

Abstract
BACKGROUND: Cardiovascular collapse is a life-threatening event after unplanned extubations (UEs) in the pediatric ICU (PICU). However, there is a paucity of pediatric studies assessing this complication. We sought to assess the incidence, risk factors, and outcome of cardiovascular collapse after UEs in PICU patients.
METHODS: All children who had been mechanically ventilated for ≥12 h were prospectively tracked for UEs over an 8-y period. Subjects were included in the study if they were between ages 1 month and 16 y and had experienced UE. They were analyzed in 2 groups: those with cardiovascular collapse (defined as the need for cardiopulmonary resuscitation or circulatory dysfunction immediately after UE) and those with no cardiovascular collapse.
RESULTS: Of the 847 subjects, 109 UEs occurred in 14,293 intubation days (0.76 UEs/100 intubation days), with 21 subjects (19.2%) experiencing cardiovascular collapse, of which 10 required cardiopulmonary resuscitation. Compared with subjects without cardiovascular collapse after UE, children with cardiovascular collapse were younger (<6 months old), with respiratory failure from lower respiratory tract diseases, lower PaO2/FIO2 (218 vs 282 mm Hg), and higher oxygenation indices (5.5 vs 3.5) before UE events. Logistic regression revealed that only an age ≤6 months old was strongly associated with cardiovascular collapse (odds ratio 3.4, P = .03). There were no differences between cardiovascular collapse and non-cardiovascular collapse subjects regarding the length of hospital stay, ventilator-associated pneumonia rate, and mortality.
CONCLUSIONS: Cardiovascular collapse is a frequent complication of UEs, particularly in the youngest children. Specific bundles to prevent UEs may reduce morbidity related to these events.
Introduction
Unplanned extubation (UE) is the commonest airway incident in the intensive care setting, and it is associated with complications such as hypoxemia, hypotension, arrhythmias, hypercarbia, need for emergency re-intubation, and, rarely, death.1,2 In the pediatric population, UE has been associated with prolonged mechanical ventilation and pediatric ICU (PICU) and hospital stays and increased cost, but it has not been associated with higher mortality.3,4
Because of the limited cardiorespiratory reserve, critically ill patients may not be able to compensate for additional injury. This population is accordingly susceptible to the adverse consequences of critical incidents.2,5 Cardiovascular collapse can be a potential life-threatening complication after UEs. In adults, Mort6 found a high rate of hemodynamic complications (72%) associated with UE events. Likewise, in a population mainly consisting of newborns (62% of patients), Klugman et al7 assessed morbidity in UE children and found that 1 in 5 subjects exhibited cardiovascular collapse after UE and that most of them required cardiopulmonary resuscitation. These authors assessed subjects admitted to the neonatal, pediatric, and cardiac ICU, so it is possible that the results from these studies cannot be directly extrapolated to the PICU population.
Reported rates of UEs and their complications may be underestimated unless a prospective, specific collection tool is utilized. To date, no study has specifically analyzed the incidence, risk factors, and outcomes associated with cardiovascular collapse following UE in the PICU setting. Given that cardiovascular collapse represents a catastrophic event, the early identification of high-risk patients for cardiovascular events may enable close monitoring of these patients (eg, during manipulation/procedures) and facilitate a more efficient allocation of nurses' time to those children who require temporarily intensified surveillance. Furthermore, determining the frequency of cardiovascular collapse in PICU patients may support further efforts to decrease the rate of UE, even for those PICUs that have historically achieved low UE rates.
Hence, the aim of this study was to determine the incidence of cardiovascular collapse after UE and to identify risk factors predicting hemodynamic deterioration after UE. Secondarily, we assessed the outcomes of these subjects compared with those UE subjects without cardiovascular collapse events.
QUICK LOOK
Current knowledge
Unplanned extubation is the most common airway incident in the ICU; however, there remains a paucity of data related to the cardiovascular morbidity associated with these events in critically ill children.
What this paper contributes to our knowledge
We studied the incidence and risk factors associated with cardiovascular collapse following unplanned extubations in the PICU. Nineteen % of cardiovascular morbidity was associated with unplanned extubations, and cardiovascular collapse was more frequent in younger children.
Methods
Study Design and Setting
This non-concurrent prospective cohort study included subjects receiving ventilation from January 1, 2008, through July 31, 2016, who were admitted to an 8-bed PICU of a tertiary hospital. The PICU was not designed to handle specialist congenital heart surgery or burn cases, and bone marrow and solid organ transplants were not performed at the hospital. The local institutional review board approved the study and waived the need for informed consent from the children's parents.
The study population included all consecutive subjects admitted to the PICU with ages between 1 month and 16 y who required invasive mechanical ventilation for ≥12 h. Subjects with tracheostomy were excluded. The nurse/patient ratio was 1:2. All of the subjects had undergone orotracheal intubation, and the method of securing the tracheal tubes was standardized using the same type of adhesive tape. Based on recommendations of the American College of Radiology,8 we did not perform daily routine chest radiographs. Respiratory therapists monitored the position of the endotracheal tube at the lip at least once per shift to detect any short displacements and adjust the endotracheal tube position when required.
Data Collection
Data were extracted from a prospectively maintained database designed to register information of all planned and unplanned extubations in the PICU. This database is part of our continuous quality improvement program to monitor and reduce UE events.9 Potential risk factors for UEs were assessed based on a data collection tool, which comprised patient characteristics, circumstances of the extubation, and outcomes. Any missing data were added by interviewing the nurse who witnessed or discovered the UE. Additional information was retrieved from subject records. All of the data were reviewed on a daily basis and transcribed with double entry by the primary investigator (PSL) into a specifically designed computer database.
The demographic and clinical variables collected included age, sex, weight, PICU admission diagnosis, and severity of illness at PICU admission as measured by the Pediatric Risk of Mortality II10 and Pediatric Logistic Organ Dysfunction scores.11 We also recorded the level of sedation before extubation (COMFORT score),12 use of physical restraints, total duration of mechanical ventilation, length of the PICU and hospital stays, and ventilator-associated pneumonia rate. The following laboratory data were collected for the last recorded data point before the UE: arterial blood gas values (pH, PCO2, and PO2), PaO2/FIO2, and oxygenation index (mean airway pressure × FIO2/PaO2 × 100).
Subjects were considered to be at the weaning phase if they fulfilled the following criteria: improvement or resolution of the underlying disease, in possession of spontaneous respiratory effort; gag or cough with suctioning, acceptable level of consciousness for extubation, no vasopressor or inotrope medication other than low-dose dopamine or dobutamine (<5 μg/kg/min), pH of 7.32–7.47 on most recent blood gas analysis, FIO2 ≤ 40%, PEEP ≤ 8 cm H2O, and plateau pressure ≤ 25 cm H2O. Once the decision to extubate had been made, subjects were considered ready for extubation if they tolerated ≥30 min of minimal ventilator support defined as follows: (1) CPAP of 5 cm H2O or (2) pressure support ventilation adjusted for the endotracheal tube size because of the increasing resistance with narrower endotracheal tube (3.0–3.5 mm = pressure support of 10 cm H2O, 4.0–4.5 mm = pressure support of 8 cm H2O, ≥5 mm = pressure support of 6 cm H2O).13–15 The weaning management and the final extubation decision were made at the discretion of the attending physician. Sedation and analgesia levels were assessed by nurses every 4 h using the COMFORT scale (range: 8–40)12 and the FLACC (face, legs, activity, cry, consolability scale) (range: 0–10),16 respectively. Subjects were kept within the desired sedation level (COMFORT score ≥17 and ≤26) while receiving mechanical ventilation. A COMFORT score of <17 implied oversedation, and a score of >26 defined undersedation.12 Noninvasive ventilation or supplemental oxygen was initially attempted in those UE subjects who did not require emergency re-intubation. The attending physician made the decision of either re-intubation or noninvasive ventilation administration.
Definitions
Unplanned extubation was defined as any displacement of the endotracheal tube from the trachea when a provider did not deliberately remove it. Re-intubation was defined as replacement of the endotracheal tube within 24 h of UE.3 The following semi-quantitative scale evaluated the amount of endotracheal secretions: no secretions/minimal secretions (suctioning required every 2–4 h), moderate secretions (suctioning required every 1–2 h), or copious secretions (suctioning required several times/h).17
Determinants of UEs included both subject- and caregiver-related reasons. Reasons related to subjects encompassed restlessness, agitation, and self-extubation (subject's deliberate action). Reasons related to caregivers involved poor fixation of endotracheal tube, bedside procedures, nursing care, or any other manipulation of the child.
Nurses and respiratory therapists continuously assessed the integrity/cleanliness of the adhesive tape. In fact, poor tube fixation was reported more frequently before UE. Inappropriate or poor fixation was determined based on the presence of significant mobility of the tubes or loose and/or grossly contaminated (ie, slimy or wet) tape securing the tube. Ventilator-associated pneumonia was defined according to the Centers for Disease Control and Prevention and the National Healthcare Safety Network.18
Cardiovascular collapse was defined as the need for cardiopulmonary resuscitation (eg, external chest compressions for ≥2 min) or cardiovascular dysfunction (hypotension and/or ≥2 signs of poor perfusion requiring a fluid challenge of ≥20 mL/kg of crystalloid solution and/or necessitating introduction of vasoactive support and/or an increased requirement of vasoactive drugs) within 1 h following the UE event. Moreover, hypotension was defined as systolic blood pressure above the 5th percentile (<70 mm Hg in infants; 70 + [age in years × 2] after 1 y of age), whereas signs of poor perfusion included decreased peripheral pulse volume, capillary refill time of ≥3 s, central peripheral temperature gradient >3°C, mottled or cool extremities, and increased lactate (>2 mmol/L).
Study Outcomes
The primary outcome variable for the analysis was the occurrence of cardiovascular collapse after UEs. We secondarily assessed the incidence and risk factors for cardiovascular collapse after UE events.
Statistical Analysis
Descriptive statistics were performed for all of the variables. The results are expressed as n (%) for categorical variables and as median (interquartile range) for continuous variables. The median difference and 95% CI was calculated when appropriate. Comparisons between cardiovascular collapse and non-cardiovascular collapse groups were based on the Mann-Whitney U test for continuous variables and the chi-square test for categorical variables or Fisher exact test if one expected that the cell value would be <5 (categorical variables). A stepwise unconditional logistic regression analysis was performed with cardiovascular collapse as the dependent variable. All of the variables in the univariate analysis with P < .05 were included as independent variables, as well as additional variables chosen a priori and considered of clinical relevance, such as younger children (<6 months)7 and respiratory failure due to lower respiratory tract disease.6 Variables thought to be collinear were not included simultaneously in the model if the variance inflation factor was not >1.0. All of the statistical tests were 2-tailed, and P < .05 was considered to be statistically significant. The data were analyzed using SPSS 16.0 (SPSS, Chicago, Illinois). A power analysis was not performed due to the limited information available from previous pediatric studies and differences in the definition of cardiovascular collapse after UE.
Results
Demographics and Clinical Characteristics
During the study period, a total of 847 subjects required 14,293 mechanical ventilation days (median 8.2 d; range 5.4–15.2 d). From this population, 90 subjects (10.6%) experienced 109 UE events (Fig. 1), resulting in a rate of 0.76 UEs/100 intubation days.
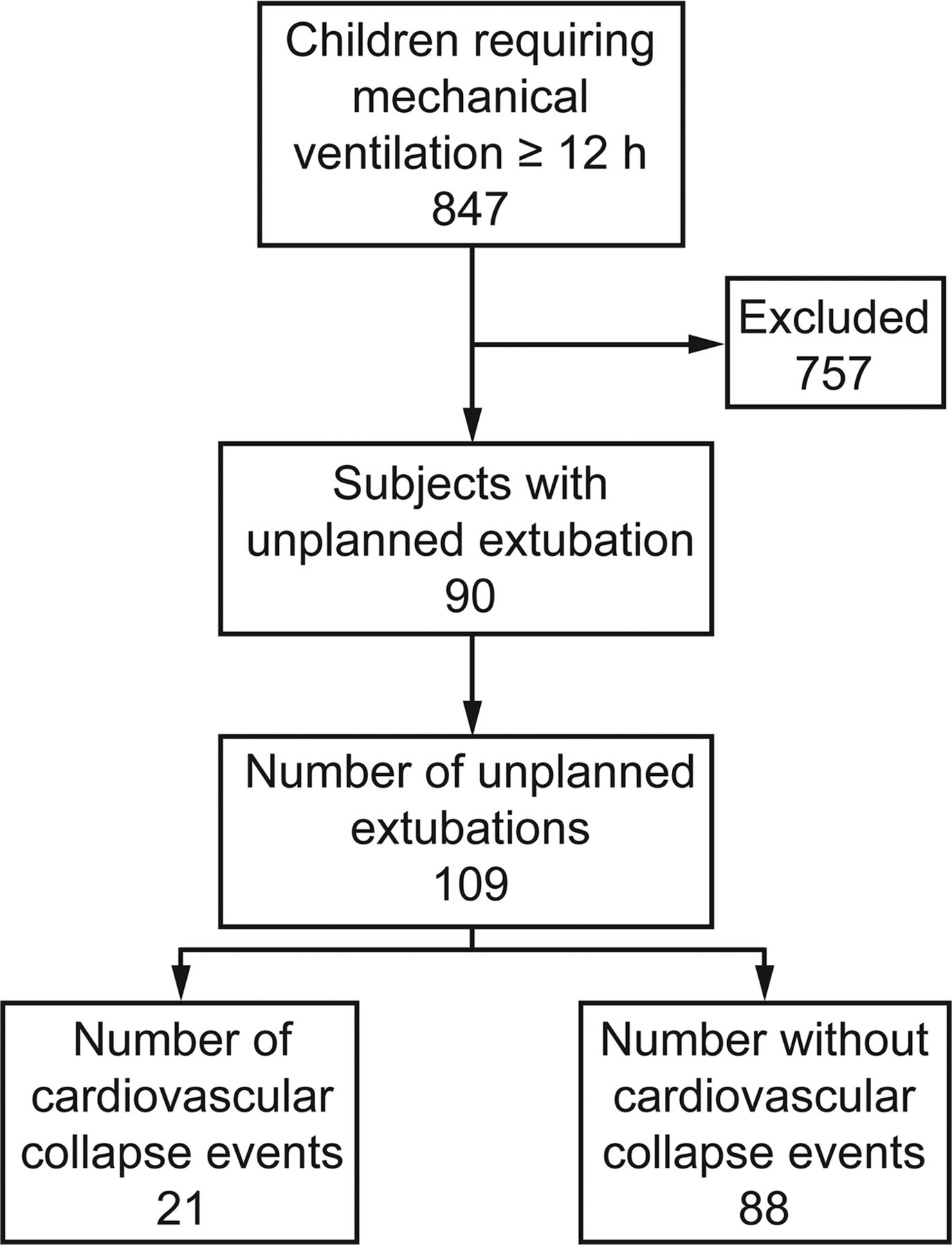
Flow chart.
Cardiovascular collapse occurred in 21 events (19.2%), of which 10 required the initiation of cardiopulmonary resuscitation. Table 1 lists the UE event characteristics sorted by the presence or absence of cardiovascular collapse. Only 18 subjects (16.5%) were weaning from mechanical ventilation, all of them non-cardiovascular subjects; 7 subjects were on a spontaneous breathing trial.
Demographics and Clinical Characteristics
The overall rate of re-intubation following UEs was 69%. Of the 88 UE events in the non-cardiovascular collapse group, 54 (61%) required re-intubation. All subjects experiencing cardiovascular collapse following UE required re-intubation within 15 min of the UE. Of note, 6 subjects (28.5%) in the cardiovascular collapse group were re-intubated before developing cardiovascular collapse. Reasons for re-intubation in the non-cardiovascular collapse group included hypoxemic respiratory failure (n = 34), increased work of breathing (n = 12), upper airway obstruction (n = 5), and decreased level of consciousness (n = 3). Of the 75 re-intubations, 90% were within 15 min of UE. Among the non-cardiovascular collapse subjects, 85% were re-intubated within 2 h of UE (46 subjects within 15 min, 3 subjects within 15–30 min, and 2 subjects within 1–2 h), whereas the 3 remaining subjects were re-intubated within 6–12 h. A total of 83 subjects received sedative agents within 2 h before UE events, 15 subjects (18%) were in the cardiovascular collapse group, and 68 subjects were in the non-cardiovascular collapse group (82%). Furthermore, 3 subjects were receiving neuromuscular blocking agents at the UE event (2 cardiovascular collapse subjects and one non-cardiovascular collapse subject). Reversal agents (naloxone and/or flumazenil) were administered to 5 subjects in the non-cardiovascular group, and 2 of these subjects did not require re-intubation.
Risk Factors for UE With Cardiovascular Collapse
Univariate analysis revealed that risk factors for cardiovascular collapse included subject age (children ≤6 months old), acute respiratory failure as a reason for PICU admission, poorer values of oxygenation measures (FIO2, PaO2/FIO2, and oxygenation index) before the UE events, and higher ventilator settings (breathing frequency and FIO2) (Table 1). In fact, weaning subjects were more likely to tolerate UE events without experiencing cardiovascular collapse (P = .02).
Table 1 shows the COMFORT score of the subjects experiencing UE; the median value is 22. Forty-seven subjects (43%) were considered agitated. It is noteworthy that the median COMFORT score differed between subjects who were agitated and those who were not (25 vs 18.5, P < .005). Considering a COMFORT score of <27, there was no difference in the proportion of subjects with cardiovascular collapse compared with those without (71.4% vs 69.3%, P = .84). By categorical age group, there was no difference in the median (interquartile range) COMFORT score between subjects <6 months old and those who were older (21 [16–26] vs 23.5 [17–29], P = .062). Still, there was no difference between the median COMFORT score in children <6 months old (18 [14–26]) versus older children (21 [16–26]) (P = .72) who experienced cardiovascular collapse. Using logistic regression, we analyzed the relation between specific independent variables and cardiovascular collapse after UEs (Table 2). The model revealed that an age ≤6 months old (odds ratio 3.4) was the only independent risk factor associated with cardiovascular collapse after UE. Furthermore, the performance for an age ≤6 months old exhibited a sensitivity of 76.2% (95% CI 52.4–90.8%), a specificity of 55.6% (95% CI 44.7–66.1%), a positive predictive value of 29% (95% CI 18.1–43.1%), and a negative predictive value of 90.7% (95% CI 78.9–96.5%).
Logistic Regression Model Predicting Cardiovascular Collapse After Unplanned Extubation
Outcomes of Subjects With Cardiovascular Collapse After UE
There were no differences between subjects who experienced cardiovascular collapse after UE and those who did not in terms of the overall duration of mechanical ventilation, length of PICU and hospital stays, and ventilator-associated pneumonia rate (Table 3). There additionally was no difference in mortality between the groups.
Subject Outcomes
Discussion
Our cohort analysis revealed that UEs were associated with substantial cardiovascular morbidity. Exploratory analyses showed that only an age ≤6 months old was associated with cardiovascular collapse following UE events. Additionally, subjects with cardiovascular collapse had outcomes similar to those of subjects without cardiovascular collapse, including a lack of impact on mortality.
The cardiovascular collapse rate (19%) observed in our study cohort was similar to that reported previously in children and neonates (20%).7 However, we found that 10 of our subjects (47%) required cardiopulmonary resuscitation; Klugman et al7 reported an even higher frequency of 83%. Some differences between our study and that of Klugman et al7 may explain these discrepant results. First, that study assessed subjects from the cardiac ICU, PICU, and neonatal ICU. We evaluated only PICU subjects. Therefore, it is possible that the rate of cardiovascular collapse might be even higher in PICUs with subspecialty populations, such as children undergoing cardiac surgery. Second, these authors reported that the highest rate of cardiovascular collapse (54%) occurred in preterm infants. In contrast, we did not include current neonatal ICU subjects in our study. Finally, Klugman et al7 may have used a different definition for circulatory dysfunction for cardiovascular collapse. In fact, there is not a specific definition for cardiovascular dysfunction in that study. Although our overall UE rate was consistent with contemporaneous UE rates19,20 as well as the target upper rate suggested by a pediatric literature review,3 the high frequency of cardiovascular morbidity in UE subjects highlights the seriousness of these adverse events. This high frequency should be considered in efforts to achieve lower benchmark rates.
Although our study found no difference in the median age between the cases of UE with cardiovascular collapse and those without cardiovascular collapse, we observed that nearly half of our UE subjects were ≤6 months old. This high prevalence of infants 6 months old or younger may have impacted the proportion of subjects experiencing cardiovascular collapse events. Actually, there have been conflicting reports about the association between age and UE, and several studies have demonstrated that younger subjects are at higher risk for UE.9,20,21 However, other studies have shown no association.19,22 We found that the youngest children had an odds ratio of cardiovascular collapse of 3.4. However, the performance for age <6 months showed modest sensitivity and low specificity. Nevertheless, consistent with a previous study7 evaluating cardiovascular collapse in children and neonates, our study reinforces the high risk of cardiovascular collapse in the youngest children experiencing UE.
Acute respiratory failure has been identified as a risk factor for cardiovascular collapse and for complications related to emergent intubation and re-intubation due to the limited physiologic reserve secondary to limitations in oxygen transport, alveolar volume, and enhanced shunt fraction.5 There are also studies that have demonstrated oxygenation index cutoff values of five23 and six24 being associated with extubation failure in children. However, our findings showed that a similar threshold (ie, oxygenation index = 5.5) was not associated with cardiovascular collapse after UE.
We should emphasize that Pediatric Risk of Mortality and Pediatric Logistic Organ Dysfunction scores are good surrogates for illness severity and are well correlated with patient mortality. We did not find that these scores were risk factors for cardiovascular collapse in our study. Given that these scores were recorded upon admission, it is possible that during the course of PICU stay, subjects with lower severity scores may have clinically deteriorated before UE events, a situation that in turn might have impacted the occurrence of cardiovascular collapse.
Some studies have associated cardiovascular collapse with increased morbidity and mortality.5,6 However, we found that there were no differences in outcomes, including mortality, between subjects with cardiovascular collapse and those subjects without cardiovascular collapse after UEs. Prompt re-establishment of the airway has been described to reduce the risk of mortality and morbidity associated with extubation failure.25 Therefore, rapid and timely re-intubation may have reduced the risk of death and significant organ damage.25
In a previous study,7 researchers showed that 43% of children who did not have cardiovascular collapse remained extubated. Likewise, we found that 39% of these subjects did not require re-intubation; all of them were weaning from mechanical ventilation. A delay in extubation after having planned weaning has been postulated as a contributing factor in up to one half of UE events.21 Whereas this finding suggests that there may have been missed opportunities to identify extubation readiness in this subgroup, increasing the risk of a UE event, the potential for cardiovascular morbidity in patients not weaning from mechanical ventilation provides insights into implementing strategies to avoid UE events in these patients.
Although not statistically significant, we should note that a high proportion of subjects had UE with cardiovascular collapse caused by some activity related to health-care providers. Most of these activities were due to either nursing or medical manipulation (23%) or endotracheal tube care (25%). A literature review on UEs3 found that the rates of UEs related to patient procedures and endotracheal tube care varied between 49 and 67% and between 36 and 78%, respectively. Hence, our finding creates room for the implementation of a plan of action designed to eliminate or reduce the occurrence of these events. It should be noted that despite the fact that we have been able to achieve a UE rate of <1/100 ventilated days through quality improvement projects and hard work, the challenge to further reduce the rate of UEs related to patient care may be affected by changes in the PICU staff experience, the complexity of patient cases, and unit workflow/turnover, which were not assessed over this 8-y study.
From a clinical perspective, we have identified a population at high risk for developing cardiovascular collapse after a UE. Hence, the youngest children should be taken into account when adjusting patient care, mainly during caregiver activity, to avoid UEs associated with hemodynamic deterioration. Therefore, although not all UEs are harmful, a large number of UEs have the potential to be catastrophic.
The main strength of this study is that it was the first to specifically report the incidence and independent risk factors for cardiovascular collapse after UEs in the PICU. On one hand, current detection systems using self-reporting and administrative coding systems may underdetect serious adverse events; the data quality of the administrative systems often has not been validated.26 On the other hand, all data related to UE events in the present study were part of our continuous quality improvement program specifically addressed to monitor and reduce the incidence of this event.
Nonetheless, the results of our study should be interpreted in the context of a number of potential limitations. First, although observational studies are more appropriate and feasible for evaluating UE, an observational study, like this one, is associated with limitations that are inherent to the study design. These limitations include latent and inadequately controlled confounders due to a lack of randomization. Second, this investigation was a single-center study, and these results may not be generalizable to other centers treating a different patient population, including those with a dissimilar level of acuity. However, our overall incidence of UEs and cardiovascular collapse rate after UEs and contributing factors leading to UEs were all consistent with the current literature.3,7,19,20 Third, our study is limited by the lack of long-term follow-up data to assess the impact of cardiovascular collapse on neurological outcomes. Finally, the lack of pediatric studies properly assessing cardiovascular collapse after UEs limits comparisons, and therefore, additional studies are needed to confirm our findings.
Conclusions
The frequency of cardiovascular collapse is high in children with UEs. An age ≤6 months old was independently associated with cardiovascular deterioration after UE. Although the complete elimination of UEs in PICUs may be an unattainable target, the implementation of appropriate preventive measures may minimize the risk of UEs and decrease ensuing cardiovascular complications.
Footnotes
- Correspondence: Paulo Sergio Lucas da Silva MD MSc, Department of Pediatrics, Pediatric Intensive Care Unit, Hospital do Servidor Público Municipal, Rua Castro Alves, 60, São Paulo 01532-900, Brazil. E-mail: psls.nat{at}terra.com.br.
The authors have disclosed no conflicts of interest.
- Copyright © 2017 by Daedalus Enterprises





{kind=link}