

Abstract
BACKGROUND: An objective method to evaluate thoracoabdominal movement is needed in daily clinical practice to detect patients at risk of hypoventilation and to allow for timely interventions in neuromuscular diseases. The clinical feasibility, reliability, and validity of a newly developed method for quantifying respiratory movement using fiber grating sensors, called the Respiratory Movement Evaluation Tool (RMET), was evaluated.
METHODS: The time needed to measure respiratory movement and the usability of the measurement were determined by 5 clinicians using the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) 2.0 questionnaire. Thoracoabdominal movement was measured using RMET 3 times in 10 healthy subjects to evaluate intraclass correlation coefficients (ICC). The subjects were encouraged to breathe 10 times while voluntarily changing the amount of air during ventilation simultaneously with the RMET and a spirometer, and their correlations were evaluated to test validity using Pearson's product-moment correlation coefficients. The same measurements were also performed in 10 subjects with Duchenne muscular dystrophy.
RESULTS: Real-time recordings of thoracoabdominal movements were obtained over a mean time of 374 ± 23.9 s. With QUEST 2.0, the median score of each item exceeded 3 (more or less satisfied). In healthy subjects, ICC(1,1) ranged from 0.82 to 0.99, and ICC(2,1) ranged from 0.83 to 0.97. Significant correlations were observed between the respiratory amplitudes measured with RMET, and the amount of air during ventilation was measured with a spirometer (r = 0.995, P < .001). In subjects with Duchenne muscular dystrophy, ICC(1,1) ranged from 0.87 to 0.97, and ICC(2,1) ranged from 0.84 to 0.99. The respiratory amplitudes measured with RMET correlated significantly with the amount of air during ventilation with a spirometer (r = 0.957, P < .001).
CONCLUSIONS: We developed a novel method of quantifying respiratory movement called RMET that was feasible to use in daily clinical practice.
- breathing
- breathing movement
- device
- motion analysis
- chest wall
- abdominal wall
- Duchenne muscular dystrophy
- pulmonary function test
Introduction
In neuromuscular diseases, respiratory impairment is a major cause of morbidity and mortality.1 The consequences of progressive respiratory muscle weakness are low tidal volume, ineffective cough, recurrent respiratory infections, progressive airway obstruction, and sleep-disordered breathing, ultimately leading to alveolar hypoventilation and respiratory failure.2 Assessment of respiratory function, which includes spirometry, maximum inspiratory and expiratory pressures, cough peak flow, and blood gas analysis, has been shown to generally facilitate the prevention of complications.3
Decreased mobility of the chest wall is one of the major causes of alveolar hypoventilation and respiratory failure in neuromuscular diseases.2,4 Respiratory muscle weakness results in low tidal volumes with disease progression.2,4 Low tidal volumes lead to decreased mobility of the chest wall caused by reduced rib cage distention, which allows contractures of costovertebral joints and stiffening of chest wall tendons and ligaments.2 Finally, decreased compliance of the rib cage and subsequent muscle fatigue result in progressive declines in tidal volume and alveolar hypoventilation with hypoxemia and hypercarbia.5
Lung volume recruitment techniques have been reported to be effective for neuromuscular diseases to prevent contractures of the chest wall and maintain the compliance of the lung.6–8 Therefore, an objective method to evaluate thoracoabdominal movement is needed in daily clinical practice to detect patients at risk of hypoventilation and to allow for timely interventions.
Conventional methods that assess mobility of the chest wall include a magnetometer,9 respiratory inductance plethysmography,10 stretching belts,11 the Respiratory Movement Measuring Instrument,12 optoelectronic plethysmography,13,14 magnetic resonance imaging,15,16 and a breathing movement measuring device.17,18 Use of these methods, except for optoelectronic plethysmography, to assess thoracoabdominal movement in neuromuscular diseases has not been reported.
Optoelectronic plethysmography has been used for the assessment of thoracoabdominal movement in neuromuscular diseases.19–21 Reliability of the optoelectronic plethysmography method in healthy subjects has been reported, with intraclass correlation coefficient (ICC)(1,1) and ICC(2,1) being over 0.75.22,23 The validity of the optoelectronic plethysmography method was evaluated in different populations, such as healthy subjects and subjects with COPD, by comparing tidal volume and inspiratory capacity obtained by means of this instrument with those measured by a spirometer.22,24 However, some hurdles must be overcome before it can be used in daily clinical practice. It requires 4 cameras from multiple directions and 86 markers to obtain accurate measurement of ventilatory parameters, as well as 45–60 min to perform the measurements by 2 persons, excluding time needed for equipment setup and volume estimation.13 In addition, a wide area of 8.0 × 1.5 × 1.5 m is needed to perform the measurements.13
The potential to evaluate respiratory functions with a new device called a fiber grating vision sensor has been reported.25,26 The fiber grating sensor is a 3-dimensional image sensor that monitors respiratory movement without contact.25 The fiber grating sensor can detect changes of hundreds of infrared light spots on the body surface in the vertical direction (ΔZ) with each breath. Additionally, this sensor has the advantages of being portable and easy to use in all clinical environments.26
We developed a novel quantitative method to assess respiratory movement using fiber grating sensors called the Respiratory Movement Evaluation Tool (RMET) to analyze thoracoabdominal mobility in neuromuscular diseases. The purpose of this study was to demonstrate its clinical feasibility, inter- and intra-rater reliabilities, and concurrent validity. The hypothesis of this study is that RMET is feasible to use in daily clinical practice and has excellent inter- and intra-rater reliabilities and high concurrent validity for healthy subjects and subjects with Duchenne muscular dystrophy.
QUICK LOOK
Current knowledge
Decreased mobility of the chest wall is one of the major causes of alveolar hypoventilation and respiratory failure in neuromuscular diseases. Optoelectronic plethysmography has been used for the assessment of thoracoabdominal movement, however, there are hurdles to overcome for use in daily clinical practice in terms of time and space needed. The potential to evaluate respiratory function with a new device called a fiber grating vision sensor has been reported.
What this paper contributes to our knowledge
We developed a novel method for assessing thoracoabdominal movement in neuromuscular diseases called the Respiratory Movement Evaluation Tool (RMET) using a fiber grating vision sensor. The RMET demonstrated an acceptable level of time needed for measurement of respiratory movement and sufficient usability by clinicians. Although it was a small sample size, RMET measurements demonstrated sufficient reliability and validity in healthy subjects and in subjects with Duchenne muscular dystrophy.
Methods
Participants
The first group consisted of 10 healthy participants. The inclusion criteria were: (1) age >20 y; (2) no history of smoking; and (3) body mass index <30 kg/m2. The exclusion criteria were: (1) history of a respiratory disorder; (2) history of respiratory trauma; (3) history of scoliosis; and (4) history of a neurological disorder.
The second group of participants consisted of 10 subjects with Duchenne muscular dystrophy. The inclusion criteria were: (1) diagnosed with Duchenne muscular dystrophy by genetic testing; (2) Cobb angle >10°; and (3) body mass index <30 kg/m2. The exclusion criteria were: (1) diagnosis of exacerbation of chronic respiratory failure due to acute pneumonia at that moment; and (2) the subject could not understand instructions due to mental disability.
Healthy participants were recruited from the staff of Higashi-Saitama National Hospital as volunteers. The subjects with Duchenne muscular dystrophy were recruited from the in-patients and out-patients of Higashi-Saitama National Hospital.
The study was approved by the institutional ethics review board (approval 13-49-2), registered with the University Hospital Medical Information Network (UMIN), and was performed after written, informed consent was obtained from the participants and in accordance with the Declaration of Helsinki (UMIN Clinical Trials Registry No. UMIN000018408; http://www.umin.ac.jp/ctr/).
The Measurement System
Figure 1 shows how the RMET measurements were performed using the fiber grating vision sensor system. The system consists of a fiber grating projector, a charge-coupled device camera, and a personal computer for data analysis. The fiber grating projector is composed of a fiber grating element and a laser source, and approximately 800–1000 bright spots were projected onto the surface of the facing object.25

Experimental setup for RMET measurement. RMET = Respiratory Movement Evaluation Tool, PC = personal computer, FG = fiber grating.
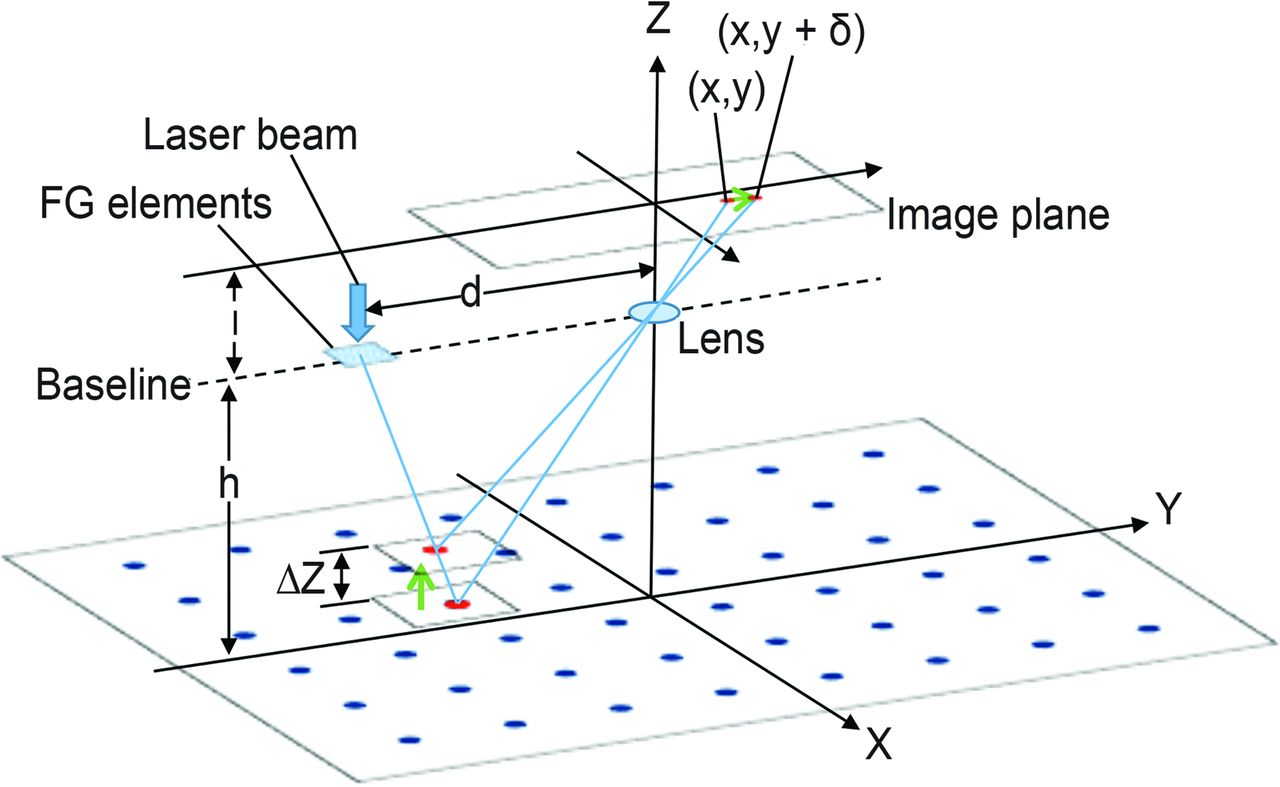
Figure 2 shows an optical pattern diagram of the system. This system calculates the thoracoabdominal displacement along the z axis by recording the movement of bright spots. The figures of bright spots in the image plane move from (x,y) to (x,y+δ) across the baseline following the respiratory movement. Displacement along the z axis is calculated by the formula1 based on the triangulation principle: ΔZ = h2δ/(Dl +hδ) [1]) where δ is the displacement of a bright spot, h is the distance from the plane to the lens, d is the distance from the fiber grating elements and the lens, and l is the distance from the lens to the image plane. The resolution of the displacement along the z axis (ΔZ) is 0.22 mm, which is suitable for precise examination of respiratory movement.

Optical pattern diagram of the fiber grating sensor system. FG = fiber grating, δ = displacement of bright spots, h = the distance from the plane to the lens, d = the distance from the FG elements to the lens; l = the distance from the lens to the image plane.
The participants were asked to wear a prepared T-shirt. A plain cotton T-shirt was used, and female participants were examined with their usual undergarments. The system was designed so that the markers could be placed on the T-shirt to avoid skin damage caused by the marker and also to minimize invasion of privacy. Markers were attached to the T-shirt on the surface of interest of the thorax and abdomen with double-faced adhesive tape and wrinkles were smoothed as much as possible.
The thoracoabdominal body surface was divided into 6 areas using 13 markers on the T-shirt. Thirteen passive markers were placed on the sternal notch, fourth rib on the sternal bone, xiphoid process, umbilical region, middle point of the anterior superior iliac spine, and both sides of the angle of the acromion, axilla, along the midclavicular line in the subcostal region, and the anterior superior iliac spine. The markers were made of acrylic board pasted with a retroreflective material, with a diameter of 30 mm and a thickness of 2 mm.
The light source was used to recognize markers on the T-shirt and draw lines in several seconds to automatically divide the thoracoabdominal body surface into 6 areas at the beginning of the examination. The position of the marker was recognized by searching for a circle that has a certain area. A genetic algorithm was used to decide optical pairs of the dividing lines.
Respiratory amplitude (mm) was defined as the mean values of the z axis migratory distance (ΔZ) of the bright spots on the body surface in each area during respiratory movement. One respiratory cycle was defined as the period from the minimum to the maximum values of the sum of all respiratory amplitudes. Figure 3 shows the RMET output screen. The divided areas were summed appropriately to compare the differences between the left and right parts, the thorax and abdomen parts, and so on. Respiratory amplitudes were monitored continuously and displayed in real time on a personal computer. In addition, the RMET displayed a circle whose size increased commensurately with the respiratory amplitudes. These quantitative respiratory amplitudes and circle information can be used for clinical assessment and feedback to the patients.
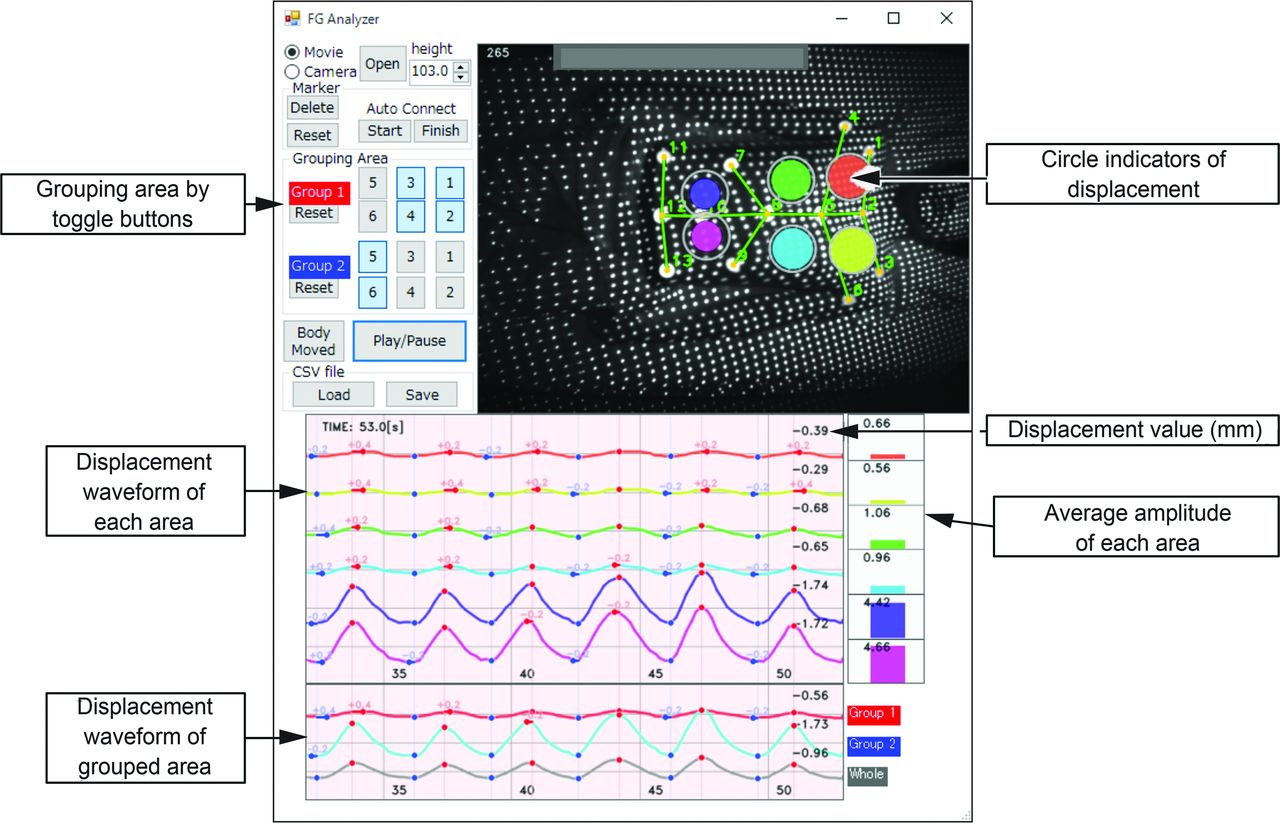
Respiratory Movement Evaluation Tool output scan. The numbers on the bottom show time(s) from the start of the examination. Colored waves show the change in respiratory amplitude of each divided area, and the displacement values (mm) are displayed in real time. Numbers on the right side show the mean of the respiratory amplitudes of each divided area, which is calculated in real time and presented as a colored bar. Colored circles show visual movements of each area. All divided areas are added to one another as grouped areas.
A preliminary evaluation was performed to compare the RMET measurements between T-shirt and naked skin in order to examine errors caused by wrinkles in the T-shirt in 10 healthy subjects using a Bland-Altman plot. There was no bias making a gradient in the plot between the 2 conditions. For the usual breathing, the difference in the respiratory amplitude was not significant (correlation coefficient 0.32, P = .36) (unpublished data). For maximum breathing, the difference in the respiratory amplitude was not significant (correlation coefficient 0.18, P = .61) (unpublished data).
Feasibility of the Respiratory Movement Measuring Instrument
The time needed for measurement of respiratory movements with the RMET was determined in 10 healthy subjects. Time measurement included: (1) starting the RMET personal computer; (2) attachment of the markers to the T-shirt on the surface of interest of the thorax and abdomen with double-faced adhesive tape; (3) instruction to participants about the measurement; (4) measurement of 1 min of breathing at rest and 3 maximum breaths with the subject in a comfortable supine position; and (5) removal of the markers and finishing the test.
For assessing satisfaction with different aspects of the RMET, the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) 2.0 was used,27 which comprises 12 satisfaction items, such as “easy to use” and “effectiveness.” Three items (repairs and servicing, professional service, follow-up services) were not appropriate for the evaluation of the RMET and, thus, were removed from the questionnaire. Five clinicians who assessed respiratory movement using the RMET system were asked to complete the QUEST 2.0 questionnaire. Clinicians answered the questionnaire immediately after using the device.
Reliability and Validity
Chest wall movement was measured 3 times in 10 healthy subjects with the RMET to test inter- and intra-rater reliabilities. Two of the measurements were performed by the same examiner, and one measurement was performed by a different examiner. The order of the measurements in each session was randomized.
The participants were asked to perform 1 min of spontaneous breathing and 3 maximum breaths in a comfortable supine position. During the measurements of spontaneous breathing, the participants were instructed to rest comfortably and breathe as usual. In maximum breathing, they were told to continuously perform 3 maximum breaths. The respiratory amplitudes of each divided area were calculated based on the average values of 1 min of spontaneous breathing and the maximal values of the 3 maximum breaths.28 Examiners included 6 physical therapists, 3 occupational therapists, and 1 medical doctor, including the authors. The participants were asked to walk a few minutes between the measurements and then return to the supine position. The markers were again placed on the defined points.
In addition, 5 healthy subjects underwent RMET measurement simultaneously with spirometry measurements to test its validity. From spontaneous breathing to maximum breathing, the subjects were encouraged to breathe 10 times while voluntarily changing the amount of air during ventilation in a comfortable supine position. For example, the first breath was spontaneous breathing at rest, the second was a slightly deeper breath, and the third was much deeper. The tenth breath was maximum breathing. A spirometer was used to record the volume of each respiration. This method was based on a previous study.26 The SP-370COPDhyper (Fukuda Denshi, Tokyo, Japan) with a nose clip and a mouthpiece was used for spirometry measurements.
The same measurements as in healthy subjects were performed in 10 subjects with Duchenne muscular dystrophy to test its reliability. Between measurements, the subjects sat in their wheelchair for a few minutes, then returned to a comfortable supine position, and the markers were placed on the defined points. The angles of hip flexion and knee flexion were measured with the subject in the supine position to confirm that they were in the same posture. Five subjects with Duchenne muscular dystrophy performed simultaneous spirometry measurements to test its validity, in the same manner as the healthy subjects.
Statistical Analyses
Inter- and intra-rater reliabilities were assessed using ICC Equations 1,1 and 2,1.29 The standard error of the mean was calculated using the formula SEM = SD/√2. To assess the validity of the RMET, the sum of 6 areas of the RMET respiratory amplitudes, and the amount of air during ventilation measured with a spirometer were divided by each maximum value. These values were defined as %RMET and %volume, respectively, and their correlations were assessed with Pearson's product-moment correlation coefficients. Statistical analyses were performed using statistical software (SPSS Statistics 22.0, IBM, Armonk, New York). The degree of correlation in this study was defined as: poor (r < 0.40), fair (r = 0.40–0.75), and excellent (r > 0.75) for ICC,30 and that for Pearson's correlation coefficients was defined as: low (r < 0.50), moderate (r = 0.50–0.70), and high (r > 0.70).31 Values of P < .05 were considered significant.
Results
Table 1 shows the demographic features of the healthy subjects and the subjects with Duchenne muscular dystrophy. Table 2 shows the clinical features of the subjects with Duchenne muscular dystrophy.
Demographic Features of Healthy Subjects and Subjects With Duchenne Muscular Dystrophy
Clinical Features of Subjects With Duchenne Muscular Dystrophy
Feasibility of the Respiratory Movement Measuring Instrument
With RMET, real-time recordings of thoracoabdominal movements of the 6 divided areas were obtained with mean ± SD values of 374 ± 23.9 s in 10 healthy subjects, beginning from start-up of the RMET to the end of the test. The measurement was well tolerated by the participants, and no discomfort or adverse effects were reported. Five healthy subjects were measured in the rehabilitation room, and 5 were at the out-patient department. Five subjects with Duchenne muscular dystrophy were measured in the rehabilitation room, 3 were at the out-patient department, and 2 were at the bedside.
Table 3 shows the most important items and the median values of items mentioned by the clinicians using the QUEST 2.0 questionnaire. All clinicians stated that the most important system feature was effectiveness, 4 clinicians answered “easy to use,” 3 clinicians answered safety, and 1 clinician answered “adjustments,” “dimensions,” and “weight.” The median score of each item exceeded 3 (more or less satisfied).
Quest 2.0: Most Important Items and Median Values of Items Mentioned by 5 Clinicians
Reliability and Validity
Tables 4 and 5 show inter- and intra-rater reliabilities during usual breathing and maximum breathing in healthy subjects. For usual breathing, the ICC(1,1) as intra-rater reliability, were 0.90–0.99, with SEM values of 0.04–0.35 mm. The ICC(2,1) values, as inter-rater reliability, were 0.83–0.97, with SEMs of 0.06–0.18 mm. For maximum breathing, the ICC(1,1) values were 0.82–0.93, with SEMs of 0.70–1.55 mm. The ICC(2,1) values were 0.83–0.93, with SEMs of 0.76–1.28 mm. All ICCs exceeded 0.75, an excellent level of correlation.
Reliability of the Respiratory Movement Evaluation Tool in 10 Healthy Subjects During Usual Breathing
Reliability of the Respiratory Movement Evaluation Tool in 10 Healthy Subjects During Maximum Breathing
In healthy subjects, significant and positive correlations were observed between the respiratory amplitudes measured with RMET and the amounts of air during ventilation measured with a spirometer (r = 0.995, P < .001) (Fig. 4). The value of r exceeded 0.70, a high level of correlation.

The relationship between volume and Respiratory Movement Evaluation Tool (RMET) percentage in 5 healthy subjects. Volume % = (amount of air during ventilation measured by spirometer/maximum amount of air during ventilation measured by spirometer) ×100, RMET % = (sum of the RMET respiratory amplitudes of each divided area/the maximum sum of the RMET respiratory amplitudes of each divided area) × 100.
Tables 6 and 7 show inter- and intra-rater reliabilities during usual breathing and maximum breathing in subjects with Duchenne muscular dystrophy. For usual breathing, the ICC(1,1) values were 0.87–0.96, with SEMs of 0.10–0.26 mm. The ICC(2,1) values were 0.84–0.97, with SEMs of 0.10–0.19 mm. For maximum breathing, the ICC(1,1) values were 0.91–0.97, with SEMs of 0.27–0.47 mm. The ICC(2,1) values were 0.89–0.99, with SEMs of 0.21–0.49 mm.
Reliability of the Respiratory Movement Evaluation Tool in 10 Subjects With Duchenne Muscular Dystrophy During Usual Breathing
Reliability of the Respiratory Movement Evaluation Tool in 10 Subjects With Duchenne Muscular Dystrophy During Maximum Breathing
The respiratory amplitudes measured with the RMET were significantly and positively correlated with the amount of air during ventilation measured with a spirometer in subjects with Duchenne muscular dystrophy (r = 0.957, P < .001) (Fig. 5).
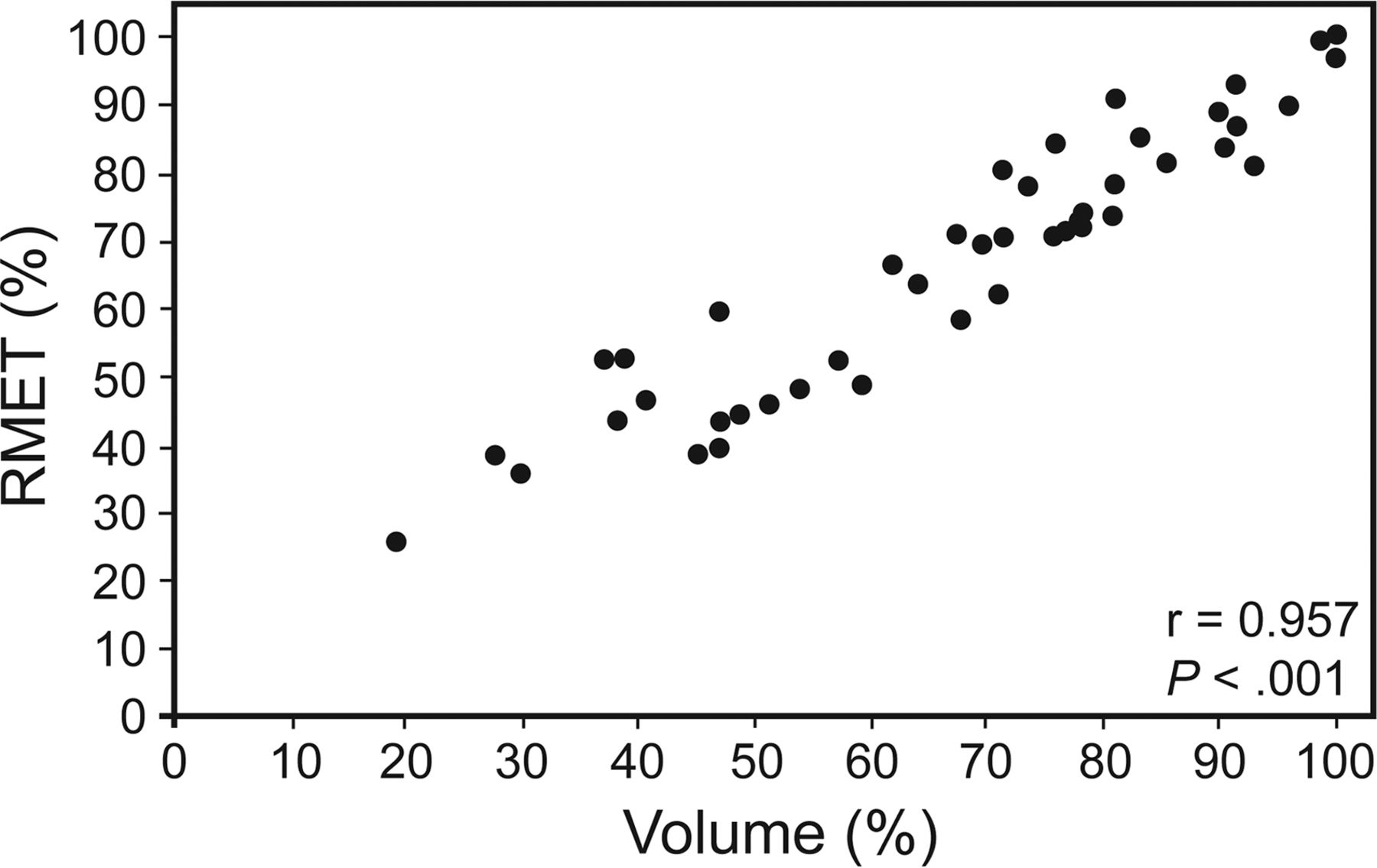
The relationship between volume and Respiratory Movement Evaluation Tool (RMET) in 5 subjects with Duchenne muscular dystrophy. Volume % = (amount of air during ventilation measured by spirometer/maximum amount of air during ventilation measured by spirometer) × 100. RMET % = (sum of the RMET respiratory amplitudes of each divided area/ the maximum sum of the RMET respiratory amplitudes of each divided area) × 100.
Discussion
We developed a novel method using fiber grating sensors to assess thoracoabdominal movement in neuromuscular diseases, called the RMET. Measurement with the RMET was feasible, reliable, and valid in healthy subjects and in subjects with Duchenne muscular dystrophy.
The measurement can be accomplished in a short period starting from equipment preparation. The time needed for measurement was around 6 min, and this seems acceptable in daily clinical practice. Because of its portability and easy setup, the RMET can be used in various places. In addition, the QUEST 2.0 questionnaire showed that clinicians scored the RMET as 4 (quite satisfied) for “effectiveness” and “easy to use,” which is an acceptable level of satisfaction.
The RMET demonstrated satisfactory inter-and intra-rater reliabilities. Most of the ICCs exceeded 0.75, an excellent level of reliability. It also had significant correlations with spirometer measurements in healthy subjects. Reliability of the optoelectronic plethysmography method in healthy subjects has been reported, with ICC(1,1) and ICC(2,1) being >0.75,22,23 and its validity has been confirmed, with sufficient linear correlations with the amount of air during ventilation measured by spirometer.22 Therefore, although it was a small sample size, the RMET had equivalent reliability and validity compared with that of optoelectronic plethysmography.
Furthermore, measurement with the RMET in subjects with Duchenne muscular dystrophy, who had spinal and thoracic deformities and whose respiratory movements were small,6 had comparable reliability and validity to measurement in healthy subjects. Therefore, the RMET is feasible for evaluating thoracoabdominal movements in neuromuscular diseases.
This study has several limitations. First, the participants were limited to healthy subjects and subjects with Duchenne muscular dystrophy with a normal or low BMI. Although Duchenne muscular dystrophy can be regarded as representative of restrictive ventilatory disorders brought about by respiratory muscle weakness and spinal deformities, application of the RMET to other neuromuscular disorders and obese people should be examined in future studies. In addition, further studies are needed to examine different impairments of lung mechanics, such as in restrictive and obstructive diseases. Second, although sufficient reliability and validity were demonstrated, the sample was small, and a sample size analysis was not performed. In addition, we have not yet examined responsiveness to treatment interventions and longitudinal changes with time. Further studies are needed to investigate the measurement properties of the RMET, including reliability, validity, and responsiveness testing, according to the COSMIN (Consensus-based Standards for the Selection of Health Status Measurement Instruments).32 Third, the method can have errors brought about by wrinkles, because respiratory movement was examined with and without the subject wearing a T-shirt. However, we must consider the trade-off between accuracy of measurement and comfort of the patient and ease of measurement. The fourth limitation is the absence of blinding of the assessors. Lastly, the measurement was performed with the subject only in the supine position. Breathing pattern evaluation in the sitting position would provide us with more insight into respiratory mechanics in daily life. Despite these limitations, the data presented in this study provide the basis for designing and conducting a larger scale trial with a more rigorous study design to test the hypothesis that the RMET has satisfactory reliability, validity, and responsiveness for assessing thoracoabdominal movements in neuromuscular and other diseases.
Conclusions
The RMET is feasible for use in daily clinical practice. Further studies are needed to investigate the measurement properties of the RMET and its applications for neuromuscular and other diseases.
Acknowledgments
We thank the participants in this study for their cooperation, as well as Drs Atsuko Anzai and Yuka Yamada; physical therapists Kento Kaneko, Yo Takino, and Kaoru Noguchi; and occupational therapist Koki Tairaku for their contribution to recruitment of the participants and data collection. The authors are also very grateful to the clinical laboratory center for assistance in data collection. The authors also acknowledge Dr Yohei Otaka and Dr Katsuhisa Ogata for their contribution to the manuscript and biostatistician Takayuki Abe for his contribution to statistical analysis.
Footnotes
- Correspondence: Meigen Liu MD PhD, Department of Rehabilitation Medicine, Keio University School of Medicine, 35 Shinanomachi, Shinjuku-ku, Tokyo 160-8582, Japan. E-mail: meigenliukeio{at}mac.com.
This study resulted from an “Innovation Venture Assist Project by New Energy and Industrial Technology Development Organization (NEDO), Japan.” The fiber grating sensor machine was supplied by Ideaquest Inc.
Dr Aoki has disclosed a relationship with Ideaquest Inc. Drs F Liu, Kawakami, Tsuji, Otsuka, Miyata, Tashiro, Wada, Mizuno, M Liu, and Mr Tamura, Mr Taki, and Mr Shimizu have disclosed no conflicts of interest.
- Copyright © 2017 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}