

Abstract
BACKGROUND: Accurately measuring the partial pressure of end-tidal CO2 (PETCO2) in non-intubated patients is problematic due to dilution of expired CO2 at high O2 flows and mask designs that may either cause CO2 rebreathing or inadequately capture expired CO2. We evaluated the performance of 2 capnographic O2 masks (Cap-ONE and OxyMask) against a clinically expedient method using a standard O2 mask with a flow-directed nasal cannula used for capnography (CapnoLine) in a spontaneous breathing model of an adult and child under conditions of normal ventilation, hypoventilation, and hyperventilation.
METHODS: An ASL-5000 simulator was attached to a manikin face with a catheter port, through which various CO2/air mixtures were bled into the ASL-5000 to achieve a PETCO2 of 40, 65, and 30 mm Hg. Both PETCO2 and inspired PCO2 were measured at O2 flows of 5, 10, 15, and 20 L/min (adult model) and 2, 4, 6, 8, and 10 L/min (pediatric model).
RESULTS: PETCO2 decreased to varying degrees as O2 flow increased, depending upon the breathing pattern. Although all devices appeared to perform reasonably well under normal and hyperventilation conditions, the clinically expedient method was associated with substantially more CO2 rebreathing. PETCO2 usually deteriorated more under simulated hypoventilation, regardless of the measurement method.
CONCLUSIONS: Both of the specially designed O2 capnography masks provided reasonably stable PETCO2 without significant CO2 rebreathing at the commonly used O2 flows. Because of their open design, PETCO2 measured at high O2 flows may produce artificially lower readings that may not reflect arterial CO2 levels compared with lower O2 flows.
Introduction
Respiratory pattern assessment and its integration with indices of oxygenation and ventilation adequacy are crucial aspects of patient monitoring during procedural sedation1,2 as well as recovery from general anesthesia.3 Respiratory depression and airway obstruction in these patients occurs frequently4 and represents the leading cause of adverse events.5 Studies using capnography in these patients have found that hypoventilation is common and that abnormal capnometry/capnography generally precedes oxygen desaturation.1,2,6 In one study, hypoventilation preceded oxygen desaturation in approximately 75% of cases by an average of 1.7 min.1
Critically ill, non-intubated patients represent another cohort that may benefit from capnography. However, utilizing capnography in non-intubated patients with respiratory insufficiency presents technical challenges that may interfere with measurement accuracy, including: (1) dilution of expired gas with varying supplemental O2 flows, (2) oxygen mask design, (3) the orientation of capnographic cuvette chamber or sample line in relation to expired gas flow, and (4) variability of the respiratory pattern, including the contributions of nasal versus mouth breathing.
Emblematic of the technical issues for monitoring critically ill patients has been the limitations imposed by sidestream CO2 sampling with a standard nasal cannula. This became readily apparent in obese patients (particularly those with obstructive sleep apnea) because they tend to be mouth breathers. Under these circumstances the partial pressure of end-tidal carbon dioxide (PETCO2) does not reliably reflect the partial pressure of arterial carbon dioxide (PaCO2).3 This problem also occurs in respiratory failure because the elevated work of breathing associated with high levels of minute ventilation (V̇E)7,8 obviates nasal breathing due to the additional resistance. To address this problem, nasal cannulas designed for capnography now incorporate an oral guided design that samples expired gas from the center of the mouth. This modification was found to accurately reflect PaCO2 in subjects recovering from general anesthesia.3 Nonetheless, studies of oral guided nasal cannula capnography in subjects with respiratory distress produced results of uncertain reliability. For example, a clinically reasonable correlation was found between PaCO2 and PETCO2 (r = 0.82), but also there was substantial variability in performance.9 Whereas 38% of the subjects had a PaCO2 − PETCO2 difference within 5 mm Hg, an equal percentage of patients had a difference ≥10 mm Hg.9
There are 2 approaches to designing O2 masks that incorporate capnography. The Cap-ONE (Nihon Kohden, Tokyo, Japan) uses mainstream capnography for its adult and pediatric masks, whereas the OxyMask and OxyKid devices (SouthMedic, Barrie, Canada) use sidestream capnography. These devices open the possibility of accurately monitoring ventilation during acute respiratory insufficiency in patients with elevated V̇E demands, who also require high flow O2 delivery. The objective of this bench study was to assess the stability of PETCO2 measurements as supplemental O2 flow increases. We compared these 2 specially designed masks with a clinically expedient tactic, whereby a standard O2 mask is coupled with an oral guided design nasal cannula (CapnoLine, Medtronic, Minneapolis, Minnesota). These devices were tested in simulated adult and pediatric patients under conditions of normal ventilation, hyperventilation, and hypoventilation, using both low- and high-flow O2 delivery.
QUICK LOOK
Current knowledge
Monitoring the partial pressure of end-tidal CO2 (PETCO2) in non-intubated patients usually is done with specially designed nasal cannulas in the postoperative setting. Its application in patients with acute respiratory failure is more challenging, which has lead to specially designed (open) O2 masks incorporating capnography. These have been shown to cause substantial artifactual decreases in PETCO2 in infant O2 masks, but this has not been studied in pediatric or adult masks.
What this paper contributes to our knowledge
Specially designed (open) O2 masks incorporating capnography generally maintain reasonable PETCO2 readings at commonly used flows. Using a standard O2 mask in concert with flow-directed nasal cannula-based capnography can provide stable PETCO2 measurements but carries a substantial risk of CO2 rebreathing. This risk is related to standard O2 mask design that does not appear to provide adequate CO2 removal at low to moderate flows.
Methods
The design and model construction were done with the assistance of Nihon Kohden representatives; however, final decisions regarding the study protocol were made solely by the authors. The study was conducted entirely at Zuckerberg San Francisco General Hospital (San Francisco, California).
Simulation Model
The simulation model consisted of custom designed adult and pediatric manikin faces with patent oronasal passages. A 16-cm length of 15-mm diameter tubing, with an additional bleed-in port connected the manikin faces to the ASL-5000 lung simulator (IngMar Medical, Pittsburgh, Pennsylvania). A short stylet was used to introduce gas tubing approximately 8 cm into the ASL-5000 (Fig. 1). Blended gases from an E cylinder of CO2 and an H cylinder of compressed air were introduced into the test lung (Fig. 2). The cylinder flow from each was titrated to reach a stable PETCO2, defined as that achieving the target value (±2 mm Hg) for 2 min before the commencement of data collection. The PETCO2 targets were 40, 65, and 30 mm Hg, representing conditions of normal breathing, hypoventilation, and hyperventilation.

Adult mannequin face with connecting tube and hose line for bleeding in compressed air and CO2 gas mixtures to the ASL-5000 piston.
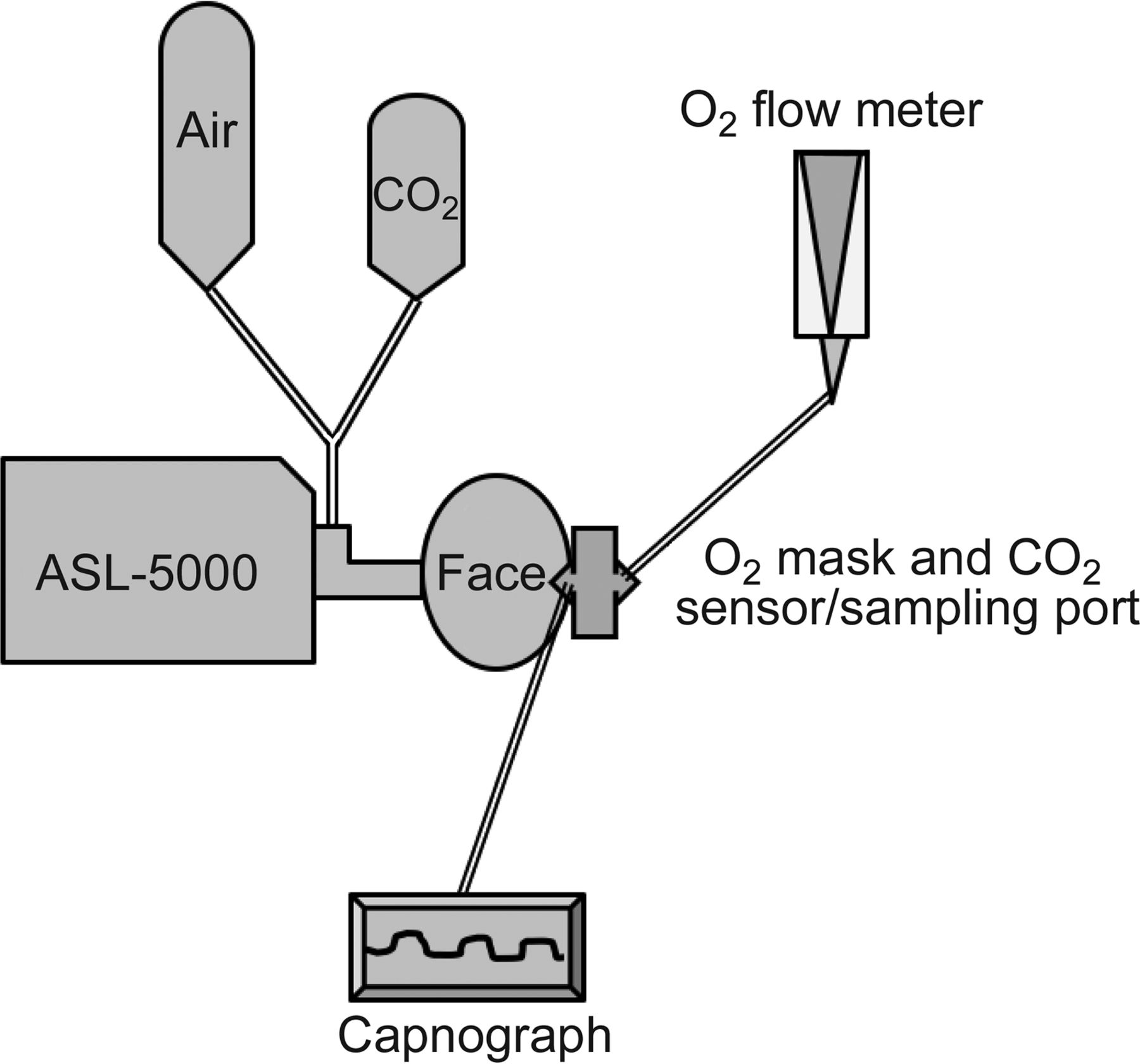
Schematic of simulation design.
Adult and pediatric simulated breathing patterns mimicking these conditions were programmed into the ASL-5000 for a 65-kg adult and a 25-kg child of approximately 7 y of age (Table 1). For the adult, simulated normal ventilation and hypoventilation used the same breathing patterns with different PETCO2 targets. The adult hyperventilation pattern mimicked a rapid-shallow breathing pattern with an increased inspiratory time fraction often observed during labored breathing.7 For pediatric breathing patterns, the frequency was decreased because of difficulty achieving a stable PETCO2 that did not exceed the target of 65 mm Hg. The simulated rapid-shallow breathing pattern also used an elevated inspiratory time fraction.
Breathing Pattern Scenarios and Associated PETCO2 Values
Settings for compliance and resistance on the ASL-5000 in the adult model were 65 mL/cm H2O and 5 cm H2O/L/s, respectively, and settings in the pediatric model were 25 mL/cm H2O and 8 cm H2O/L/s, respectively. The piston volume (analogous to functional residual capacity) was set to a value of 33 mL/kg (2.1 and 0.8 L for adult and pediatric models, respectively).10
Monitoring Devices
The 3 O2 capnograph strategies were tested using 4 monitors. The Cap-ONE adult and pediatric O2 masks were interfaced with the Nihon Kohden Cap-TEN 2800, and the OxyMask was used with the 8400 Capnograph (Smiths Medical, St Paul, Minnesota). In contrast, the adult CapnoLine and pediatric Smart CapnoLine flow-directed nasal cannula/sidestream capnography (Oridion/Medtronic, Minneapolis, Minnesota) devices were each tested using 2 monitors, the Capnostream-20 (Oridion/Medtronic, Minneapolis, Minnesota) and the Philips MX-450 (Philips, Eindhoven, Netherlands), because these sampling lines were designed for use with multiple monitors. Before data collection, the monitors were zeroed, and the gain was evaluated using a calibration tank with either 5 or 10% CO2/balance air (Cal Gas Direct, Huntington Beach, California) to achieve a PCO2 of either 38 or 65 mm Hg.
Both the Cap-Ten 2800 and MX-450 monitors were set to read-out breath-by-breath changes in PCO2 (inspired and end-tidal). Because the Capnostream-20 displays an updated value of PETCO2 every second, the displayed value was considered likely to capture breath-by-breath changes. In contrast, the 8400 only exhibits a 4-breath average. To test the impact of different sampling methods, we compared the results between recording the PETCO2 from every 4th breath with consecutive breaths during extended sampling periods. We found no appreciable difference in results (data not shown).
Two different O2 flow meters were used: For adult conditions, a model 1MFA high-flow capacity O2 flow meter (Precision Medical, North Hampton, Pennsylvania) with a range of 5–70 L/min, and for pediatric conditions, a model 1MFA1001 (Precision Medical, North Hampton, Pennsylvania) flow meter with a range of 0.5–15 L/min was used.
Protocol
Each age-specific device and capnograph was tested under the 3 conditions described above. The baseline PETCO2 was established with the simulated breathing pattern engaged and the mask/capnograph fitted onto the manikin face but without supplemental O2 flow. As mentioned earlier, the gas mixtures were titrated, typically over a 5-min period, to achieve the target PETCO2 that varied no more than ±2 mm Hg for 2 min, after which PETCO2 data from 20 consecutive breaths were recorded.
After the baseline PETCO2 was established for each condition, O2 flow was adjusted in 5-L/min steps between 5 and 20 L/min for each adult test condition and in 2-L/min steps between 2 and 10 L/min for each pediatric test condition. The same PETCO2 stability conditions before beginning data collection were maintained throughout the study.
The Cap-ONE and OxyMask/OxyKid masks differ in design from a standard adult or pediatric O2 mask; namely, they are characterized by a large open surface area to prevent CO2 rebreathing. Therefore, we performed additional baseline testing of all masks using the CapnoLine readings without any masks attached to the manikin face during spontaneous breathing as a reference. We then placed each mask over the manikin face and recorded the change in PETCO2 to assess CO2 rebreathing.
Data Analysis
All data were reported as mean ± SD. Previous experience with lung model testing demonstrated that variables of interest often produce monotonous data, such that the SD has been or has approached zero. In consequence, inferential statistical testing was reserved for comparing PETCO2 values between testing conditions or devices when the coefficient of variation (SD/mean) was >0.05 and the difference between mean values was only 1 mm Hg. Statistical analysis was done with PRISM (GraphPad Software, LaJolla, California) using either unpaired t tests or one-way analysis of variance and Tukey-Kramer post-tests. α was set to .05.
Results
Adult Model
The ability of each monitoring device to maintain a constant PETCO2 varied across testing conditions as supplemental O2 was introduced and then increased. During simulated normal ventilation, the CapnoLine tested with the CAP-20 provided the most stable PETCO2 measurements as O2 flow increased from 5 to 20 L/min (Table 2). However, the other 3 devices also performed well at very high O2 flows. When simulating hypoventilation, the CapnoLine with the CAP-20 provided slightly more stable measurements than the Cap-ONE and the CapnoLine with the MX-450 at the highest O2 flows. With the introduction of O2 flow, there was an exceptionally large initial drop in PETCO2 with the OxyMask (12 mm Hg vs 4–5 mm Hg with the other devices) that made the subsequent changes in PETCO2 as O2 flow increased misleading. In contrast, both the Cap-ONE and OxyMask provided very stable measures of PETCO2 under conditions of simulated hyperventilation.
Comparisons of PETCO2 Between Devices as Supplemental O2 Flow Rate Increases in an Adult Model
More importantly, CO2 rebreathing was a problem when using the CapnoLine with a standard O2 mask compared with the Cap-ONE system. Both in the absence of supplemental O2 and at O2 flows of 5–10 L/min, and under both simulated normal ventilation and hypoventilation conditions, inspired PCO2 was significantly higher with the CapnoLine versus the Cap-ONE system (inspired PCO2 range of 3–10 mm Hg vs 2–3 mm Hg, respectively, P < .001) (Fig. 3, A and B). We were unable to evaluate the OxyMask because the 8400 monitor did not provide inspired PCO2 readings.

Inspired PCO2 as a function of mask design and supplemental O2 flow under simulated normal (A) and hypoventilation conditions (B) in the adult model and also under simulated normal (C) and hypoventilation conditions (D) in the pediatric model.
This explains why we performed additional testing using just the CapnoLine as the reference monitor and compared changes in PETCO2 before and after placing each mask under conditions of simulated normal and hypoventilation. As would be expected, there was little difference in PETCO2 under baseline (mask-off) conditions. Once O2 masks were placed on the manikin face, differences between the closed and open mask designs were readily apparent as the mean PETCO2 increased by 8–9 mm Hg with the simple mask versus 3–4 mm Hg with the Cap-ONE mask and 1–2 mm Hg with the OxyMask (Fig. 4).
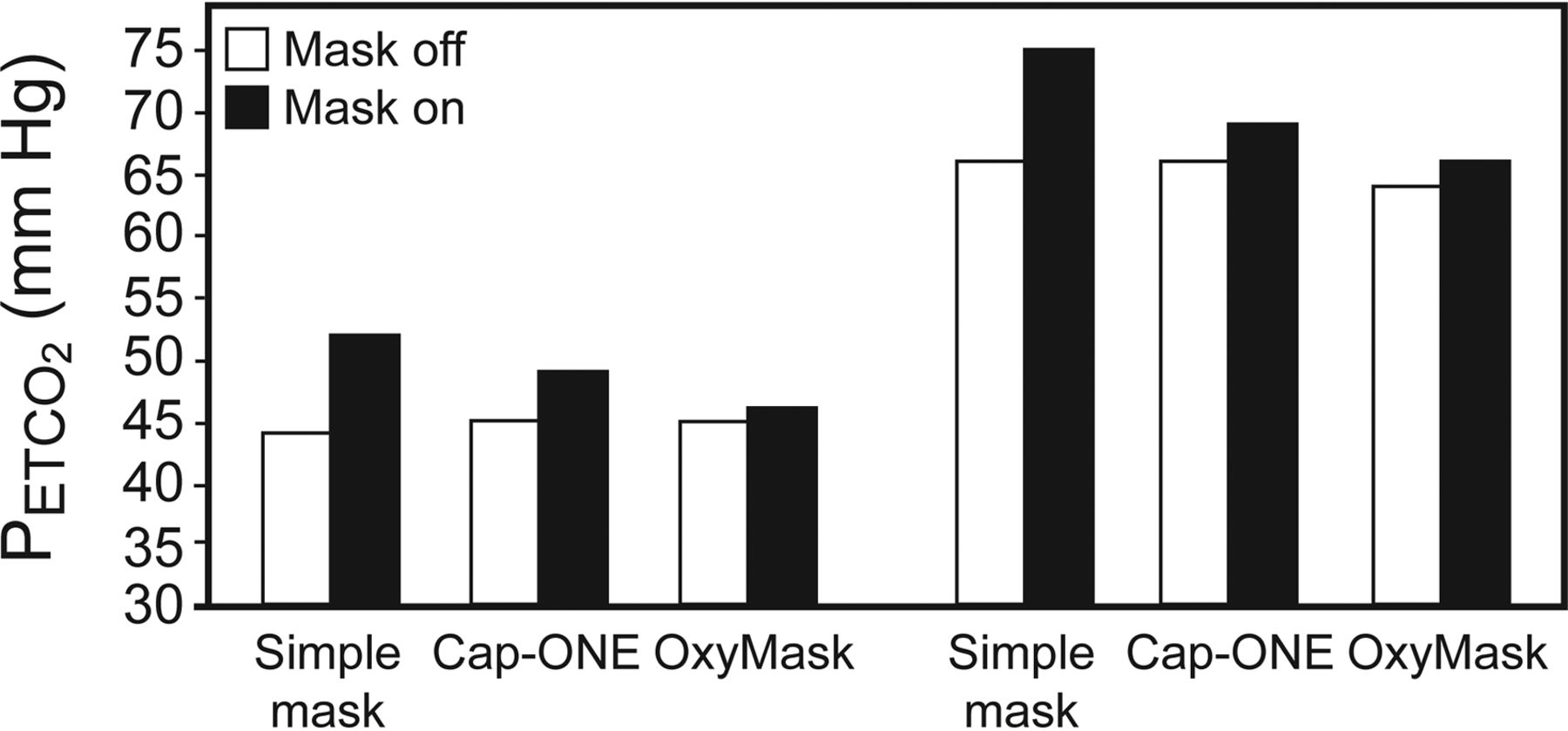
The effect of mask design on PETCO2 under simulated normal and hypoventilation conditions (see text).
In addition, we noted that the performance of the CapnoLine appeared to be highly dependent upon the monitor it was interfaced with because the CAP-20 yielded more stable results than the MX-450 under both simulated normal and hypoventilation conditions, but not during simulated hyperventilation. This occurred despite the fact that both monitors use the same low sampling flow of 50 mL/min.
Pediatric Model
During simulated normal ventilation, the Cap-ONE provided the most stable PETCO2 measurements, with decrements of 3 mm Hg compared with 5–6 mm Hg with the other devices as O2 flow increased from 2 to 10 L/min (Table 3). During simulated hyperventilation, the Cap-ONE, OxyKid, and CapnoLine attached to the MX-450 also demonstrated decrements of only 2–3 mm Hg in PETCO2. Under conditions of simulated hypoventilation, the Cap-ONE provided the most stable readings of PETCO2 as O2 flow increased with decrements of 4 mm Hg compared with 8–9 mm Hg with the other devices. Just as in the adult model scenarios, a standard O2 mask caused more CO2 rebreathing compared with the Cap-ONE (83% incidence with inspired PCO2 range of 1–17 mm Hg vs 2–5 mm Hg, respectively, P < .001) (see Fig. 3, C and D).
Comparisons of PETCO2 Between Devices as Supplemental O2 Flow Rate Increases in a Pediatric Model
Discussion
The main finding of this study was that regardless of measuring device strategy used, the PETCO2 signal deteriorates to varying degrees as supplemental O2 flow is increased to very high levels (>15 L/min for adult scenarios and ≥8 L/min for pediatric scenarios). In addition, the performance of the devices was altered, depending upon the simulated breathing pattern and expired CO2 concentration. Moreover, the apparent stability in PETCO2 observed over the range of supplemental O2 flows with the clinically expedient design came at the price of substantial CO2 rebreathing. Furthermore, the accuracy of this design was found to be dependent upon the capnograph with which it was interfaced.
Therefore, our results suggest that monitoring PETCO2 in non-intubated patients receiving supplemental O2 should be done with a product specifically designed for this purpose (ie, that has an open design that prevents rebreathing, particularly at relatively low flows). Careful attention should be given to monitoring mask position, inspired PCO2, and capnographic waveform to assess measurement accuracy. This is particularly important if the arterial PCO2 changes abruptly with the initiation of or adjustments to mask O2 flow, salient changes in the breathing pattern, or mask positioning.
In our early experimental runs, we discovered that despite the mask appearing to be fitted correctly, subtle discrepancies between the orientation of the CO2 cuvette and the stream of expired gas flow caused considerable errors. For example, the OxyMask positions the gas sampling structure relatively high. As a result, our inclination to position the mask in a traditional manner (ie, with the top of the mask at the bridge of the nose) initially caused larger deteriorations in PETCO2 (2–4 mm Hg lower at each level of O2 flow), compared with when the top of the mask was placed lower on the nose, something that most clinicians would be disinclined to do. However, in doing so, the gas sampling structure is directly over the mouth.
A similar situation occurred with our initial testing of the Cap-ONE system when a small misalignment of the mask apparently caused PETCO2 to decrease by 7 rather than 2 mm Hg as O2 flow increased. This finding is particularly important because movement of the patient's head or mouth, particularly when the securing straps become loose, could alter PETCO2 readings. This inherent limitation becomes particularly important when the device is used in a restless or agitated patient.
Most importantly, our results suggest that changes in PETCO2 alone cannot be relied upon as an accurate reflection of arterial CO2 tension, particularly when used to monitor patients with acute respiratory failure. Clinicians should be particularly cognizant of the fact that at higher levels of supplemental O2 flows, the correspondence between end-tidal and arterial CO2 is likely to diverge and cannot be taken for granted (particularly under conditions of hypoventilation). Therefore, clinicians might misinterpret a declining PETCO2 as signifying adequate ventilation while worsening oxygenation becomes a factor and O2 flow is increased in consequence.
A similar study previously examined whether PETCO2 can be accurately monitored in non-intubated patients receiving supplemental O2 therapy by mask. Takatori et al11 used an infant model to test the Cap-ONE system (simulated V̇E of 3 L/min and baseline PETCO2 of 38 mm Hg), when O2 flows of 2 and 5 L/min (67 and 167% of V̇E, respectively) were used. These O2 flows caused PETCO2 to decrease 0–4 mm Hg (at 2 L/min) and 3–7 mm Hg (at 5 L/min). By comparison, our study suggests better performance with specially designed capnography masks that generally maintained PETCO2 within 1–4 mm Hg at supplemental O2 flows that were the equivalent of 83–330% of V̇E (adult model, normal conditions) and between 1 and 5 mm Hg at O2 flows the equivalent of 40–277% of V̇E (pediatric model, normal conditions).
As suggested above, differences in the stability of PETCO2 over the range of supplemental O2 flow tested are multifactorial and not readily parsed. These include mask design and placement as well as their interactions with the dynamic relationship between O2 flow and V̇E. In addition to this, consideration must be given to sampling technique. The OxyMask/OxyKid and the CapnoLine/SmartCapnoline use sidestream technology, whereas the Cap-ONE uses mainstream technology. In addition, the sampling flows and their ranges differ between monitors. For example, both the Capnostream-20 and MX-450 use a mean sampling flow of 50 mL/min, which varies between 45–60 and 43–65 L/min, respectively,12,13 whereas the 8400 uses a sampling flow of 120 ± 20 mL/min.14
Our study highlights a heretofore underappreciated aspect of supplemental mask O2 therapy; namely, the ability to adequately washout CO2 from the mask requires that O2 flow match or exceed V̇E. Clinically, this is not possible to ascertain. Our results suggest that at high flows (≥15 L/min in adults and ≥8 L/min in relatively young children), this is unlikely to be a problem. However, the onset of hypercapnia (or an acute change in PaCO2 of ≥5 mm Hg) after the initiation of mask O2 therapy, should arouse suspicion that the O2 delivery strategy or flow setting may play a contributory role. As our study results demonstrate, the open nature of specially designed O2 capnography masks minimizes this risk. However, this also comes at the price of degraded PETCO2, which was observed in some conditions of the open mask designs.
Our study has several limitations. Foremost is the non-modifiable lack of an accepted standard instrument for measuring PCO2. This, coupled with the different measurement methods (ie, sidestream vs mainstream, oral guided design nasal cannula vs mask design), prevented us from establishing a baseline PETCO2. Our solution to this problem was to establish a stable PETCO2 with each device, with the model breathing spontaneously. We then used that as the control conditions for assessing each device once O2 flow was introduced.
The question therefore is whether the amount of CO2 titrated into the model was less in the oral guided design nasal cannula with a standard O2 mask because of enhanced CO2 rebreathing. Our CO2 flow meter only allowed a minimal reading of 0.5 L/min, and often we had to titrate below that level to achieve the targeted PETCO2 measured at the mask. The expectation of such a methodological bias is that for any subsequent O2 flow, more CO2 would be washed from the mask (ie, because less CO2 was being bled into the model), and therefore the measured PETCO2 would decline to a greater extent as O2 flow increased. However, this was not apparent from our results. When comparing the magnitude of PETCO2 change just from increasing O2 flow from 0 to 5 L/min, no clear pattern emerged, and this absence of a reproducible pattern was observed over all conditions (Fig. 5). As reported in our results, the mask by itself increased PETCO2 by 3 mm Hg under simulated normal breathing at a V̇E of 6 L/min (41–44 mm Hg).
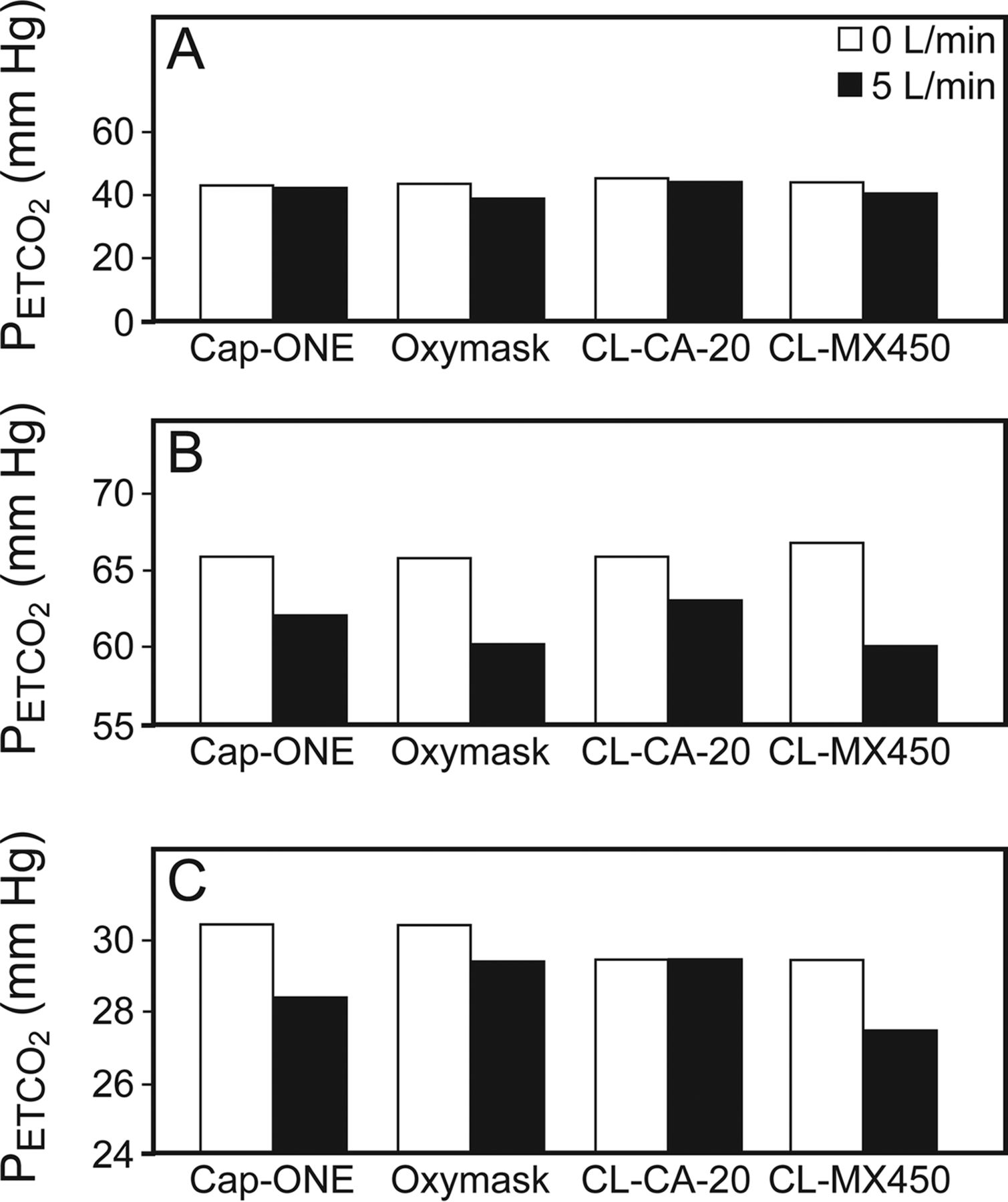
The initial drop in PETCO2 from baseline rebreathing conditions to the introduction of O2 flow measured during simulated normal ventilation (A), hypoventilation (B), and hyperventilation (C).
Other limitations became apparent during the study. First, the CapnoLine can be interfaced with different capnography devices, which is attractive in terms of convenience. Nevertheless, the disparity in our results between the CAP-20 and MX-450 monitors raises concerns about applying the results from one monitor to another, particularly when different monitors are used in the same institution. Second, model testing with stationary manikin faces makes the generalization of our results to clinical practice uncertain, because an almost endless variation in facial characteristics is encountered.
Third, bleeding gas mixtures into the piston of a lung simulator is a rather crude representation of respiratory physiology, wherein gas exchange occurs across both complex physiologic membranes and airway architecture, particularly under pathological conditions. Other studies that have tested PETCO2 stability between sidestream and mainstream nasal cannula devices have reported that the capnograph waveform deteriorates at very low tidal volumes (200 mL), and higher O2 flows as would be anticipated.15 However, this does not consider the fact that, unlike under in vivo conditions where all gas flow at the airway ceases, the constant bleed-in of CO2 into the ASL-5000 piston may also have entered the mask during late expiration and influenced our results.
On the other hand, this very limitation also provides an advantage in comparing devices. This is because dynamic, confounding variables, such as temporal fluctuations in global ventilation/perfusion relationships, as well as breathing patterns (including the presence of and variability in active expiratory muscle activity), are eliminated, so that performance differences among devices can be isolated.
Last, many of the differences between devices and monitors in maintaining stability in PETCO2, although clinically salient, may not be as great as seems apparent at first blush. For both the normal and hyperventilation patterns tested, the manufacturer's published literature states an accuracy of ±2 mm Hg for PCO2 values up to 40 mm Hg.12–14,16 Despite the fact that the dispersion in data was minimal (eg, the relative SD ranged from 0.3 to 2.8%) to non-existent (ie, 55% of all PETCO2 variables had an SD of 0 mm Hg), the resultant statistically significant differences within and between devices, measuring the same conditions, often were within the range of error. And for the hypoventilation scenarios, the stated accuracy of the monitors is approximately ±3 mm Hg.12–14,16
In summary, we found that specially designed O2 masks incorporating either mainstream or sidestream capnography generally maintain reasonable PETCO2 readings when supplemental O2 flows are in the range typically used during clinical practice as well as during unusually high settings. Using a standard O2 mask in concert with flow-directed nasal cannula-based capnography can, under some conditions, provide stable PETCO2 measurements, but it also carries a substantial risk of CO2 rebreathing. This risk is not related to the flow-directed nasal cannula, but rather to the design of standard O2 masks. This raises a heretofore underappreciated risk of standard O2 masks causing CO2 rebreathing, particularly at lower O2 flows.
Acknowledgments
We thank Dr Hong-Lin Du and Mr Germano Foti of Orange Medical, a Nihon Kohden company, for technical assistance with developing the model. We also thank Nihon Kohden and CareFusion for donations of supplies and a loan of equipment for this study.
Footnotes
- Correspondence: Justin S Phillips RRT, Respiratory Care Services, Bld-5, GA-2, Zuckerberg San Francisco General Hospital, 1001 Potrero Avenue, San Francisco, CA 94110. E-mail: Justin.Phillips{at}ucsf.edu.
This work was supported by an unrestricted gift from Nihon Kohden. The authors have disclosed no other conflicts of interest.
- Copyright © 2017 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}