

Abstract
BACKGROUND: Oxidative damage is a major contributing factor to carcinogenesis and obstructive disorders in lungs. Current evidence suggests that the inflammatory processes yield to oxidative mechanisms, which underlie COPD, lung cancer, and obstructive sleep apnea syndrome (OSAS). This study aimed to evaluate the oxidative damage in these diseases by evaluating the oxidative and antioxidant biomarkers.
METHODS: Malondialdehyde, 8-oxo-7,8-dihydro-2′-deoxyguanosine, and coenzyme Q10 levels were evaluated in the blood samples of subjects with COPD, lung cancer, and OSAS by high-pressure liquid chromatography.
RESULTS: A total of 111 participants (35 females, 76 males) with OSAS (n = 29), COPD (n = 26), and lung cancer (n = 28) and healthy controls (n = 28) were included in the study. The malondialdehyde and coenzyme Q10 levels were significantly higher in all 3 diseases when compared with controls (P < .01), whereas 8-oxo-7,8-dihydro-2′-deoxyguanosine levels were only significantly higher than in healthy controls in subjects with lung cancer (P = .005). The highest levels of malondialdehyde and coenzyme Q10 were determined in subjects with OSAS and lung cancer, respectively. The highest 8-oxo-7,8-dihydro-2′-deoxyguanosine levels were also observed in subjects with lung cancer, but the differences of this biomarker with other diagnoses were not statistically significant (P = .56).
CONCLUSION: Oxidative damage was observed in all 3 diagnoses, and, as a response to oxidative stress, antioxidant mechanisms were also active in these diseases. Malondialdehyde and 8-oxo-7,8-dihydro-2′-deoxyguanosine were found to be efficiently usable in the evaluation of oxidative damage in chronic respiratory diseases. (ClinicalTrials.gov registration NCT02406053.)
- malondialdehyde
- 8-oxo-7,8-dihydro-2′-deoxyguanosine
- coenzyme Q10
- COPD
- OSAS
- lung cancer
- oxidative damage
- antioxidants
Introduction
The lung is a particularly important organ because of its interface with the environment. The environmental pollutants and endogenous reactive oxygen species (ROS) from inflammatory cells exert substantial pathological effects on the lung cells.1 Oxidative stress is a major factor that plays a significant role in lung cancer,2 COPD,3 and obstructive sleep apnea syndrome (OSAS).4,5 The current evidence suggests that oxidative stress takes part in the mechanisms involved in the initiation, promotion, and progression of respiratory diseases. The major exposures that cause oxidative stress can be summarized as smoking and ambient air pollution that contains particulate matter smaller than an aerodynamic diameter of 2.5 μm.6–8 Epidemiological and clinical studies showed that the overall outcome of pulmonary oxidative stress increased mortality due to increased incidence of respiratory diseases.9
In OSAS, an episodic hypoxia-reoxygenation cycle occurs during intermittent nocturnal hypoxias that causes the production of ROS.10 These metabolites are responsible for the activation of inflammatory cells in OSAS,11,12 and their increased levels eventually cause ischemia-reperfusion injury13 and cellular and DNA damage.14,15 The latter is also a significant contributor of lung cancer progression. The DNA damage in the presence of ROS yields carcinogenesis by several mechanisms. Some of them are single- or double-stranded DNA breaks and modifications in purines or pyrimidines. Nevertheless, oxidative stress is not the only susceptibility factor for carcinogenesis; there are also many other pathological mechanisms contributing to cancer development, such as reactive nitrogen species and involvement of mitochondrial DNA mutations16 in inflammatory conditions. Previous studies reported that lung cancer occurs more frequently in subjects with moderate to severe COPD.17,18 Oxidative stress is also the main etiological factor of COPD, which is particularly important in the exacerbations of the disease.19 The parenchymal damage in COPD includes some mechanisms, such as chronic inflammation, oxidative stress, deteriorations in the balance of protease and antiprotease activities, and apoptosis.20 The major etiological factor suspected to play a role in the progression of lung cancer in COPD is reported as chronic inflammation, which causes induction of several interleukins and cyclooxygenase-2 activity. The inflammatory microenvironment is a potential medium to contribute to the neoproliferative process, which interacts with regulatory mechanisms, such as apoptosis and angiogenesis.21
Some biomarkers are available for evaluating the oxidative stress in living organisms.22 Some of these biomarkers are malondialdehyde, 8-oxo-7,8-dihydro-2′-deoxyguanosine, and coenzyme Q10. Each of these biomarkers is involved in oxidative processes. Malondialdehyde is a by-product of polyunsaturated fatty acid peroxidation.23 Lipid peroxidation is the oxidation reaction between ROS and polyunsaturated fatty acids, which eventually causes changes in the structure and permeability of the lung membrane.24 The second biomarker, 8-oxo-7,8-dihydro-2′-deoxyguanosine, is primarily involved in DNA damage. The mechanism for this damage is the guanine:cytosine to adenine:thymine transversion on DNA replication,25 which induces microsatellite instability and abnormal apoptosis or necrosis.26 The third biomarker is coenzyme Q10, which is also a mediator of lipid peroxidation and an essential cofactor in the electron transport chain. It is also a lipophilic antioxidant component of the lipid membranes.27 In this study, we measured and compared the levels of malondialdehyde, 8-oxo-7,8-dihydro-2′-deoxyguanosine, and coenzyme Q10 in different pulmonary diseases to evaluate the oxidative damage in chronic pulmonary diseases.
QUICK LOOK
Current knowledge
Environmental pollutants and endogenous reactive oxygen species from inflammatory cells exert substantial pathological effects on the lung. Oxidative stress plays a significant role in lung cancer, COPD, and obstructive sleep apnea syndrome (OSAS). The major exposures that cause oxidative stress are smoking and air pollution.
What this paper contributes to our knowledge
Biomarkers of oxidative stress in lung cancer, obstructive sleep apnea, and COPD were significantly higher compared with normal controls. The highest levels of oxidative stress were seen in lung cancer. Levels of 8-oxo-7,8-dihydro-2′-deoxyguanosine were elevated in subjects with cancer but not in the other 2 groups.
Methods
This is a prospective study, conducted in the Pulmonology Department of the Faculty of Medicine of Yuzuncu Yil University Hospital between January 2014 and July 2014. A total of 111 participants (35 females, 76 males) with OSAS (n = 29), COPD (n = 26), and lung cancer (n = 28) and healthy controls (n = 28) were included in the study.
The COPD diagnosis was based on spirometry that was performed previously during the stable period of the disease using Global Initiative for Chronic Obstructive Lung Disease criteria.28 The study included subjects with moderate to severe COPD, with FEV1 >30% and <80%, who were clinically stable and under adequate treatment for the degree of illness.
Subjects suspected clinically of having OSAS were examined and underwent standard overnight polysomnography in the Sleep Unit of the Pulmonary Medicine Department of our Yuzuncu Yil University. Sleep stages and respiratory parameters were scored according to the standard criteria of the American Academy of Sleep Medicine.29 Untreated OSAS subjects who had a higher apnea-hypopnea index, >15/h, were included in the study.
The diagnosis of lung cancer was based on the analysis of biopsy or cytologic specimens obtained by bronchoscopic examination, transthoracic biopsy, or surgery. The subjects who had not had chemotherapy and/or radiotherapy were included in the study. Cardiovascular disease, hypertension, diabetes mellitus, inflammatory or infectious conditions were exclusion criteria for COPD, OSAS and lung cancer. Twenty-eight healthy controls were without a history of chronic or recurrent disease and had normal physical examination results. The study was conducted according to the Declaration of Helsinki and approved by the Ethics Committee of the Yuzuncu Yil University School of Medicine. Blood samples were obtained from the subjects. The samples were centrifuged at 3000 rpm for 5 minutes and stored at −80°C until analysis.
8-Oxo-7,8-Dihydro-2′-Deoxyguanosine
The blood samples were treated with a DNA isolation kit before the hydrolysis procedure. After that, 0.5 mL of 60% formic acid was added to the 1 mL of obtained mixture. After waiting for them to cool down, the tubes were kept at room temperature to eliminate the formic acid. Then approximately 1 mL of mixture was preserved at −20°C.
High-Pressure Liquid Chromatography Analyses
8-Oxo-7,8-dihydro-2′-deoxyguanosine levels were obtained in predetermined systems by high-pressure liquid chromatography under various wavelengths and by high-pressure liquid chromatography UV and electron capture detection. Before the high-pressure liquid chromatography analyses, hydrolyzed DNA samples were melted in high-pressure liquid chromatography eluent. The final volume was 1 mL and 20 μl of final hydrolyzing high-pressure liquid chromatography-electron capture detection (Agilent 1200 modular system [Agilent Technologies, Santa Clara, California] and Waters 2456 electron capture detector [Waters, Eschborn, Germany]): column, reverse-phase C18 analytic column (250 mm × 4.6 mm × 4.0 μm; Phenomenex, Torrance, California). Mobile phase consisted of acetonitrile (97:3, v/v) containing a 0.05 M potassium phosphate (pH 5.5) tampon with a 1-mL/min flow rate. dG concentration was determined by measuring its absorbance <245 nm and by the 8-oxo-7,8-dihydro-2′-deoxyguanosine electrochemical reading (600 mV). Amounts of deoxyguanosine and 8-oxo-7,8-dihydro-2′-deoxyguanosine were determined by Sigma and 8-oxo-7,8-dihydro-2′-deoxyguanosine standards. DNA damage was presented as 8-oxo-7,8-dihydro-2′-deoxyguanosine/deoxyguanosine × 105.30,31
Coenzyme Q10
Ubiquinol-10 and ubiquinone-10 analyses were performed according to Mosca et al.33 50 μL of 1–4 benzoquinone (2 mg/mL) was added to a 200-μL serum sample and mixed for 10 s by vortex. After incubating for 10 min at room temperature, 1 mL of n-propanol was added. After 2 min of centrifugation at 1,000 rpm, 200 μL of supernatant was used in a high-pressure liquid chromatography-UV system. The UV detector was set to 275 nm, and the flow rate was set to 1 mL/min. A 65:35 ethanol/methanol mixture was used as the mobile phase, and a Supelcosil LC 18 column (Supelco, Bellefonte, Pennsylvania) (25 × 0.46 cm inner diameter, 5 μm) was used as the column. Results were presented as ubiquinol-10/ubiquinone-10.32,33
Malondialdehyde
Serum malondialdehyde analysis was performed by high-pressure liquid chromatography according to Khoschsorur et al.34 Fluorescent detectors were used in the high-pressure liquid chromatography system. 0.44 M H3PO4 and 42 mM thiobarbituric acid were added to 50 μL of serum sample, and the mixture was incubated in boiled water for 30 min. It was immediately cooled down after incubation, and an equal volume of alkaline methyl alcohol was added. The mixture was centrifuged for 3 min at 3,000 × g. The upper layer was separated by a pipe. One hundred μL of supernatant was used in the high-pressure liquid chromatography-fluorescence detection system. Chromatographic conditions were as follows: pressure, 75 ± 10; fluorescence detector, excitation 527 nm and emission 551 nm; flow rate, 0.8 mL/min; mobile phase, methanol plus 50 nM KH2PO4 (40:60, v/v); column, reverse-phase C18 (5 μm, 4.6 × 160 mm, Eclipse VDB-C18, Agilent); injection volume, 20 μL.
Statistical Analyses
Descriptive statistics are presented with frequency and percentage for categorical data and with mean and SD for numerical data. Comparisons between 2 independent groups were conducted with the Mann-Whitney U test and the chi-square test for non-normally distributed numerical and categorical variables, respectively. Multiple-group comparisons were done with the Kruskal-Wallis test, and the Mann-Whitney U test was utilized for post hoc comparisons. A type-1 error level of 5% was considered as statistical significance. Statistical analyses were performed with PASW Statistics (SPSS, Chicago, Illinois).
Results
Age and sex distribution of the study groups are presented in Table 1. The male/female ratios were similar between the study groups (P < .001). The distribution of malondialdehyde, 8-oxo-7,8-dihydro-2′-deoxyguanosine, and coenzyme Q10 levels in the study groups is presented in Table 2.
Distribution of the Demographic Characteristics in Study Groups
Distribution of the Biomarkers in the Study Groups
Malondialdehyde
The highest malondialdehyde levels were observed in subjects with OSAS (6.1 ± 3.5), and the lowest values were in healthy controls (2.9 ± 0.6). The malondialdehyde levels in OSAS were significantly higher than in the remaining groups (P < .01). The levels in COPD and lung cancer were similar (P = .43) and significantly higher than in the control group (P < .01).
8-Oxo-7,8-Dihydro-2′-Deoxyguanosine
The highest 8-oxo-7,8-dihydro-2′-deoxyguanosine levels were observed in subjects with lung cancer, where it was significantly higher than in the controls (P = .01). No other significant differences between the remaining groups were observed for the 8-oxo-7,8-dihydro-2′-deoxyguanosine levels (P = .56).
Coenzyme Q10
The coenzyme Q10 levels in subjects with lung cancer was significantly higher than in the healthy controls (P < .01). The subjects with OSAS and COPD were similar for coenzyme Q10 levels (P = .21). The distribution of the levels of these biomarkers is presented in Figure 1.
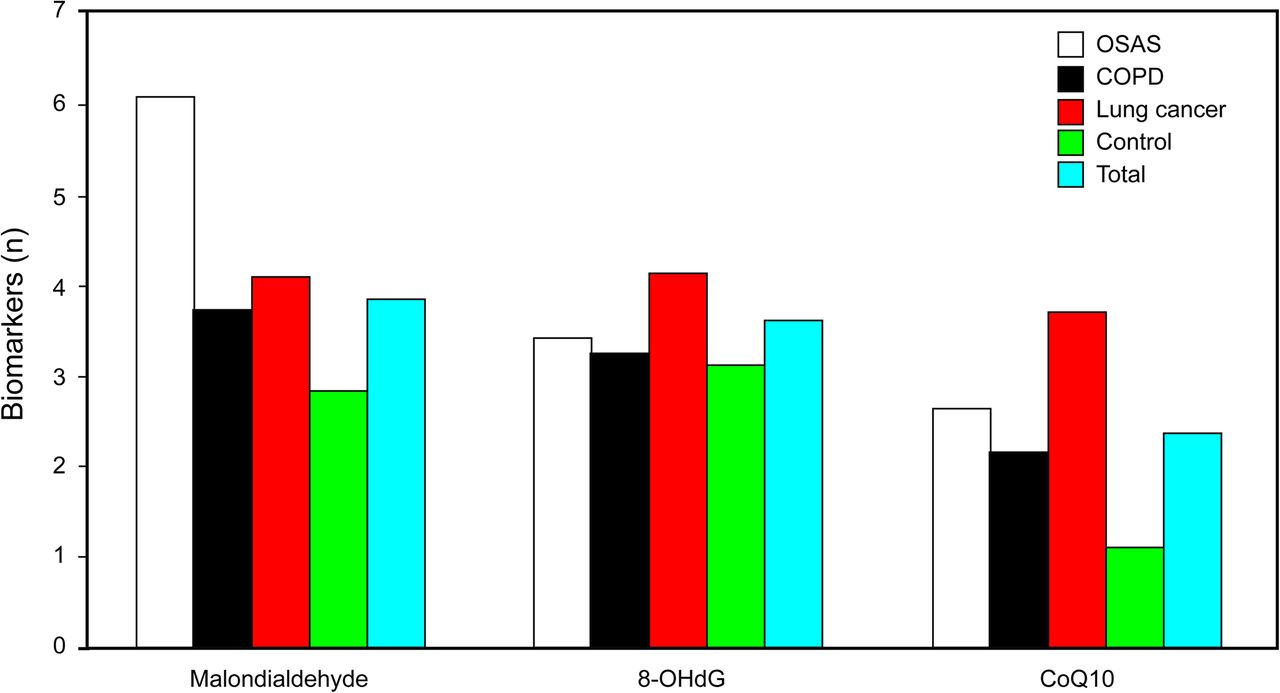
Distribution of biomarkers in the study groups. OSAS = obstructive sleep apnea syndrome.
Discussion
This study evaluated the biomarkers of oxidative stress in selected respiratory diseases and carcinogenesis. The levels of malondialdehyde, 8-oxo-7,8-dihydro-2′-deoxyguanosine, and coenzyme Q10 were evaluated in the subjects with lung cancer, OSAS, and COPD to determine which of these diseases are more prone to oxidative damage. The malondialdehyde and coenzyme Q10 levels were significantly higher in all 3 diseases when compared with controls, whereas 8-oxo-7,8-dihydro-2′-deoxyguanosine levels were only significantly higher than in healthy controls in the subjects with lung cancer. The highest levels of malondialdehyde and coenzyme Q10 were determined in subjects with OSAS and lung cancer, respectively. The highest 8-oxo-7,8-dihydro-2′-deoxyguanosine levels were also observed in subjects with lung cancer, but the differences of this biomarker with other diagnoses were not statistically significant. Overall, findings of the present study suggest that the oxidative processes play a significant role in OSAS, lung cancer, and COPD.
Oxidative stress appears to be an important factor in various human diseases. Oxidative stress occurs in a cell or tissue when the concentration of ROS generated exceeds the antioxidant capability of that cell.35 Maintenance of steady-state concentrations of ROS is essential for adequate functioning of aerobic organisms. ROS may interact with and modify the cellular protein, lipids, and DNA, resulting in altered target cell function.36 There is considerable evidence that ROS are involved in the pathogenesis of various human diseases.37 Recent studies have shown an important role for ROS in tumor development.36 Studies have also shown that hypoxia has been associated with various stages of tumor formation and progression.38 Our hypothesis suggests that oxidative stress may be a crucial factor in both processes. The causal effects between hypoxia and carcinogenesis remain to be elucidated.
OSAS is regarded as a human-model disease that can be used for measurements of oxidative mechanisms.10 Some previous studies suggested that OSAS is directly or indirectly related to the production of ROS.14,39 The uncertain results obtained in some studies yielded the comment that elevated oxidative stress parameters cannot be determined in subjects with light to severe OSAS, and the most robust biomarker for oxidative processes in this disease is malondialdehyde.10
The end products of the reactions between ROS and polyunsaturated fatty acids are hydroperoxides, and malondialdehyde is one of the major aldehydes produced by the breakdown of such hydroperoxides. The hypoxia-reoxygenation cycles in OSAS were suggested to cause increases in malondialdehyde levels, which was also confirmed by the studies that showed increased malondialdehyde levels following hypoxemia in healthy controls,40 or hyperoxic reoxygenation in surgical subjects.41 Our results also confirm these findings. We observed that malondialdehyde was significantly higher in OSAS when compared with the other diagnoses and may be effectively used for evaluating the oxidative stress in these patients.
Another biomarker that was suggested could be efficiently used for assessment of oxidative DNA damage is 8-oxo-7,8-dihydro-2′-deoxyguanosine, the levels of which we found were not significantly different from those of the healthy controls. This finding was both challenged and replicated in a previous study by Jordan et al.10 They found in their study that urinary 8-oxo-7,8-dihydro-2′-deoxyguanosine levels were significantly correlated with the duration of oxygen desaturation, but hypoxemia followed by reoxygenation was inadequate to produce marked DNA damage, and 8-oxo-7,8-dihydro-2′-deoxyguanosine was found to remain at normal levels. We have also observed that 8-oxo-7,8-dihydro-2′-deoxyguanosine levels in subjects with OSAS were higher than in controls, but this was not statistically significant.
8-Oxo-7,8-dihydro-2′-deoxyguanosine levels were found to be highest in lung cancer in our study; nevertheless, the differences between other diseases were not statistically significant. Recent studies showed that increased levels of oxidative stress were observed in subjects with lung cancer when compared with healthy controls.42 The oxidative stress causes oxidation in the guanine base in DNA, which results in the production of 8-oxo-7,8-dihydro-2′-deoxyguanosine.43 Moreover, guanine base oxidations cause G to T transversion mutations in DNA, which are found in the K-ras oncogene and p53 tumor-suppressor gene of human lung cancer.25,44,45 These findings suggest that oxidative stress plays a role in different steps of carcinogenesis in lungs. However, according to our findings, it is also worthy of mention that 8-oxo-7,8-dihydro-2′-deoxyguanosine represents a widespread oxidative process, which is also effective in the progression of OSAS and COPD.
The antioxidant coenzyme Q10 is an oil-soluble vitamin-like molecule, which is present primarily in the mitochondria and is part of the electron-transport chain. Literature data suggest that its levels are decreased in elderly individuals and in subjects with chronic diseases.46 As a result of its decrease, lipid and protein peroxidation increases. In this regard, the presence of coenzyme Q10 is an important factor in protecting the DNA from oxidative damage. We have observed that the levels of coenzyme Q10 were significantly increased in subjects with OSAS, lung cancer, and COPD when compared with the healthy controls. This finding suggests that the antioxidant mechanisms are activated in these diseases due to increased oxidative stress. However, the highest increase was in subjects with lung cancer, and the differences between lung cancer and the remaining diseases were also statistically significant. This may suggest that the highest oxidative stress is in lung cancer and that coenzyme Q10 has been increased as a response to the oxidative damage.
Coenzyme Q10 is a redox molecule, which can be found in oxidized (ubiquinone) or reduced (ubiquinol) form in the mitochondria. It basically prevents the biological molecules by inhibiting lipid peroxidation.47 The unstable free radicals are stabilized by taking electrons from ubiquinone in the electron-transport chain, which is the antioxidant feature of coenzyme Q10 with great importance.27 Previous studies have reported that coenzyme Q10 levels are significantly decreased in subjects with lung cancer.48 Our results conflict with these findings. This difference may result from the different clinical characteristics of the subjects with lung cancer between the studies, such as stage or underlying comorbidities. But overall, increases in the antioxidant mechanism may be regarded as a balancing response of the organism against oxidant processes.
The present study has several limitations. First, our study findings may have been influenced by confounding factors. Second, this was a single-institution study, and although the patient population was probably comparable with that of many other departments in the same time period, some caution should be taken before generalizing the findings to other settings. Due to these restrictions, associations should be interpreted with caution. However, we hope that this research will pioneer further studies on this method.
Conclusions
When the findings of our study were interpreted into clinical practice, we concluded that the highest level of oxidative stress was observed in lung cancer, which is reflected by the highest level of antioxidant molecule coenzyme Q10 and also by the highest level of 8-oxo-7,8-dihydro-2′-deoxyguanosine in this disease. Malondialdehyde was highest in OSAS, but it was also significantly higher in lung cancer and COPD when compared with controls. Overall, these 3 diagnoses were all related with increased oxidative stress and antioxidant mechanisms in response to oxidative damage.
Footnotes
- Correspondence: Aysel Sunnetcioglu MD, Department of Chest Diseases, Yuzuncu Yil University, Faculty of Medicine, Van, Turkey.
The authors have disclosed no conflicts of interest.
Aysel Sunnetcioglu presented a version of this report as a poster at the 18th Thorax Congress, held April 3, 2015, in Antalya, Turkey.
- Copyright © 2016 by Daedalus Enterprises





{kind=link}