

Abstract
INTRODUCTION: There is a paucity of studies comparing the physiological effects of nasal CPAP or non-synchronized noninvasive ventilation (ns-NIV) during the postextubation phase in preterm infants. Heart rate variability (HRV) can identify system instability before clinical or laboratory signs of deterioration. Thus, we sought to investigate any differences in HRV between those modes.
METHODS: 15 preterm infants with birthweight ≤1,250 g and undergoing their first extubation attempt were studied immediately after disconnection from mechanical ventilation. Electrocardiogram (ECG) recordings were obtained while on nasal CPAP and ns-NIV in a random order (30–60 min on each). Time and frequency domain analyses were used to calculate HRV from 5-min segments of ECG.
RESULTS: 12 of 15 infants were analyzed (3 were excluded for low ECG quality): 7 successes and 5 failures. HRV parameters were higher during ns-NIV when compared to nasal CPAP, but differences were not statistically different. However, absolute and relative differences in HRV values (all time domain parameters) were significantly higher in infants who failed extubation during ns-NIV.
CONCLUSIONS: Nasal CPAP or ns-NIV provided immediately postextubation did not affect HRV. Interestingly, in an exploratory analysis, changes in HRV did occur during ns-NIV in the subgroup of infants who failed extubation. Hence, changes in HRV as early as 2 h after extubation should be further explored in larger studies as a potential predictor of postextubation respiratory failure.
- extubation failure
- heart rate variability
- noninvasive ventilation
- preterm infants
- respiratory support
- neonatal intensive care
Introduction
The majority of extremely preterm infants require intubation and mechanical ventilation after birth.1–3 Because mechanical ventilation can lead to complications,4,5 physicians often proceed from early extubation to some type of noninvasive respiratory support,6 most commonly nasal CPAP and noninvasive ventilation (NIV).6,7 In a recent meta-analysis comparing these 2 modes, NIV demonstrated superiority over nasal CPAP in preventing extubation failure.8 However, the pooled studies were very heterogeneous and used different nasal CPAP and NIV modalities, making it difficult to translate these results into clinical practice. From the available evidence, synchronization during NIV appears to confer important clinical and physiological benefits in the immediate postextubation period. In contrast, the mechanisms of action of non-synchronized NIV (ns-NIV) are not yet fully understood.8 To date, the only physiological study comparing nasal CPAP with ns-NIV found no differences in tidal volume, minute ventilation, breathing frequency, gas exchange, or inspiratory effort among clinically stable infants studied 1 wk after extubation.9
Heart rate variability (HRV) refers to the fluctuations of beat-to-beat intervals over time.10 In neonates, HRV measurements identified system instability before clinical or laboratory signs of deterioration, as demonstrated for the prediction of sepsis,11 weaning from mechanical ventilation,12 and outcomes of hypoxic-ischemic encephalopathy.13,14 Therefore, we hypothesized that during the unstable period after extubation, any additional benefit of ns-NIV over nasal CPAP would be reflected by differences in HRV. As a secondary exploratory analysis, differences in HRV and extubation outcomes were evaluated.
QUICK LOOK
Current knowledge
Extubation failure rates are high in extremely preterm infants. To increase the chances of successful extubation, noninvasive respiratory support such as nasal CPAP or ns-NIV are applied immediately after extubation. Heart rate variability is a useful marker of wellbeing and may provide insight on differences between those modes.
What this paper contributes to our knowledge
The study provides new information on the physiological effects of nasal CPAP or ns-NIV in extremely preterm infants immediately after extubation. Heart rate variability was not affected by either mode. An exploratory analysis showed that changes on heart rate variability during ns-NIV occurred only in infants who failed extubation.
Methods
Population
This prospective randomized crossover trial was conducted in 3 neonatal intensive care units (Royal Victoria Hospital, Montreal Children's Hospital and Jewish General Hospital, Montreal, Canada). Subjects with birthweight ≤ 1,250 g, receiving mechanical ventilation, and undergoing their first extubation attempt were eligible. Infants with congenital anomalies or receiving narcotics, sedatives, or inotropes at the time of extubation were excluded. The research ethics board of each institution approved the study, and informed consent was obtained from parents or legal guardians. This study received financial support from the Royal Victoria Foundation.
Peri-extubation Management
Clinical decisions concerning intubation, adjustments, and weaning of mechanical ventilation, timing of extubation, type of postextubation respiratory support provided outside of the study period, and the need for re-intubation were made exclusively by the treating physician. The current practice of the units was to keep oxygen saturation (SpO2) alarms between 85–94% (target: 88–92%).
Study Design and Data Acquisition
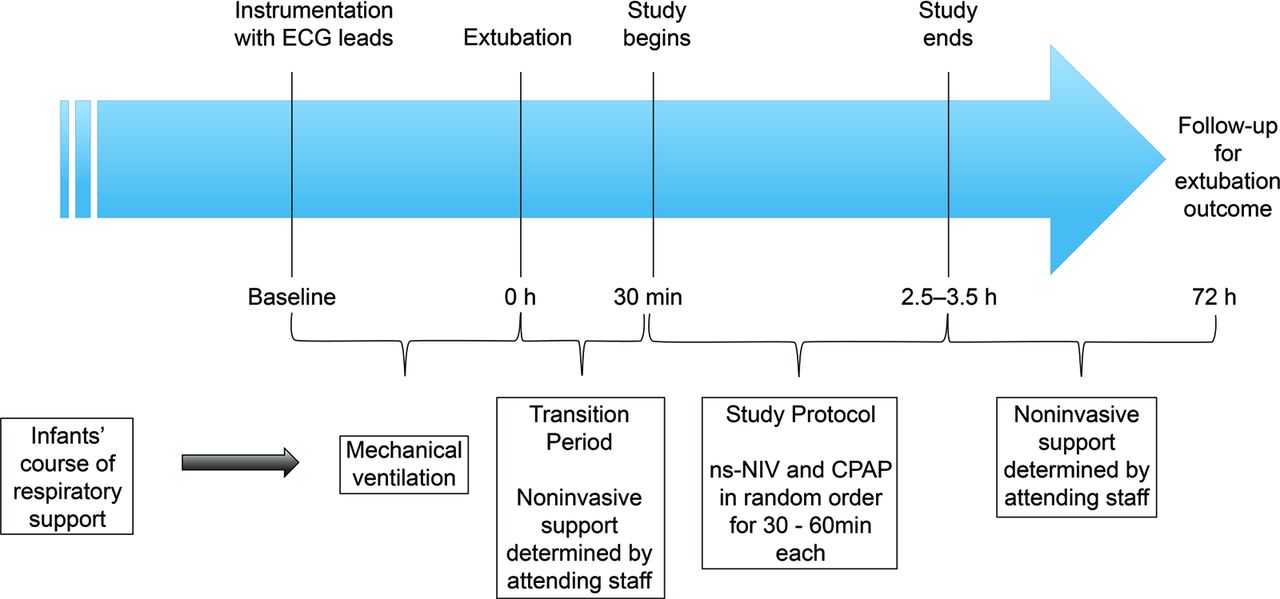
Before extubation, 3 electrocardiogram (ECG) leads were placed on the infants' limbs, at least 1 cm apart from the existing leads to prevent interference. After extubation, a period of 30 min was allowed for rest and stabilization free of any unnecessary manipulations prior to initiation of recordings. During this transition period, infants received the type of noninvasive respiratory support determined by the treating team, either nasal CPAP or ns-NIV. Throughout the study, infants were kept in a supine position, and all efforts were made to minimize leaks by using the appropriate size of binasal prongs (Hudson RCI, Wayne, Pennsylvania) and applying the Cannulaide (Salter Labs, Lake Forest, Illinois) and a chinstrap. Nasal CPAP or ns-NIV was provided in a random order, and oxygen supplementation was adjusted to maintain SpO2 within the target range. Nasal CPAP or PEEP levels were set at 5 or 6 cm H2O (depending on the pre-extubation PEEP level), and inflation pressures during ns-NIV were set 10 cm H2O above the PEEP. ECG was recorded for a period of 30–60 min for each mode using a bioamplifier (FE132, ADInstruments, Colorado Springs, Colorado) connected to the PowerLab acquisition system (ADInstruments), and signals were stored in a research computer for analysis. Recordings on each mode included an initial 10-min washout period. A timeline for the study design is provided in Figure 1.
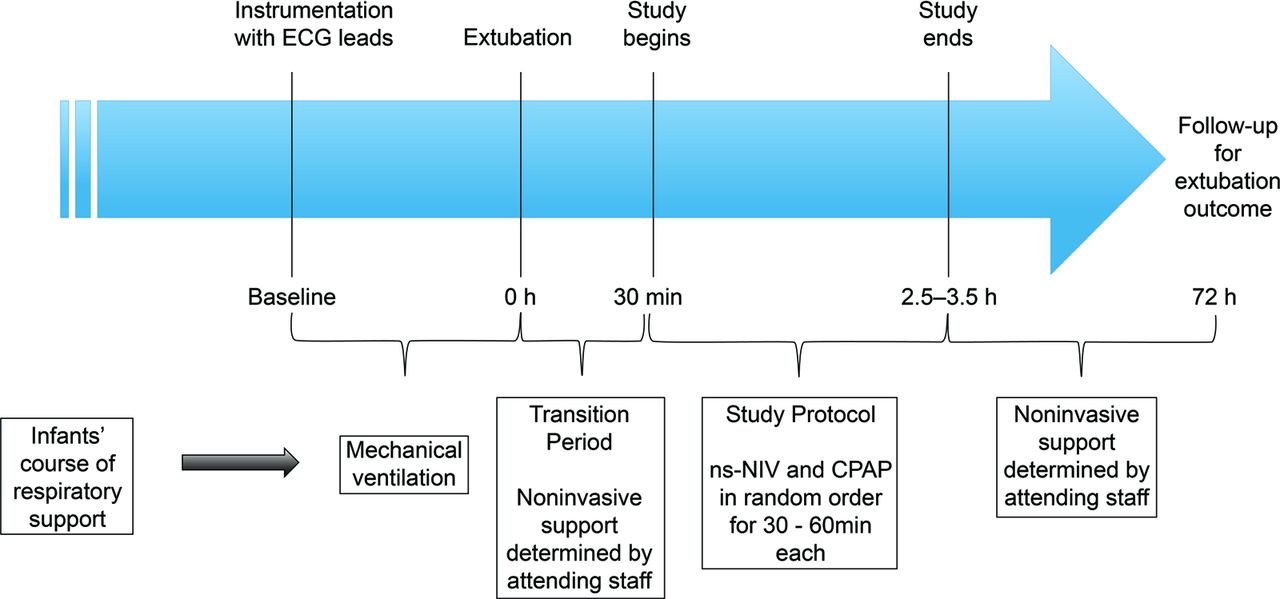
Study timeline. Baseline = 1 h before extubation (mechanically ventilated with echocardiogram leads). 30 min postextubation = study recordings begin with mode of noninvasive support in random order. 72 h postextubation = determine outcome (success or failure). ECG electrocardiogram; NIV = noninvasive ventilation; ns-NIV = non-synchronized NIV.
Heart Rate Variability
HRV analysis was performed offline using the HRV module of the LabChart software (version 1.4.2, ADInstruments). The following definitions were used for the normal-to-normal beat (NN) intervals: normal = 300–600 ms (100–200 beats/min), ectopics = 200–300 ms (200–300 beats/min) and 600–1000 (60–100 beats/min), and artifacts = <200 ms (>300 beats/min) and >1,000 ms (<60 beats/min). Each selected ECG segment required manual adjustments of the voltage thresholds to maximize beat detection. The first 10 min of ECG recording on nasal CPAP or ns-NIV was considered a transitional washout period and was not included in the analysis. The first acceptable 5-min segment with ≤80% normal NN intervals, starting from the end of each mode (or the last segment) was selected. A band-pass filter of 5–80 Hz was applied to each segment prior to analysis to reduce noise. The following time domain parameters were calculated: standard deviation of the NN intervals (SDNN), that is, the variation of intervals measured between consecutive sinus beats, standard deviation of the successive differences between NN intervals (SD delta NN), root mean square of successive differences of NN intervals (RMSSD), and the percentage of adjacent NN intervals that differ by > 50 ms (pNN50). For the frequency domain, the following parameters were obtained: TP: total power (<0.4 Hz), VLF: very low frequency (<0.04 Hz), LF: low frequency (0.04–0.15 Hz), HF: high frequency (>0.15 to <0.4 Hz), and LF/HF: ratio of the low-frequency to high-frequency power.10
Clinical Data
Baseline subject demographics (birthweight, gestational age, sex, Apgar scores along with weight, day of life, and post-conceptional age at extubation), pre-extubation blood gases (pH, PCO2, bicarbonate, and base excess), ventilation settings (mode, peak inspiratory pressure [PIP], PEEP, mean airway pressure (P̄aw), breathing frequency, FIO2, and SpO2), noninvasive respiratory support used during the transition period (mode, PIP, PEEP, and inflation rates), use of caffeine and postnatal steroids at the time of extubation, and extubation outcomes (success or failure) were prospectively collected. Extubation failure was defined as the need for re-intubation within 72 h.6,15 The primary reason for re-intubation (apneas and bradycardias, increased work of breathing, respiratory acidosis) was also recorded.
The primary objective of the study was to investigate for differences in HRV parameters between nasal CPAP and ns-NIV. As a secondary objective, HRV parameters were related to extubation outcomes, with the rationale that successfully extubated infants may have a different underlying physiology compared to infants who fail extubation. As such, the following comparisons were made:
1) For each of the success and failure groups, HRV parameters were compared between nasal CPAP and ns-NIV.
2) For each of the nasal CPAP and ns-NIV groups, HRV parameters were compared between success and failure.
3) The absolute and relative changes in HRV values from one mode to the other (ΔHRV and percentage ΔHRV, respectively) were compared between the success and failure groups. ΔHRV was calculated as the HRV values while on ns-NIV minus nasal CPAP, and percentage ΔHRV was calculated as ΔHRV divided by the nasal CPAP values multiplied by 100.
Sample Size and Statistical Analysis
Given the lack of data on HRV in preterm infants during the immediate postextubation period, a calculation of sample size was not possible. Therefore, a convenience sample size of 12 infants was chosen. On the basis of our previous experience, due to the low quality of ECG signals detected during the offline analysis, a loss between 10–20% of the subjects was expected.12 Thus, we planned to enroll 15 subjects. Continuous and categorical clinical variables were compared using the non-parametric two-sided Wilcoxon rank-sum test or Fisher exact test, respectively (Matlab, MathWorks Inc., Massachusetts). Paired Wilcoxon signed-rank tests were used for all comparisons between nasal CPAP and ns-NIV, while Wilcoxon rank-sum tests were used for all comparisons between success and failure groups. Statistical significance was set at P < .05.
Results
A total of 15 subjects were studied; 3 subjects were excluded due to low-quality ECG (2 were successfully extubated and 1 failed extubation). Of the 12 subjects included, 7 were successfully extubation and 5 failed extubation. Subject demographics, respiratory support settings pre- and postextubation, blood gas results, and postextubation management are described in Tables 1 and 2. Infants who failed extubation were extubated from significantly higher P̄aw (8 vs 6 cm H2O, P = .043). After the study protocol, 1 infant in the success group was switched from ns-NIV to nasal CPAP, while 2 infants in the failure group that were originally receiving nasal CPAP were switched over to ns-NIV (Table 2).
Subject Characteristics and Pre-extubation Management
Postextubation Management
Primary Outcome
All HRV parameters, for both time and frequency domain, were higher during ns-NIV compared to nasal CPAP, but the differences were not statistically significant (Table 3).
Comparison of Heart Rate Variability Parameters Between Nasal CPAP and ns-NIV
Exploratory Analysis
There were no differences on all absolute HRV values between nasal CPAP and ns-NIV for both groups (ie, extubation success and failure). Analysis comparing infants who were successfully extubated or failed extubation showed that, during ns-NIV, a higher SDNN was observed in failure subjects (23.9 ms [20.3–25.1]) versus 14.7 ms [11.8–16.4], respectively, P < .05). Finally, ΔHRV and % ΔHRV values were significantly higher in the failure group for all time domain parameters (Fig. 2). The ΔHRV values were also significantly higher in the failure group for the TP and VLF components of the frequency domain (see the supplementary materials at http://www.rcjournal.com).

Changes in heart rate variability and extubation outcomes. Changes in heart rate variability values were significantly higher in the failure group than the success group for all time domain parameters. A = Absolute changes in heart rate variability. B = Percentage change in heart rate variability. SDNN = standard deviation of NN intervals; SD delta NN = standard deviation of the successive differences between NN intervals; RMSSD = root mean square of successive differences of NN intervals; pNN50 = percentage of adjacent NN intervals that differ by > 50 ms.
Discussion
This prospective crossover observational study provides new information on the physiological effects of ns-NIV in extremely preterm infants undergoing their first extubation attempt. HRV values were higher on ns-NIV compared to nasal CPAP, but differences were not statistically significant. Interestingly, in the exploratory analysis, higher absolute and relative changes in HRV values were observed in infants who failed extubation. Results of this study are unique given the challenges of studying extremely preterm infants during the period immediately after extubation. Furthermore, results of the secondary analysis raise the possibility that HRV measurements may be useful for early identification of infants at high risk of postextubation failure.
Nasal CPAP Versus Non-Synchronized NIV
NIV use has increased as a result of evidence from randomized control trials and a recent meta-analysis8 suggesting improved extubation outcomes compared to nasal CPAP. It is interestingly that most beneficial effects were reported in studies that applied synchronized NIV.8 Indeed, in preterm infants evaluated immediately postextubation, synchronization during NIV was demonstrated to improve tidal volume, minute ventilation, gas exchange, and thoracoabdominal synchrony while reducing breathing frequency and inspiratory effort.16,17 Such beneficial effects have not been reported with ns-NIV,9 and the largest trial evaluating this mode did not show any differences in important clinical outcomes.18
HRV has been shown to be an accurate biomarker of wellbeing, able to detect changes in response to both physiological and non-physiological events.19 In adults, natural R-R interval oscillations occur due to small changes in intrathoracic pressure during normal respiration, and the addition of positive airway pressure has been shown to further modulate HRV.20 Thus, one could hypothesize that, in preterm infants, the application of higher mean airway pressures with ns-NIV would also alter intrathoracic pressure and modulate HRV.21–23 However, transmission of positive pressure to the lungs may not always be reliable, and HRV behavior may vary according to patient stability. In a study evaluating stable preterm infants, ns-NIV was associated with highly variable PIP levels around the set value,24 depending on the timing of inflation in relation to each spontaneous inspiration, presence of leaks, or an apneic event.25 Furthermore, in a newborn lamb model, increased activity of the thyroarytenoid muscle (glottal constriction) was noted during the inspiratory phase of a breath delivered during ns-NIV but not during nasal CPAP. Higher PIP levels were associated with increased thyroarytenoid activity and occasionally caused complete glottal closure, thereby impeding pressure transmission and lung ventilation.26 Finally, another study in stable preterm infants revealed no significant differences in cardiac function and cerebral hemodynamics between nasal CPAP and ns-NIV.27
Our study is the first to investigate the effects of ns-NIV and nasal CPAP on HRV during the immediate postextubation phase. Although an increased level of support resulting from ns-NIV would have theoretically influenced HRV parameters, no statistically significant changes were observed. It is plausible that this was related to the absence of adequate subject–ventilator interaction during ns-NIV.
HRV and Extubation Outcome
Failure of noninvasive respiratory support applied after extubation is highly prevalent in extremely preterm infants.7 Despite clinical and laboratory similarities, some infants are successfully extubated while others fail extubation. No good predictor of extubation outcome is currently available.28 HRV is a highly sensitive tool capable of detecting various stressors and distinguishing between different disease states.19 As such, changes in HRV can reflect intentionally generated responses to internal and external stimuli rather than simple random fluctuations. As an example, application of positive distending pressure resulted in significant HRV changes in subjects with COPD but caused no changes in healthy controls.23 A similar phenomenon was observed in our exploratory analysis, whereby changes between nasal CPAP and ns-NIV did not affect HRV in successfully extubated infants, but such changes caused significantly higher absolute (ΔHRV) and relative changes (% ΔHRV) for almost all HRV parameters in the failure group. We speculate that such changes could indicate a beneficial modulating effect of ns-NIV on the autonomic nervous system of more unstable infants. Another possible explanation is that infants who failed extubation were 2 weeks more immature than successfully extubated subjects. However, evidence from longitudinal studies suggests a very slow maturation process of the autonomic nervous system around 24 to 28 weeks post-conceptional age,29,30 therefore such maturational difference cannot explain the significantly increased ΔHRV parameters observed in the failure group. Alternatively, the differences observed could be related to a discomfort associated with the use of higher P̄aw or the absence of synchronization in the more unstable infants. Nevertheless, while the increased benefit of one mode over the other remains unclear, significant changes in HRV measurements were observed and can be explored in future studies as a potential predictor of respiratory failure, as early as 2 h after extubation. With the introduction of new technologies able to continuously measure HRV at the bedside, prompt identification of infants at high risk of failure could lead to implementation of interventions with the potential to change this undesirable outcome.
This study has several strengths. We used a crossover methodology in random order, which prevents any one mode from influencing the other and the subject acts as his or her own control. ECG and clinical data were prospectively collected and analyzed by a group of researchers familiar with the methodology applied. Given the small numbers for comparison, the analysis of differences between success and failure was solely exploratory and hypothesis-generating. Frequency domain ranges were set according to the guidelines of the Task Force of The European Society of Cardiology and The North American Society of Pacing and Electrophysiology,10 as they are the only standardized ranges that currently exist. Although the ranges are for adults, to our knowledge respiratory sinus arrhythmia has not been demonstrated in infants with gestational age < 30 wks.31 In addition, ECG recordings were made for relatively short durations (30–60 min). It is unclear whether the HRV results would have changed with longer exposure times.
Conclusion
Nasal CPAP or ns-NIV, the two most commonly used modes of noninvasive respiratory support provided to extremely preterm infants immediately after extubation, do not affect HRV. Interestingly, in an exploratory analysis, changes in HRV did occur during ns-NIV in the subgroup of infants who failed extubation. Hence, changes in HRV as early as 2 h after extubation should be further explored in larger studies as a potential predictor of postextubation respiratory failure.
Footnotes
- Correspondence: Guilherme Sant'Anna MD PhD, Associate Professor of Pediatrics, Neonatal Division, McGill University Health Center, 1001 Boulevard Decarie, Room B05.2711, Montreal, Quebec, Canada, H4A3J1. E-mail: guilherme.santanna{at}mcgill.ca.
Ms Latremouille presented a version of this paper at the American Thoracic Society International Conference, held May 13–18, 2016, in San Francisco, California.
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}