

Abstract
BACKGROUND: Spontaneous breathing trials (SBTs) are used to assess the readiness for discontinuation of mechanical ventilation. When airway resistance (Raw) is elevated, the imposed work of breathing can lead to prolongation of mechanical ventilation. Biofilm and mucus build-up within the endotracheal tube (ETT) can increase Raw. Scraping the ETT can remove the biofilm build-up and decrease mechanical Raw. The primary aim of this study was to evaluate the impact of ETT scraping on Raw. The secondary aim was to determine whether decreasing Raw would impact subsequent SBT success.
METHODS: Intubated, mechanically ventilated subjects were enrolled if they failed an SBT and had an Raw of > 10 cm H2O/L/s. SBT failure was based on institutional guidelines, and Raw was calculated by subtracting the difference between the measured peak and plateau pressures using a square flow waveform with an inspiratory flow set at 60 L/min. The endOclear device was inserted into the ETT and withdrawn per manufacturer's guidelines. Scraping was repeated until the ETT was cleared. Change in Raw was compared pre- and post-ETT scraping using a paired t test. A Mann-Whitney U test evaluated the difference in percentage change in Raw between SBT groups.
RESULTS: Twenty-nine subjects completed the study. The mean pre- and post-ETT scraping Raw values were 15.17 ± 3.83 and 12.05 ± 3.19 cm H2O/L/s, respectively (P < .001). Subsequent SBT success was 48%; however, there was no difference in percentage change in Raw between subsequent passed SBT (18.61% [interquartile range 8.90–33.93%]) and failed SBT (23.88% [interquartile range 0.00–34.80%]), U = 78.5, z = −0.284, P = .78. No adverse events were noted with ETT scraping.
CONCLUSIONS: This study demonstrated that ETT scraping can reduce Raw. The decrease in Raw post-ETT scraping did not affect subsequent SBT success.
- mechanical ventilation
- resistance
- spontaneous breathing trial
- biofilm
- endotracheal extubation
- work of breathing
- airway obstruction
- endotracheal tube
- endotracheal tube obstruction
- secretion removal
Introduction
A spontaneous breathing trial (SBT) is the evaluation of a patient's ability to balance the respiratory load or work of breathing (WOB) with his or her respiratory capacity to do the work. Due to factors that cause a load/capacity imbalance (eg, increased airway resistance [Raw], decreased lung compliance), it is important that clinicians avoid suboptimal conditions when performing SBTs. An example is mucus buildup in the endotracheal tube (ETT), which results in luminal narrowing of the tube. It is thought that this narrowing imposes an unnecessary increase in the WOB due to the increase in Raw.1 Efforts have been made to understand the degree of this ETT luminal narrowing. Mietto et al2 measured this by using high-resolution computed tomography, noting that ETT narrowing is common and correlates with an increase in air-flow resistance. This narrowing occurred despite adequate humidification and suctioning.
Endotracheal tube scrapers have been described in the literature as devices that may be able to restore the original internal diameter of the ETT by removing accumulated secretions and biofilm.3,4 At our institution, we utilize the endOclear (Endoclear LLC, San Ramon, California) to clear secretions when ETT obstructions are suspected. Although we have used it safely, it is unknown what impact its use has had on Raw and overall WOB in spontaneously breathing patients. Furthermore, it is unclear whether the resolution of the associated increase in Raw and WOB has any impact on subsequent SBT success in our institution.
An inspiratory Raw of < 10 cm H2O/L/s is considered acceptable in intubated patients.5 We sought to evaluate the impact of ETT scraping on Raw in subjects with a measured Raw of > 10 cm H2O/L/s. The secondary aim of this study was to determine whether decreasing imposed work of breathing impacted success of the subsequent SBT.
QUICK LOOK
Current knowledge
Biofilm and mucus build-up within the endotracheal tube (ETT) can increase airway resistance (Raw). When Raw is elevated, the imposed work of breathing can lead to prolongation of mechanical ventilation. Cleaning an ETT with a tube scraper can remove the biofilm build-up, restore ETT patency, and decrease mechanical Raw.
What this paper contributes to our knowledge
Using a tube scraper to remove secretions from an ETT can reduce mechanical Raw by a statistically significant amount.
Methods
This prospective observational study was conducted between December 2013 and October 2015 at Rush University Medical Center, a large urban academic medical center located in Chicago, Illinois. The study protocol, including waiver of consent, was approved by our institutional review board. Waiver of consent was requested after the study was initially approved, because the endOclear device was being used on mechanically ventilated patients with an increased Raw in our institution. Subjects were included if they failed at least one SBT as documented in the electronic medical record and had an Raw > 10 cm H2O/L/s. Raw was measured by temporarily changing the ventilator mode to continuous mandatory ventilation in a square flow waveform at 60 L/min and calculating the difference between the peak and plateau airway pressures.
Spontaneous breathing trials are performed daily by the respiratory therapists per physician order at our institution after they have been assessed for extubation readiness. Qualifiers for SBT failure include an increased respiratory rate, tachycardia attributed to SBT, complaint of distress, anxiety, and a rapid shallow breathing index > 105 (see Appendix 1 in the supplementary materials at http://www.rcjournal.com). Study staff were notified by respiratory therapists when mechanically ventilated adults failed at least one SBT. Members of the study team confirmed the SBT failure based on documentation in the electronic medical record.
Tube Clearance Procedure
Ventilator data, including peak and plateau pressure, was recorded pre- and post-tube scraping to assess changes in the calculated Raw. Raw was measured as described above. Subject assessment data were also recorded pre- and post-tube scraping to assess subject safety and tolerance with the tube scraping procedure. Data included breathing frequency, tidal volume, rapid shallow breathing index, heart rate, blood pressure, and accessory muscle use.
During the tube clearance procedure, study subjects were hyperoxygenated and suctioned via in-line suction catheter as per department policy. That policy dictates that the catheter should be advanced until resistance is met and then withdrawn slowly for a duration no longer than 15 s while applying negative pressure. The endOclear device was inserted and deployed into the ETT until it was 1 cm above the terminal end of the tube. This placement was based on alignment of the numbers on the ETT and endOclear device. It was then withdrawn over a period of 5–10 s. Any secretions extracted were collected in the small attached vial and visually inspected. A second pass was performed if necessary to clear all of the secretions from the ETT. Per study protocol, if Raw decreased by 3 cm H2O after the initial scraping, this process could be repeated before the next planned SBT if the Raw had increased by 3 cm H2O or more since the initial scraping. If Raw remained the same or decreased from the initial scraping, a subsequent attempt was not required before the subsequent SBT was performed. The study staff were trained to measure Raw and perform endotracheal tube scraping as described above. We also collected data on ETT size, primary diagnosis, duration of mechanical ventilation, and follow-up SBT results (Table 1).
Subject Information
Statistical Analysis
SPSS (version 23.0, IBM Corp, Armonk, New York) was used to analyze all collected data. A paired t test was conducted to evaluate the mean difference in pre- and post-ETT scraping. A Mann-Whitney U test was used to evaluate the difference in percentage change in Raw between SBT groups.
Results
Population
During the study period, 34 subjects were initially enrolled in the study. Twenty-nine subjects completed the study, because 5 subjects either refused the tube scraping or had missing data noted at the time of final analysis. All adult ICUs were utilized, including the surgical, neuroscience, medical, and cardiac ICUs. Subject disease states were categorized as primarily respiratory, cardiac, neurologic, septic, or other. Nine subjects were categorized as respiratory, of whom 2 had the primary diagnosis of COPD exacerbation, 2 had hypercarbic respiratory failure, 2 had pulmonary embolism, one had pulmonary sarcoidosis, one had lung cancer complicated by pneumonia, and one had an asthma exacerbation.
Airway Resistance and SBT Success
The mean pre- and post-ETT scraping Raw was 15.17 ± 3.83 cm H2O/L/s and 12.05 ± 3.19 cm H2O/L/s, respectively (P < .001). The success of subsequent SBT was 48%; however, there was no difference in the percentage change in Raw between subsequently passed SBT (18.61% [interquartile range 8.90–33.93%]) and failed SBT (23.88% [interquartile range 0.00–34.80%]), U = 78.5, z = −0.284, P = .78. There were no adverse events associated with ETT scraping (Figs. 1 and 2).

Mean airway resistance before (± 3.83 SD) and after (± 3.19 SD) endOclear treatment.
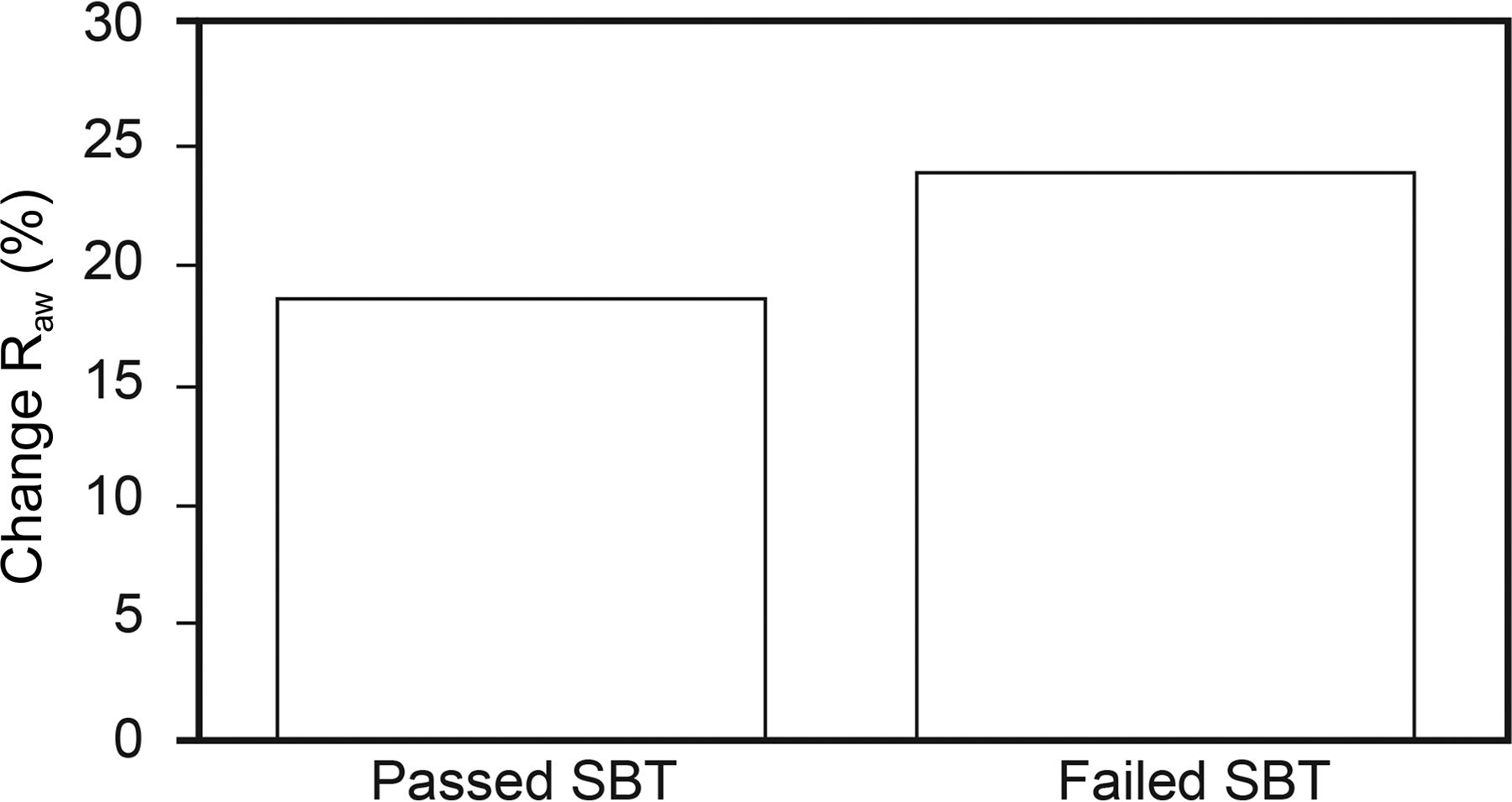
Median percentage change (decrease) in airway resistance after ETT scraping in subjects who subsequently passed (19%, interquartile range [IQR] 9–34) or failed (24%, interquartile range 0–35) a spontaneous breathing trial (SBT). P = .78.
Discussion
Our findings indicate that ETT scraping can significantly lower the imposed Raw due to secretion buildup in the lumen of the endotracheal tube in subjects managed in adult ICUs who are receiving mechanical ventilation. Although statistically significant, the clinical importance of this approximately 3-cm H2O/L/s drop in mean Raw post-scraping remains questionable. To assess whether there is a clinical impact, we compared the change in resistance pre- and post-scraping between the study subjects who subsequently passed the SBT and those who failed. We found no difference, which suggests that our targeted Raw of > 10 cm H2O/L/s was too low or Raw has less of an impact on SBT success than previously thought.
It has been reported that the increase in Raw can cause respiratory mechanics to deteriorate during an SBT.6 The resistive load on the respiratory muscles can become too great for these critically ill patients, resulting in SBT failure. The exact amount of Raw that results in the adverse outcome of SBTs is not yet known. Resistive loads may be higher when patients have ETT sizes of < 7.0-mm inner diameter (ID). This suggests that ETT sizes of > 7.0 mm may impose negligible work if the tube is kept clean and unobstructed.7 In our study, one subject was intubated with a 6.5-mm ID ETT, and the others had 7.0-mm ID or larger ETTs. To account for the variable resistance of the different size ETTs used in this study, all SBTs were conducted using automatic tube compensation. This spontaneous mode compensates for the ETT's imposed resistance based on the documented airway size and the patient's peak inspiratory flow. Thus, the lack of difference in SBT success post-scraping is mostly likely not due to variability in ETT size.
In a study by Wilson et al,8 it was noted that clinicians may assume that Raw imposed by ETT is minimized when the tube is properly sized for the patient. In fact, clinicians make adjustments to the mechanical ventilator to overcome the imposed Raw when it is suspected. Industry standards of ETT manufacturing regulate diameter consistency at production. It is mandated that ETTs with an ID of ≥ 6.5 mm have a no-more-than 0.20-mm variability. This implies that Raw can be predicted, because the ID of the ETT is precisely known. Interestingly, their study found that after intubation, secretions can have a significant impact on the resistance of the ETT. This has previously been thought to be clinically important, since it directly impacts WOB. Nearly 50% of all of the ETTs that they studied had a resistance that was equal to one tube size smaller. The authors suggest that this would be similar to having an ETT with ID of 7.5 mm that has the resistance of a 6.5-mm ID tube.8 Their research suggests that secretions inside of an ETT unnecessarily increase Raw and WOB in patients during SBTs and lead to a perceived failure of the SBT. This finding would support the use of ETT scraping to reestablish the original ETT ID to allow a truer weaning assessment.8 In addition to an Raw of > 10 cm H2O/L/s being too low to identify patients with a clinically important increase in Raw, the lack of clinical importance may also be related to the short period of time that most patients are undergoing an SBT, typically 30 min, based on department practice. However, the minimum of a 30-min SBT is consistent with previously published guidelines that were available during the time our study was conducted.9
The subsequent SBT pass rate in our study was not improved by lowering the Raw. Subjects with the largest percentage change in Raw after ETT scraping actually failed the SBT at a rate similar to the subsequent SBT pass group (48%). The difference in the percentage change from pre- and post-tube scraping was not statistically significant; however, the findings suggest that a decrease of approximately 19–24% in Raw may not be enough to improve the success of subsequent SBTs. This finding warrants further study to determine the amount of Raw improvement with ETT scraping that is clinically relevant.
There are several limitations to this study. First, we did not account for the many reasons that a patient may fail a subsequent SBT. We only ensured that Raw was reduced to the lowest amount possible using the endOclear device. Second, our sample size was small and was primarily aimed at assessing whether the Raw could be significantly reduced by ETT scraping in those subjects who failed the initial SBT. Another limitation could be the unknown secretions that remained in the ETT after scraping, since we only decreased mean Raw by approximately 3 cm H2O/L/s. The Raw remained elevated in a majority of our subjects studied. A more significant decrease may have had a greater impact on WOB and improved SBT success.
Conclusions
The purpose of this study was to assess the impact of ETT scraping on Raw in mechanically ventilated patients. ETT scraping can significantly reduce Raw in patients with an Raw of > 10 cm H2O/L/s. This reduction in resistance did not improve subsequent SBT success. Based on our results, we cannot make a recommendation on the use of ETT scraping to improve SBT success in patients with an Raw of > 10 cm H2O/L/s. Future studies are needed to define the level of Raw at which ETT scraping would impact SBT success.
Footnotes
- Correspondence: J Brady Scott MSc RRT-ACCS AE-C FAARC, Division of Respiratory Care, Department of Cardiopulmonary Sciences, Rush University, Armour Academic Center, 600 S Paulina, 751 AAC, Chicago, IL 60612. E-mail: jonathan_b_scott{at}rush.edu.
Mr Scott presented a version of this paper as an Editor's Choice abstract at AARC Congress 2016, held October 15–18, 2016, in San Antonio, Texas.
Endoclear LLC supplied the endOclear devices free of charge. Mr Scott discloses relationships with Bayer Pharmaceuticals, Aerogen, and Sunovion Pharmaceuticals. Ms Dubosky discloses relationships with Halyard and Aerogen. Mr Vines discloses relationships with Teleflex, Aerogen, Carefusion, Covidien, Bayer Healthcare, Boehringer Ingelheim, Halyard, and Ohio Medical. Dr Balk discloses relationships with Ohio Medical, Roche Scientific, Thermo Fisher Scientific, bioMerieux, CDC, Immunexpress, and Asahi Kasei. The other authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2017 by Daedalus Enterprises





{kind=link}
{kind=link}