulmonary function laboratories across a geographic region. Consistency of test measurement across a geographic area is clinically relevant, as patients are often evaluated at different hospitals in the same region. The important findings of this hospital-based PFT laboratory quality control study of DLCO instruments were as follows: (1) 43% of devices did not meet our accuracy criteria for DLCO measurement (within 2.0 mL/min/kg of target value), with the largest absolute errors exceeding 4.0 mL/min/mm Hg; (2) high volume laboratories generally performed better than low volume laboratories, although the difference was not statistically significant; (3) gas analyzers for CO and inert gas measurements performed adequately; and (4) device pneumotachographs generally performed poorly; 48% did not accurately measure VI. All instruments tested were maintained and calibrated according to the manufacturer's specifications, and the laboratories routinely performed bio-control testing. However, bio-control testing was not well standardized in most laboratories, and there was often a lack of consistent personnel to serve as bio-controls. This suggests that routine quality control measures are not adequate for many pulmonary function laboratories, and routine testing with a DLCO simulator will identify poorly performing instruments and likely improve laboratory performance. Our findings reinforce the caution that care should be taken in comparing DLCO results obtained in different laboratories.
Prior studies have addressed DLCO accuracy using the same DLCO simulator employed in the present study. Jensen et al7 measured mean absolute accuracy of 5 DLCO instruments, from different manufacturers, tested over 90 d, and reported that the mean deviation from the target DLCO ranged from 1.0 to 4.0 mL/min/mm Hg. Jensen et al9 also tested 125 DLCO instruments involved in a multi-center international inhaled insulin trial using the same DLCO simulator as used in the present study. That study found that 25% of laboratories failed initial testing (mean absolute deviation from target value 1.54 mL/min/mm Hg); instrument failure was defined as a deviation from target value of greater than 3.0 mL/min/mm Hg. We defined instrument failure as a deviation from target value of greater than 2.0 mL/min/mm Hg, based on a large clinical PFT laboratory study that found that 91% of subjects had an absolute difference of < 2.0 mL/min/mm Hg between 2 DLCO measurements.16 In our study, the overall mean deviation from the 2 target values was 1.80 mL/min/mm Hg.
Variability in DLCO measurement can be due to both technical (instrument, testing procedure, instrument gases) and biological/patient factors.12 Technical sources of variability need to be minimized, both because they contribute more to overall DLCO testing inaccuracy and because they are more readily controlled than biological/patient factors. Jensen et al6 assessed DLCO instrument accuracy and variability using normal subjects and a DLCO simulator over 3 months and reported that variability was primarily due to the instrument and that there were significant differences between manufacturers. DLCO instrument inaccuracy can be due to multiple factors. The main sources of error are inaccurate measurements of VI, CO gas concentration and inert gas concentration (see Equation 1 above). Inaccurate CO gas analysis, often attributed to non-linearity of CO analyzers, was thought to be the main source of error in measurement of DLCO.12 In our study, the largest source of error was attributable to inaccurate measurement of VI (mean absolute error of 3.69%) rather than inaccuracy in CO gas analysis (mean absolute percent error of 3.26%). Inhaled volume accuracy needs to be closely monitored with daily 3-L syringe testing, and poorly performing pneumotachographs need to be replaced. The inert gas analyzers performed well (mean absolute percent error of 1.52%). Another potential source of inaccuracy results from errors in instrument gas concentration (FICO and FITR in Equation 1). Instrument gases were either locally provided or obtained from the manufacturer and are required to be accurate to within 2.0% of stated concentration. However, some laboratories used gravimetrically mixed test gases that are accurate to within 1.0%. Although we did not test instrument gases for accuracy, it is not likely that they were a source of significant error.
Simulator testing only assesses technical sources of variability due to the DLCO instrument. It does not assess variability due to the technician or biological/patient factors. Large errors can be observed if the technician does not allow adequate washout of the dead space or if gas leaks in the system are not identified. Biological/patient sources of error can include a failure to inhale to total lung capacity, prolonged inhalation or exhalation time, maintaining airway pressure during the breath-hold that is significantly higher or lower than atmospheric pressure, leaks at the mouth or nose or cough during testing, and failing to correct for variations in hemoglobin level or elevated carboxyhemoglobin. Small variations in temperature and barometric pressure observed during testing have minimal effects on accuracy.9
It is important to minimize inaccuracy and variability in DLCO testing so changes due to disease process or changes due to therapeutic interventions can be detected. The clinical utility of DLCO measurement will be enhanced by maintaining accurate instruments. The magnitude of some of the errors in DLCO measurement observed in this study was clinically important. Inaccurate DLCO measurement may affect clinical management in a variety of clinical settings including idiopathic pulmonary fibrosis,17 lung cancer,3 patients being monitored for drug-induced pulmonary toxicity,2,18 and sarcoidosis.19,20
Conclusions
Our results confirm that inter-laboratory variability in DLCO testing is large and that simulator testing can detect instruments performing poorly beyond those that can be identified with standard PFT laboratory quality control measures. More importantly, this study re-emphasizes the need for caution when comparing DLCO measurements made in different laboratories.
Footnotes
- Correspondence: Matthew J Hegewald MD, Pulmonary and Critical Care Medicine, Intermountain Medical Center, 5132 South Intermountain Drive, Murray, UT 84157. E-mail: matt.hegewald{at}imail.org.
Dr Hegewald presented this work in abstract form at the American Thoracic Society International Conference, held May 13–18, 2011, in Denver, Colorado.
Dr Hegewald has been on the speaker's bureau for Forest Laboratories and Janssen Pharmaceuticals. Dr Jensen has received royalties from Hans Rudolph, Inc. All other authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}