

Abstract
BACKGROUND: The 2005 American Thoracic Society/European Respiratory Society guidelines for single-breath diffusing capacity of the lung for carbon monoxide (DLCO) recommend a weekly biological control test and/or DLCO simulator to detect instrument error drift. Very little has been published regarding the results of such a quality assurance program. Our aim was to analyze the long-term stability of a portable DLCO instrument.
METHODS: We used a new EasyOne Pro system and checked its accuracy using a DLCO simulator with 2 reference gases (concentration A: carbon monoxide [CO] = 0.1% and helium = 6.52%; concentration B: CO = 0.08% and helium = 7.21%) during the first 3 y of use in our large clinical laboratory. To detect instrument drift, a healthy woman (MSC), age 43 y old at baseline, tested herself every week during this period of time.
RESULTS: More than 6,000 spirometry and 5,000 DLCO maneuvers were done using this instrument for patients during these 3 y. There were no failures in the daily volume and flow checks or the CO and helium calibration checks performed automatically by the instrument. The differences between the simulator DLCO and the measured DLCO were −0.91 ± 1.33 mL/min/mm Hg and −0.61 ± 1.45 mL/min/mm Hg for concentration A and concentration B, respectively. The results of the 110 biological control tests were: mean 30.8 ± 1.7 mL/min/mm Hg (95% CI 30.5–31.1), coefficient of variation of 5.4% in DLCO, and repeatability of 2.5 mL/min/mm Hg. Only 4 measurements were outside ±3 mL/min/mm Hg (3.6%). Her mean alveolar volume was 4.2 ± 0.25 L with coefficient of variation of 6.2%; her inspired volume was 3.05 ± 0.14 L, and coefficient of variation = 4.5%.
CONCLUSIONS: Measurements of DLCO were stable over the 3-y period without any need for manual recalibration of the instrument. The biological control was as good as the DLCO simulator to evaluate this kind of device in a long-term laboratory quality control program.
Introduction
Single-breath diffusing capacity of the lung for carbon monoxide (DLCO) tests have considerable clinical value for detecting the emphysema COPD phenotype and for changing the pretest probability of an interstitial lung disease or pulmonary vascular disease in patients with dyspnea.1 Once a diagnosis is established, a change in DLCO can help to determine treatment response or disease progression. However, the accuracy and reproducibility of DLCO results from one laboratory to another has been highly variable, causing an increased rate of misclassification in interpretations.2,3 We have previously reported the quality of spirometry tests done in our laboratory,4,5 but very little has been published regarding the results of DLCO quality assurance programs in clinical pulmonary function testing (PFT) laboratories, so our aim was to analyze the results for a new DLCO instrument and report it here. We hypothesized that the DLCO device is a stable long-term clinical instrument and that both simulator and biological-based quality control strategies may be appropriate in terms of follow-up.
QUICK LOOK
Current knowledge
The 2005 American Thoracic Society/European Respiratory Society guidelines for single-breath diffusing capacity of the lung for carbon monoxide (DLCO) recommend a weekly biological control test and/or DLCO simulator to detect instrument error drift. Very little has been published regarding the results of such a quality assurance program.
What this paper contributes to our knowledge
Our study demonstrates that measurements of DLCO were stable over the 3-y period without any need for manual recalibration of the instrument. The biological control was as good as the DLCO simulator to evaluate this kind of device in a long-term laboratory quality control program.
Methods
In 2010, we acquired an EasyOnePro system (ndd Medical Technologies, Zurich, Switzerland) to measure FVC, slow VC, and DLCO for patients referred to our large clinical laboratory in México City (altitude 2,250 m). Before placing the instrument into clinical use, we verified the accuracy of DLCO measurements using a DLCO simulator (series 5560, Hans Rudolph, Shawnee, Kansas), testing with 2 different 1% precision reference gases, (concentration A: carbon monoxide [CO] = 0.1% and helium = 6.52%; concentration B: CO = 0.08% and helium = 7.21%), producing DLCO target values of about 10, 20, and 35 units, calculated using EasyLab software, with inspired volumes from 2–5 L. A difference from target of ± 2.0 DLCO units was used as the threshold to initiate an investigation into possible causes of error.6 Throughout this paper, for easier reading, we will use the term units in place of mL/min/mm Hg. The instrument checked the accuracy of the CO and helium sensors automatically before each test session by performing a 5-point calibration using test gas, mixed gas, and ambient air. This calibration allows automatic determination of sensor gain, offset, and drift. As an additional component of our instrument quality assurance program, we routinely tested a biological control subject, a healthy woman (MSC), age 43 y old at baseline, who tested herself every week. Two DLCO maneuvers were done to obtain repeatability matching. The same healthy woman measured slow VC as well as FVC each week. Her baseline DLCO and short-term variability were determined from her first 20 tests. The instrument was then considered “out of control” if her current DLCO was outside of her baseline range. Instrument troubleshooting would then be performed to determine the cause of the DLCO drift. During the 3 y of use, we checked the absolute DLCO accuracy using the DLCO simulator. The accuracy of the ultrasonic flow sensor was checked at the beginning of each testing day using a 3.0-L calibration syringe (CareFusion, Hoechberg, Germany) for volume and flow check and every week at 3 different flows for linearity, for both inspired and expired volumes. The acceptable range was 2.91–3.09 L (±3%).7
Patient testing was done according to 2005 American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines for spirometry and DLCO.8 Instrument software versions during this period of time were from 1.1.7.0 to 1.4.1.0. Four different PFT technologists, with National Institute for Occupational Safety and Health certificates for spirometry, all with at least 8 y of experience, used the instrument (and others) to test patients referred to the PFT laboratory. Certification of PFT technologists for DLCO is not available in México. Reference equations used for spirometry and DLCO were from Pérez-Padilla et al9 and Crapo et al,10 respectively.11 An acceptable DLCO maneuver had a breath-hold time from 8 to 12 s, a test gas inspired volume >85% of the largest vital capacity (slow VC or FVC), an inspiratory time ≤4 s, and a sample volume ≥0.1 L. The instrument displays error messages whenever a maneuver is not acceptable according to these standards. A good quality DLCO test session included at least 2 acceptable DLCO results, which matched within 3.0 units. The instrument displays and prints a DLCO quality grade (A–F) according to the degree of DLCO repeatability within the test session. A database within the instrument stored all test results and maneuver graphs as well as calibration checks and biological control results. After 3 y of testing patients, we transferred the accumulated results to a computer for statistical analyses (Stata 13, StataCorp, College Station, Texas). The results were summarized as the coefficient of variation = SD/mean, and repeatability was summarized as 1.96 × SD. Root mean square, coefficient of variation, and range percentiles of intra-subject DLCO test values were calculated. The ethics committee of our institution approved the study, and the tested biological control gave her written informed consent.
Results
More than 6,000 FVC, 2,000 slow VC, and 5,000 DLCO maneuvers were done using the instrument during the study period. From 694 DLCO test sessions done for subjects, 86.6% met ATS/ERS acceptability goals,8 and 93.2% were repeatable within 3 units. The rates of each type of maneuver error are given in Table 1. The rates for each DLCO quality grade are shown in Table 2. The within-subject variability of DLCO (the degree of matching), expressed as the root mean square coefficient of variation, was 5.4%, and the repeatability (1.96 × SD) was 1.57 units.
Single-Breath Diffusing Capacity of the Lung for Carbon Monoxide Maneuver Acceptability
Rates for Each Diffusing Capacity of the Lung for Carbon Monoxide Quality Grade
There were no failures in the daily volume and flow checks using the 3.0-L syringe or the CO and helium calibration checks performed automatically by the instrument. The differences (or error) between the simulator DLCO and the measured DLCO were −0.91 ± 1.33 units (95% CI from −0.94 to −0.89) for CO and helium concentration A and −0.61 ± 1.45 units for concentration B (95% CI from −4.6 to 6.2) (Fig. 1).
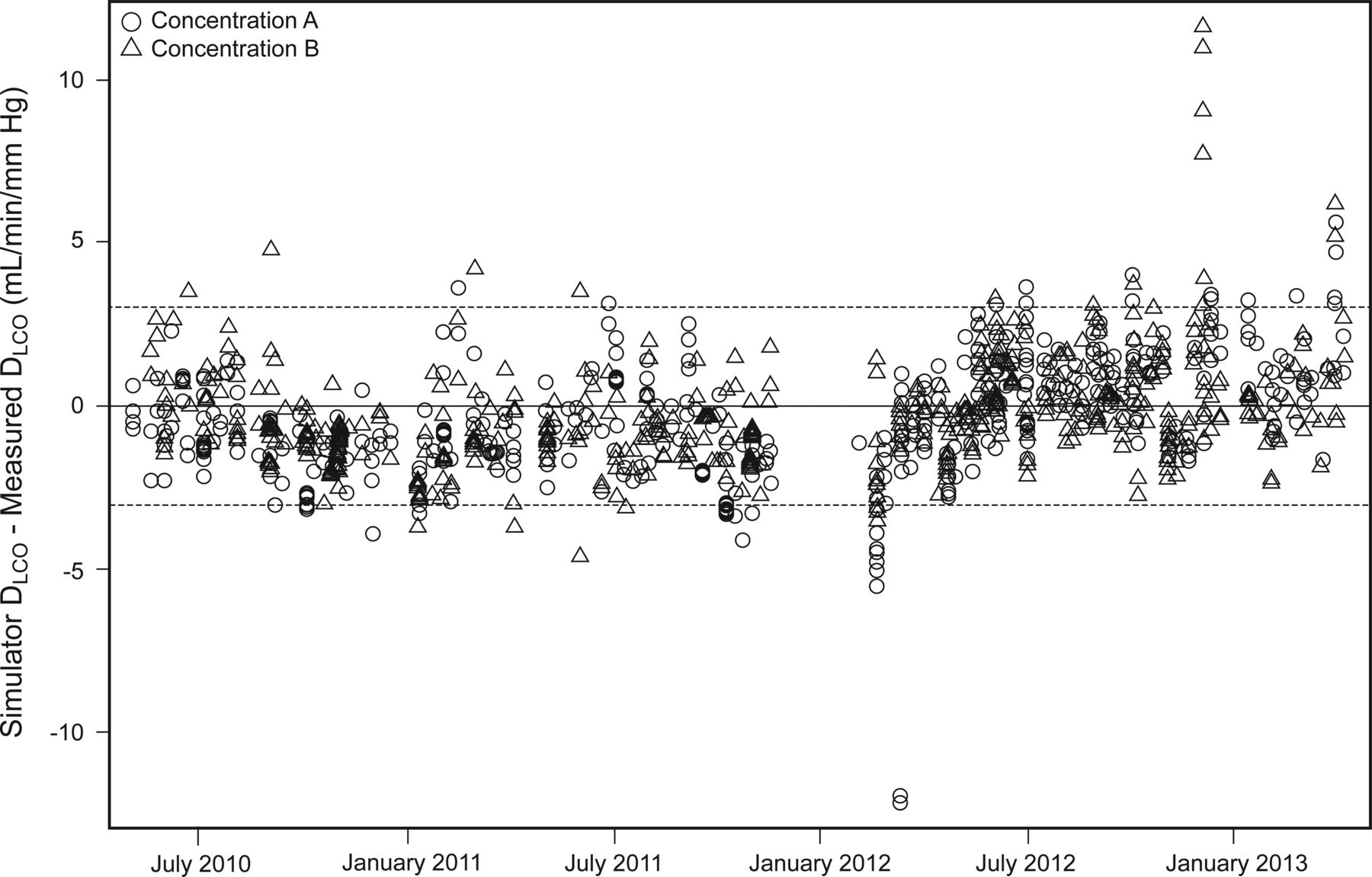
Differences between the simulator diffusing capacity of the lung for carbon monoxide (DLCO) and measured DLCO during the 3 y of testing hundreds of subjects, at different CO and helium gas concentrations (concentration A: CO = 0.1% and helium = 6.52%; concentration B: CO = 0.08% and helium = 7.21%). Dashed lines show ±3 mL/min/mm Hg.
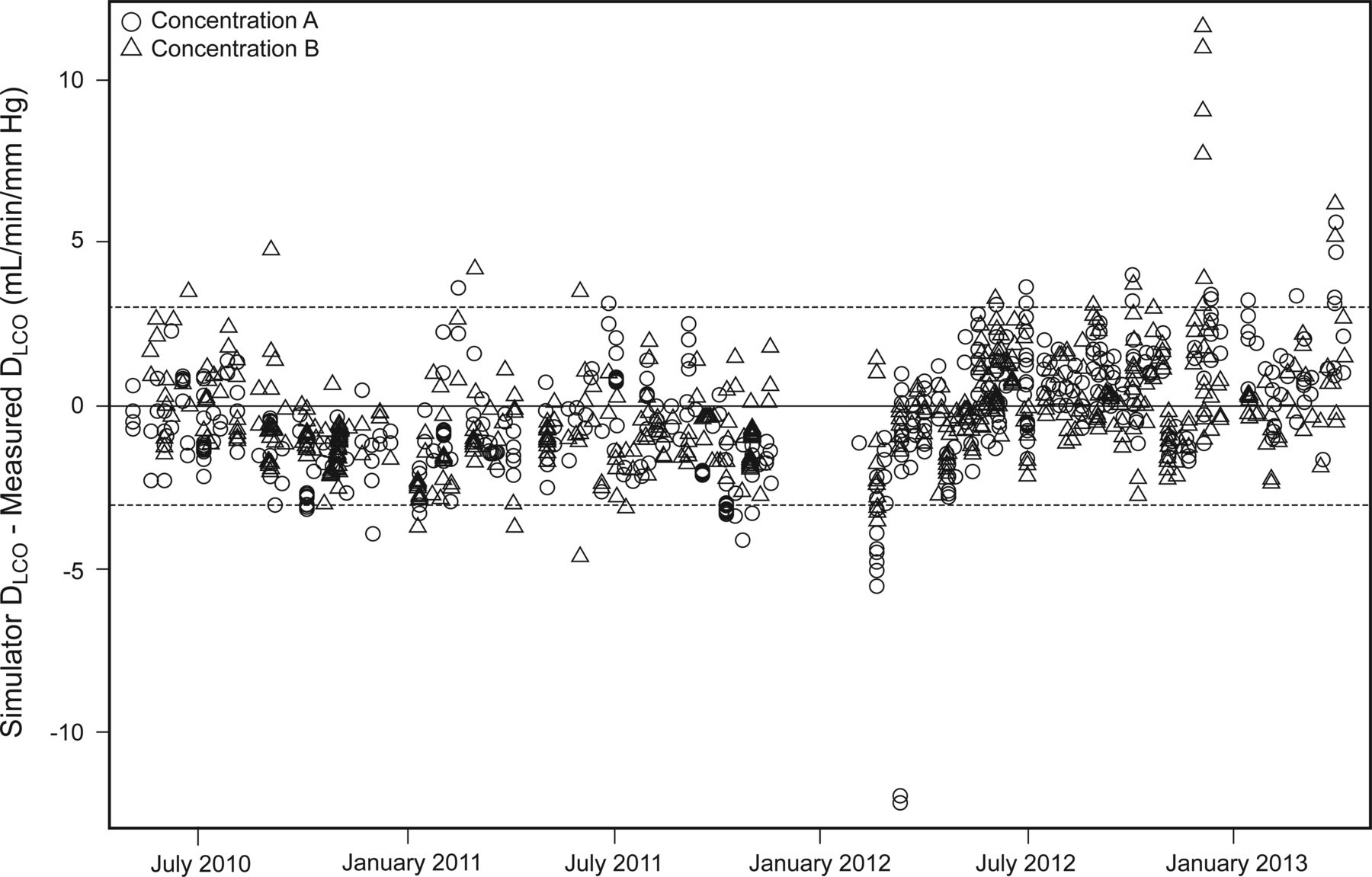
The results of the 110 biological control test sessions done by the healthy technologist are plotted in Figure 2. Her mean DLCO was 30.8 ± 0.16 units (95% CI 30.5–31.1), the coefficient of variation was 5.4%, and the repeatability was 2.5 units; during this period, the slow vital capacity was 3.2 ± 0.08 L and the FVC was 3.12 ± 0.09 L, with a coefficient of variation of 2.5 and 2.9%, respectively. Only 4 DLCO measurements (3.6%) were outside ±3 units of her mean value. Her mean alveolar volume was 4.2 ± 0.25 L with a coefficient of variation of 6.2%, and her mean inspired volume was 3.05 ± 0.14 L (coefficient of variation = 4.5%). When the measurements were out of control, the biological control repeated the maneuver, and if the error continued, we informed the distributor of the device. During the 3-y period, we had to perform maintenance 3 times (maintenance includes exchanging a few parts accessible to the user). When the error was high, the problem was resolved by changing the hose that goes from the device to the sensor or by changing the seals; when the error coincided with a respiratory infection suffered by the biological control, the results returned to her mean values after the infection resolved, in that case, we did not make any changes.

Variability of bio-quality control diffusing capacity of the lung for carbon monoxide (DLCO) values from a healthy technologist over 3 y. Dashed lines represent ±3 mL/min/mm Hg from the mean. Her mean DLCO was 30.8 ± 1.7 SD; the coefficient of variation was 5.4%; and the repeatability was 2.5 mL/min/mm Hg. Only 4 measurements (3.6%) were outside ±3 mL/min/mm Hg of her mean value.
Discussion
Several factors affect the false positive and false negative rates for the interpretation of DLCO results.12 These include the training and enthusiasm of the technologist performing the tests for meeting guidelines for maneuver acceptability and repeatability13; the accuracy and reproducibility of the instrument14; the inherent biological variability of the patient (including changes in hemoglobin and carboxyhemoglobin); the degree of DLCO impairment (a very low VC or very low DLCO causes low sample volumes, which cause errors in some instruments); the choice of reference equations (especially for very elderly patients and those with non-white ethnicity); thresholds for abnormality (80% predicted vs the 5th percentile lower limit of the normal range); the availability of clinical information that can be used to estimate the pretest probability of various diseases that can affect the DLCO; and the training, experience, and skill of the physician who interprets the test results (especially those with suboptimal quality). A quality control program for the instrument substantially improves the accuracy and visit-to-visit reproducibility of DLCO results15–17 but does not address the other factors, so a comprehensive approach is needed to minimize misclassification and optimize the value of the test for clinical decision making.
The DLCO simulator checks the accuracy of DLCO results at 3 levels within the clinical range. At the beginning of a multi-center international study of inhaled insulin, the simulator was used to check the accuracy of the DLCO machines (12 different models) used at the PFT laboratories of the 125 study sites.16 Equipment at one fourth of those sites failed the initial DLCO simulation testing. After correcting instrument issues or purchasing new equipment, all but one of the 125 sites were confirmed to be measuring DLCO and alveolar volume accurately. A similar multi-site study asked the PFT laboratories to use the DLCO simulator every 8 weeks. Over 16,000 DLCO simulations were performed. Systems outside of control limits (3.0 units) were detected on 5.8% of tests. Significant differences were noted in inter-device average, with ranges from −5.0 to +2.1%. Higher inspired volume and higher alveolar volumes were associated with larger DLCO differences. Larger DLCO errors were noted for device temperatures <21°C and >27°C.
A clinically important difference in DLCO from one visit to another in patients with interstitial lung disease or pulmonary vascular disease is considered a change of ∼15%.18–22 The long-term reproducibility of the instrument, as estimated by the biological control testing of the healthy technologist (95% of the values within 3 units of her mean DLCO and a coefficient of variation of 5.4%) suggests that clinicians retesting patients during follow-up visits in a laboratory with good quality control could be highly confident that a measured change of >15% is outside the measurement noise and is clinically important.
There are some limitations with the use of the DLCO simulator. The device relies on the delivery of a precise volume of test gas and also depends on the test gas being extremely accurate. Since a syringe delivers the volume, any damage could alter the volume of test gas to the tested instrument. Operator errors (eg, software settings, valve initiations) in the DLCO simulator will alter the desired targets. The precision test gas has to be mixed via a gravitational method, as opposed to via filling pressures, which is much more accurate. This ensures that the gases in the simulator gas have tolerances that will not affect the desired target DLCO. Estimates of the errors for both volume and simulator gas in DLCO targets are ∼1%.
Conclusions
Measurements of DLCO were stable over the 3-y period without any need for manual recalibration of the instrument. The biological control was as good as the DLCO simulator to evaluate this kind of device in a long-term laboratory quality control program.
Footnotes
- Correspondence: Luis Torre-Bouscoulet MD MSc, Departamento de Fisiología Respiratoria, Instituto Nacional de Enfermedades Respiratorias, “Ismael Cosío Villegas,” Tlalpan 4502, Colonia Sección XVI Delegación Tlalpan CP 14080, México. E-mail: luistorreb{at}gmail.com.
Dr Gochicoa-Rangel presented a version of this paper at the 2015 European Respiratory Society International Conference, held September 26–30, 2015, in Amsterdam, Netherlands.
The authors have disclosed no conflicts of interest.
- Copyright © 2017 by Daedalus Enterprises





{kind=link}
{kind=link}