

Abstract
BACKGROUND: We evaluated the outcome of subjects with ARDS in relation to etiology and severity in a retrospective cohort study of the ARDS Network randomized controlled trials. The primary outcome was 28-d mortality. The secondary outcomes were 60-d mortality and ventilator- and ICU-free days. For severity of ARDS, subjects were stratified according to PaO2/FIO2. The etiology of ARDS was classified into sepsis, pneumonia, aspiration, trauma, and others.
RESULTS: A total of 2,914 subjects were included in these trials. Outcomes were modeled with multivariable regressions adjusted for baseline covariates, age, sex, race, Acute Physiology and Chronic Health Evaluation III (APACHE III), vasopressor use, modified lung injury score, diabetes mellitus, cancer status, body mass index, pre-ICU location, ICU location, and study. There was no statistically significant difference in 28-d mortality in relation to ARDS severity. Subjects with trauma, compared with other etiologies of ARDS, had significantly lower mortality at 28 d (odds ratio [OR] = 0.47, 95% CI 0.26–0.83, P = .01). Sixty-day mortality was significantly lower for trauma subjects and those with severe ARDS group (OR = 0.5, 95% CI 0.3–0.85, P = .01 and OR = 0.71, 95% CI 0.52–0.98, P = .034, respectively). There were statistically significantly more ICU-free days and ventilator-free days for the aspiration group (OR = 1.09, 95% CI 1.02–1.17, P = .01 and OR = 1.09, 95% CI 1.02–1.16, P = .01, respectively). There was no statistically significant difference in ICU-free days or ventilator-free days in relation to severity of ARDS.
CONCLUSIONS: Severity of ARDS based on PaO2/FIO2 did not impact 28-d mortality, ventilator-free days, or ICU-free days. Among the etiologies of ARDS, trauma subjects had the lowest 28- and 60-d mortality, whereas subjects with aspiration had more ICU-free days and ventilator-free days.
Introduction
ARDS is a constellation of pathophysiologic changes associated with an early acute lung injury that results in increased capillary leak and pulmonary edema. Clinically, patients manifest with hypoxemia, diffuse radiographic pulmonary infiltrates, and decreased lung compliance. In the United States, it is estimated that there are 150,000 cases of ARDS annually with a mortality of 40–50%.1
There are conflicting results in the literature about the predictors of outcome in patients with ARDS. Factors such as age and the diagnosis of cancer are associated with poor outcome, but not sex, body mass index, diagnosis of diabetes mellitus, or location of the patient.2–4 There are few data on the role of etiology and severity of ARDS upon presentation on different outcomes of patients, and these also show variable results.5–7 The purpose of this study is to analyze the ARDS Network randomized controlled trials database to determine whether etiology and severity of ARDS affected the short-term outcomes of these subjects.
QUICK LOOK
Current knowledge
ARDS remains a major problem in critically ill patients with high mortality. There are conflicting data in the literature about predictors of outcome in subjects with ARDS.
What this paper contributes to our knowledge
Analysis of the ARDS Network robust database shows that severity of ARDS based on PaO2/FIO2 did not predict short-term outcome of these subjects and that trauma was associated with better outcome compared with other causes of ARDS.
Methods
The ARDS Network has conducted several randomized controlled trials to evaluate therapeutic interventions in the management of ARDS. These trials have been previously published.8–13 Table 1 summarizes the relevant features of these trials. Briefly, all subjects fulfilled diagnostic criteria for ARDS and were mechanically ventilated. Similar inclusion and exclusion criteria were used in all of the trials. The National Institutes of Health and the local institutional review boards of each of the sites approved all studies.
Summary of the ARDS Network Trials
We had authorized access to the original data for each of these studies. This paper was prepared using the KARMA (ketoconazole and respiratory management in acute lung injury (ALI)/ARDS), LaSRS (late steroid rescue study), LARMA (lisofylline and respiratory management in ALI/ARDS), ALVEOLI (assessment of low tidal volume and elevated end-expiratory volume to obviate lung injury), FACTT (fluids and catheters treatment trial), and ALTA (albuterol for the treatment of acute lung injury) research materials obtained from the National Heart, Lung, and Blood Institute Biologic Specimen and Data Repository Information Coordinating Center. The primary objective of the KARMA trial was to investigate the efficacy and safety of ketoconazole and respiratory management in the treatment of ALI and ARDS. The ketoconazole arm of the study was later stopped due to an inability to show efficacy. Subjects continued to be randomized to the respiratory management arms of the study (ARMA), which compared 2 ventilator strategies: a tidal volume of 6 mL/kg versus 12 mL/kg (https://biolincc.nhlbi.nih.gov/studies/ardsnet/, Accessed February 27, 2017). The subjects reported in ARMA (N = 861) were a combination of those from KARMA (N = 667) and LARMA (N = 194)8 (https://biolincc.nhlbi.nih.gov/studies/ardsnet/, Accessed February 27, 2017). The findings of the current study do not necessarily reflect the opinions or views of the KARMA, LASRS, LARMA, ALVEOLI, FACTT, and ALTA investigators or the National Heart, Lung, and Blood Institute. For the purpose of this analysis, we included only subjects who had PaO2/FIO2 ≤ 300 to fulfill the Berlin definition of ARDS.14
The 2 variables that we are studying are the severity as well as the etiology of ARDS. The severity was stratified according to PaO2/FIO2 into mild (PaO2/FIO2 = 200–300), moderate (PaO2/FIO2 = 100 to < 200), and severe (PaO2/FIO2 < 100) as per the Berlin definition of ARDS. The etiology was classified based on the original ARDS Network trials' determination into pneumonia, aspiration, trauma, sepsis, and others.
Statistical Analysis
Descriptive statistics for subject baseline characteristics were summarized within each of the 6 studies. The authors made every effort to ensure that each subject was unique and that there were no overlaps between the different studies. Medians with ranges were reported for continuous data, whereas frequencies and percentages were reported for categorical data. The primary objective for our study was mortality at 28 d after enrollment in the study in relation to severity and etiology of ARDS. Covariates in the multivariable regressions included age (< 60 and ≥ 60), sex, ethnicity (white, black, and other), pre-ICU location, type of ICU, Acute Physiology and Chronic Health Evaluation III (APACHE III), vasopressor use, cause of lung injury (pneumonia, sepsis, aspiration, trauma, and others), modified lung injury score, cancer status, body mass index, diabetes mellitus, and study. These variables were specified a priori to be clinically sound or based on our previous publications.2–4 The commonly used measure of acute lung injury score was proposed in 1988 by Murray et al.15 The score is composed of 4 components: (1) chest radiograph; (2) PaO2/FIO2; (3) PEEP; and (4) lung compliance. We proposed the modified lung injury score in this study by excluding the PaO2/FIO2 component. We added individual scores for each category and then divided by the number of components used. Hence, the PaO2/FIO2 was reported independently in our study because it is one of the variables of interest for this work. The secondary clinical outcomes evaluated were 60-d mortality, ventilator-free days, and ICU-free days. The ventilator-free days were defined as the number of days of at least 48-h unassisted breathing during the first 28 d after enrollment.
The univariate analysis of association between our variable of interest, namely severity and etiology of ARDS, and clinical outcomes, including 28-d mortality, 60-d mortality, categorized ventilation-free days in weeks, and categorized ICU-free days in weeks, were performed for statistical significance using a chi-square test or Fisher exact test where appropriate. In-hospital mortality curves for the 3 subgroups of severity of hypoxemia were constructed with the cumulative incidence function method using discharge as competing events.
A multivariable logistic regression model and multivariable zero-inflated negative binomial regression model were then used to evaluate the effect of severity and etiology of ARDS on clinical outcomes, including 28-d mortality or 60-d mortality and ventilation-free days or ICU-free days, respectively. All P values are 2-sided with a significance level of .05. The results of these analyses should be regarded only as exploratory findings, and raw P values were reported without adjustment for multiple testing. All calculations were performed with R 3.2.2.
Results
A total of 2,914 subjects were included in these trials. Five subjects with PaO2/FIO2 > 300 and 2 with missing data were excluded from analysis. Table 2 describes the baseline characteristics of these subjects.
Baseline Subject Characteristics by Study
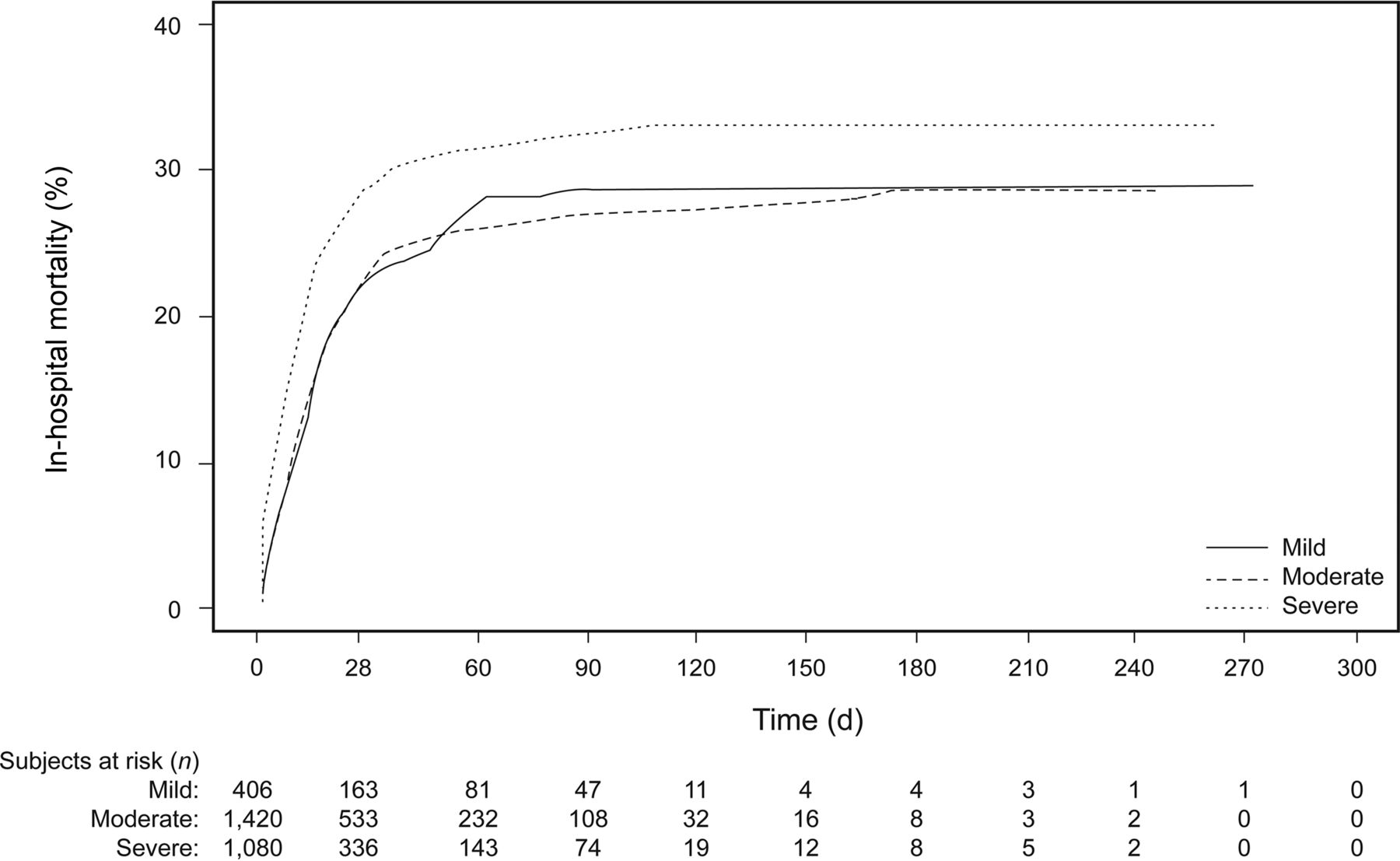
Based on univariate analysis, there were significant differences in 28-d mortality between the different etiologies of ARDS (Fig. 1A). The highest mortality was with sepsis (32.29%), followed by pneumonia (24.91%), other causes (24.14%), aspiration (23.06%), and trauma (8.81%). The differences between these groups were significant (P < .001, chi-square test). Similar associations were observed with 60-d mortality (Fig. 1A). For the severity of ARDS based on PaO2/FIO2, there were significant differences in 28-d mortality, with the highest mortality in severe ARDS (28.61%), followed by moderate ARDS (22.75%) and mild ARDS (22.17%) (P = .001, chi-square test). Similar associations were observed with 60-d mortality (Fig. 1B). Higher mortality acceleration was observed in the severely hypoxemic group within 28 d (Fig. 2). The early phase of accelerated mortality leveled off between 28 and 60 d. Then the hospital mortality rate plateaued after 60 d.

Mortality rate by cause of lung injury (A), and PaO2/FIO2 (B). Chi-squared test was used to calculate P values. Bars show mortality rate ± SD from subgroups defined by each variable. Chi-squared test was used to test the association between the mortalities (alive or dead) and cause of lung injury (sepsis, pneumonia, aspiration, trauma, and other) for A and association between mortalities and PaO2/FIO2 (mild, moderate, and severe) for B.

Cumulative incidence of in-hospital mortality by PaO2/FIO2 category.
Univariate analysis of other secondary outcomes also revealed that ventilator-free days and ICU-free days were most frequent in the case of aspiration and lowest with sepsis (Figs. 3A and 4A) and did not follow a specific pattern in relation to PaO2/FIO2 (Figs. 3B and 4B).

Percentage of subjects with 0, 1–7, 8–14, 15–21, and 22–28 categorized ventilator-free days during the first 28 d after enrollment by cause of lung injury (A), and PaO2/FIO2 ratio (B); chi-squared test was used to test the association between the categorized ventilator-free days and cause of lung injury (sepsis, pneumonia, aspiration, trauma, and other) for A and association between categorized ventilator-free days and PaO2/FIO2 (mild, moderate, and severe) for B.

Percentage of subjects with 0, 1–7, 8–14, 15–21, and 22–28 categorized ICU-free days during the first 28 d after enrollment by cause of lung injury (A) and PaO2/FIO2 (B); chi-squared test was used to test the association between the categorized ICU-free days and cause of lung injury (sepsis, pneumonia, aspiration, trauma, and other) for A and association between categorized ICU-free days and PaO2/FIO2 (mild, moderate, and severe) for B.
On multivariable analysis of outcomes to assess the role of etiology and severity, the following variables were included as covariates: age, sex, race, APACHE III, modified acute lung injury score, vasopressor use, diabetes mellitus, cancer status, body mass index, pre-ICU location, ICU location, and study. With sepsis as the reference variable, trauma had significantly lower 28- and 60-d mortality (odds ratio [OR] = 0.47, 95% CI 0.26–0.83, P = .01 and OR = 0.5, 95% CI 0.3–0.85, P = .01, respectively) (Table 3). As for the severity of ARDS, with mild serving as reference, there were no significant differences in 28-d mortality; however, subjects with severe ARDS had significantly lower 60-d mortality (OR = 0.71, 95% CI 0.53–0.98, P = .034).
Results of Multivariable Regression Models
Also, trauma was associated with the lowest ICU-free days (OR = 0.9, 95% CI 0.83–0.99, P = .02). Aspiration had higher ICU- and ventilator-free days (OR = 1.09, 95% CI 1.02–1.17, P = .01 and OR = 1.09, 95% CI 1.02–1.16 P = .01, respectively) (Table 3). There were no significant differences between the severity of ARDS in relation to ventilator- and ICU-free days (Table 3).
Discussion
The current analysis of the ARDS Network trials was conducted to determine the effect of etiology and severity of ARDS on short-term patient outcomes. It shows that trauma had the lowest 28- and 60-d mortality; it was also associated with the lowest ICU-free days. Aspiration was associated with higher ventilator- and ICU-free days. There were no significant differences between other etiologies of ARDS. Using PaO2/FIO2 as a surrogate for severity of ARDS, there were no differences in 28-d mortality or ventilator- or ICU-free days. Subjects with severe ARDS had lower 60-d mortality.
The impact of etiology of ARDS on outcome has been previously studied with variable and sometimes contradictory results.5,6 The current study shows that there is no difference in mortality between the different etiologies of ARDS except for trauma, which was associated with better prognosis. This finding is consistent with other studies.5 A meta-analysis of 34 studies was performed to determine the difference in outcome (mortality) between subjects with pulmonary and extrapulmonary causes of ARDS. There was no difference in mortality between the 2 groups (OR of mortality in pulmonary ARDS group compared with the extrapulmonary ARDS group was 1.11 (95% CI 0.88–1.39).6 In the case ARDS in the setting of trauma, earlier studies suggested that it has worse prognosis; however, other reports show better outcomes.16,17 The current study of a large and robust database confirms better mortality outcomes for trauma patients but lower ICU-free days.
The better outcome in subjects with ARDS and trauma compared with other groups may be related to multiple factors, including younger age, no co-morbid illnesses, improved ICU care, and the possibility that earlier studies included subjects who had trauma and other complications, such as sepsis, which increased their risk of dying. Also, ARDS in patients with trauma may be in part related to fluid resuscitation and massive transfusions, which are usually associated with fewer inflammatory changes than sepsis or aspiration.18 Furthermore, there is evidence that the severity of lung endothelial and alveolar epithelial injury in ARDS from major trauma appears to be less than that of other clinical disorders associated with acute lung injury.19,20
The implications of potential differences in outcome in relation to the etiology of ARDS are that different diseases may respond differently to therapeutic interventions. However, this theory was not demonstrated in previous studies, including the ARDS Network trials (Table 1). In a study that specifically reviewed the efficacy of low tidal volume in different etiologies of ARDS, there was no difference in outcome.21
Another important finding of this analysis is that the primary outcome of ARDS is not affected by PaO2/FIO2 at the time of enrollment. Also, there were no differences in ventilator- and ICU-free days but lower 60-d mortality in subjects with severe ARDS (PaO2/FIO2 < 100). Whereas some studies have suggested that initial PaO2/FIO2 determined outcome and was lower in non-survivors,22 others have shown that initial PaO2/FIO2 did not independently predict outcome.7,23 The current study provides further evidence, based on a more vigorous database and strict definition of ARDS, that the severity of ARDS, as measured by initial PaO2/FIO2, does not predict outcome, and patients should receive the same level of care and lung-protective measures regardless of how mild or severe the initial assessment of ARDS. PaO2/FIO2 is useful in early identification of patients with ARDS, in fulfilling diagnostic criteria to enroll in clinical trials, and to initiate the appropriate therapies for ARDS; however, it should not be used as a predictor of outcome. A more important predictor of outcome may be the direction of PaO2/FIO2 during the course of management of ARDS, as suggested by one study.24
The explanation of why there are no differences in outcome in relation to initial severity of ARDS could possibly be due to delay in diagnosis and/or management of ARDS in patients with milder disease, leading to worse outcome. Another explanation is that patients with severe ARDS (lower PaO2/FIO2 at randomization) are more likely to receive protective lung strategies or other interventions that have been shown to improve outcome of ARDS, such as muscle relaxation or proning.
The study has several strengths, including the multi-center prospective database, the robust diagnosis of ARDS, strict definition of severity of ARDS at the time of randomization based on the Berlin criteria, heterogeneous patient population including surgical and trauma, and the therapeutic interventions in these trials. There are few limitations that warrant mention. These include the retrospective analysis of the prospective database and the fact that details about the different etiologies, including microbiology, antibiotic treatment, and type of trauma, are lacking. Also, this study does not provide long-term outcomes of the subjects. Further studies are needed to address these limitations.
Conclusions
This study provides further insight about predictors of outcome in subjects with ARDS. Despite the importance of PaO2/FIO2 in making the diagnosis of ARDS and stratifying its severity at the time of diagnosis, this study shows that PaO2/FIO2 does not predict outcome of these subjects. Among the etiologies of ARDS; trauma was associated with best survival compared with other causes.
Footnotes
- Correspondence: Ayman O Soubani MD, Division of Pulmonary, Critical Care, and Sleep Medicine, Wayne State University School of Medicine, Harper University Hospital, 3990 John R-3 Hudson, Detroit, MI 48201. E-mail: asoubani{at}med.wayne.edu.
The authors have disclosed no conflicts of interest.
- Copyright © 2017 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}