

Abstract
INTRODUCTION: Exercise intolerance is the most predominant symptom in patients with COPD. Nevertheless, it is unclear whether walking economy and gait variability are altered in these patients. Thus, our main objective was to compare the cost of transport and gait variability as a function of speed, including the self-selected walking speed, in subjects with COPD relative to healthy subjects.
METHODS: 22 subjects, 11 with COPD (FEV1 = 45 ± 17% of predicted) and 11 age- and sex-matched healthy subjects undertook an evaluation that involved walking on a treadmill at 6 speeds (at 3.2 km/h, at a self-selected walking speed, and at 2 speeds below and 2 speeds above the self-selected walking speed) and measuring the cost of transport (the oxygen consumption normalized by mass and distance), gait variability, perceived dyspnea, and leg fatigue.
RESULTS: In subjects with COPD, the cost of transport decreased with increasing walking speed, contrary to healthy subjects, who presented a minimum at the self-selected walking speed. No difference was found in cost of transport between the experimental groups at the same absolute velocity (P = .62). In subjects with COPD, dyspnea sensation rose above the self-selected walking speed, doubling at the maximal walking velocity (P = .03), and gait variability was higher at low speeds.
CONCLUSION: Subjects with COPD choose their walking speed so as to keep the dyspnea sensation tolerable and to keep gait variability and cost of transport at an acceptable level. These outcomes suggest that interventions acting on dyspnea and gait pattern may increase patients' self-selected walking speed and improve their quality of life
Introduction
Exercise intolerance and activity-related dyspnea are the most common symptoms of patients with COPD,1 resulting in a decrease of daily living activities and a poorer quality of life.1–3 Patients with COPD present a reduction in daily walking intensity2,3 and self-selected walking speed4 compared to control individuals.
The exact nature of exercise limitation in patients with COPD is controversial and probably multifactorial.5–7 Many parameters, including impairment of respiratory mechanics,5 reduced oxidative capacity of skeletal muscles,6 and increased energy demands of respiratory muscles combined with a decrease in oxygen supply,7 may contribute to the reduced maximal work attainable by these patients, depending on the type of exercise and the characteristics of the patient.5–7 In particular, the factors involved in the reduction of the self-selected walking speed chosen by patients with COPD have been poorly investigated.
Healthy patients spontaneously choose a self-selected walking speed corresponding, in terms of walking economy, to the optimal speed, that is, the speed at which the cost of transport (ie, the amount of energy necessary to walk a given distance) is minimal.8,9
It is unknown whether patients with COPD choose the self-selected walking speed according to this criterion. In patients with chronic diseases, pathological factors not necessarily related to walking economy may become preponderant in the choice of the self-selected walking speed.10,11
A candidate factor, which may play a primary role in the choice of the self-selected walking speed by subjects with COPD, is dyspnea sensation. Dyspnea sensation rises with increasing exercise intensity due to the high respiratory drive in the setting of an abnormally high mechanical load. Indeed, in the presence of expiratory-flow limitation and an increased respiratory rate, dynamic hyperinflation develops, leading to augmented inspiratory elastic work along with deleterious hemodynamic consequences.12 On the other hand, the physiological relation between self-selected walking speed and cost of transport can be disrupted by gait and balance deficits,13,14 which are the focus of current research due to their connection with a higher risk of falls.15–18
We hypothesized that, rather than choosing a speed that minimizes the cost of transport, patients with COPD walk at a velocity which represents an adjustment between an unpleasant dyspnea sensation and an excessive cost of transport and gait variability, which may result in a loss of dynamic stability.19
Hence, the main purposes of this study were to measure the relationship between the cost of transport and speed in subjects with COPD and compare them to healthy subjects, to verify whether the self-selected walking speed of subjects with COPD during walking corresponds to the speed at which the cost of transport is minimal, and to assess the role of gait variability and dyspnea sensation in the determination of the cost of transport and the choice of the self-selected walking speed by subjects with COPD.
QUICK LOOK
Current knowledge
Exercise intolerance and ventilatory efficiency impairments have been identified in symptomatic patients with COPD, mainly using a cycle ergometer. It is not known if these factors determine a true physiologic limit to walking ability and metabolic cost of walking (cost of transport). The presence of a high ventilatory equivalent for CO2, suggesting reduced ventilatory efficiency, has consistently been reported in several exercise studies in COPD, but the underlying causes and repercussions for walking economy, gait variability, and self-selected walking speed are still unclear.
What this paper contributes to our knowledge
The cost of transport as a function of speed was similar between subjects with COPD and healthy subjects. Thus, the lower walking velocity that subjects with COPD spontaneously choose cannot be explained by alterations of the energetics of locomotion. Rather, the sharp increase of dyspnea sensation experienced by subjects with COPD at walking velocities greater than the self-selected walking speed indicates that subjects with COPD choose to walk at the maximal speed compatible with a tolerable dyspnea sensation, at the price of an increased cost of transport and gait variability.
Methods
Subjects
Eleven subjects with COPD were recruited from the ambulatory clinic for chronic respiratory disease of the local hospital and were age- and sex-matched with 11 healthy subjects. Inclusion criteria were FEV1/FVC < 0.70 and FEV1 < 80% of the predicted value, former smokers with a smoking history of >20 pack-years, and stable clinical conditions. Exclusion criteria were respiratory tract infections or exacerbations in the last 2 months, concomitant cardiovascular or respiratory diseases, or neuromuscular, orthopedic, or cognitive diseases that could compromise the ability to walk.
Study Design
This cross-sectional study received ethics approval from the local hospital (140149) and followed STROBE recommendations. All of the participants signed an informed consent form. The participants underwent 2 evaluation days at the exercise laboratory of pathophysiology and pulmonary function at the Hospital de Clínicas de Porto Alegre. On the first day, each participant underwent a spirometric evaluation at rest and an incremental cardiopulmonary exercise test on a treadmill. The cost of transport and gait variability were measured on the second day, with a minimum interval of 48 h between the 2 visits. The submaximal and maximal tests were carried out as proposed by Figueiredo et al.10 A detailed description of data collection and analysis can be found in the online supplement (see the supplementary materials at http://www.rcjournal.com).
Pulmonary Function Test
Spirometry was performed in accordance with international standards20 using a Jaeger Oxycon (CareFusion, Heidelberg, Germany). Results are reported as absolute and percent of predicted values.21
Cardiopulmonary Exercise Test (CPET)
After a 10-min familiarization with the treadmill (INBRAMED 10200, Porto Alegre, Rio Grande do Sul, Brazil), the speed was set to a predetermined ground self-selected walking speed, and the subject was asked to walk while adjusting the speed until the pace was the most comfortable (self-selected walking speed). Along with the self-selected walking speed, 4 other speeds were defined as ± 20% and ± 40% the self-selected walking speed, as previously described.10 In addition to these 5 speeds, all subjects walked at a common speed of 3.2 km/h so that all participants could be compared at the same absolute walking speed (ie, isovelocity speed).
After standing still on the treadmill for 5 min, the participants were instructed to walk for 5 min at each of the 6 speeds, in random order. The relevant parameters (ventilation [V̇E], carbon dioxide production [V̇CO2], and oxygen consumption, [V̇O2]) were collected breath by breath using an ergoespirometric device (Jaeger Oxycon, Würzburg, Germany). Heart rate and pulse oxygen saturation (SpO2) were continuously monitored. Reported values are the average of the last 2 min using a 20-s filter. The dyspnea sensation intensity and leg fatigue were rated using the Borg scale scoring between 0 (no dyspnea or leg fatigue at all) and 10 (most severe sensation of dyspnea or leg fatigue that the patient could imagine). The subject was allowed to rest between the different runs, until V̇O2, heart rate, leg fatigue, and dyspnea sensation returned to resting values. The rest maximal time between bouts was not more than 5 min.
The difference between V̇O2 during walking and at rest was normalized by the walking speed and the weight of the subject. This value, times 20.1 J/mL O210, is the cost of transport.
For the measurement of gait variability, a video camera (120 Hz; Casio, Exilim FH25, Tokyo, Japan) was used to film the subjects' left side while walking on the treadmill at each speed.22 Gait variability (ie, stride-to-stride fluctuations) was indexed by the coefficient of variation of the stride frequency, calculated every 10 strides.
Statistical Analyses
We conducted a transversal physiological study with the primary outcome measure consisting of cost of transport and secondary outcomes of gait variability and self-selected walking speed using SPSS software v.20.0 (Chicago, Illinois). A P < .05 level of significance was used for all analyses.
This study was powered to detect a 30% difference in cost of transport between healthy subjects and subjects with COPD with a statistical power of 80%, assuming that the standard deviation of the cost of transport at self-selected walking speed in both experimental groups is similar to that previously reported in healthy and chronic heart failure subjects.10
Data normality and sphericity were tested with Shapiro-Wilk and Mauchly's test, respectively. Parametric data were analyzed with a generalized estimating equation followed by Bonferroni corrections for comparisons between groups and speeds. Anthropometric, pulmonary function, and cardiopulmonary parameters were compared using independent sample t tests. The same test was used to compare parameters at isovelocity. Nonparametric data such as dyspnea sensation and leg fatigue were analyzed with the Friedman test and with Wilcoxon or Mann-Whitney tests. Pearson's product moment correlations were used for parametric data, and Spearman's rank correlations for nonparametric data. A stepwise linear regression was performed to predict the cost of transport through self-selected walking speed and coefficient of variation in the COPD group.
Results
No differences were detected regarding age, body mass index, or lower limb length between healthy subjects and subjects with COPD (Table 1). When compared to the control group, subjects with COPD presented lower peak V̇O2 and ventilation. In subjects with COPD, the latter parameter was almost equal to maximum voluntary ventilation, in accordance with a ventilatory limitation to exercise (Table 1).
Subject Characteristics and Cardiopulmonary Exercise Test
Effects of Speed on the Cost of transport, Ventilatory Efficiency, Dyspnea, and Leg Fatigue
The self-selected walking speed chosen by subjects with COPD was significantly lower than that selected by healthy subjects (2.6 ± 0.5 vs 3.6 ± 0.7 km/h, P < .001). At the self-selected walking speed, the cost of transport was not different in subjects with COPD relative to controls (3.3 ± 0.6 vs 2.9 ± 0.7 J/kg/m, P = .18). In healthy subjects, the relationship between the speed and the cost of transport was parabolic, and the self-selected walking speed corresponded to the speed at which the cost of transport was minimal (Fig. 1A). In contrast, the cost of transport decreased when subjects with COPD walked at speeds higher than the self-selected speed (Fig. 1A). When the cost of transport in healthy subjects and subjects with COPD was plotted against absolute speed, it became evident that there was no difference in terms of the cost of transport between the 2 experimental groups (Fig. 1B), as confirmed by the absence of a difference in the cost of transport at isovelocity (P = .62).
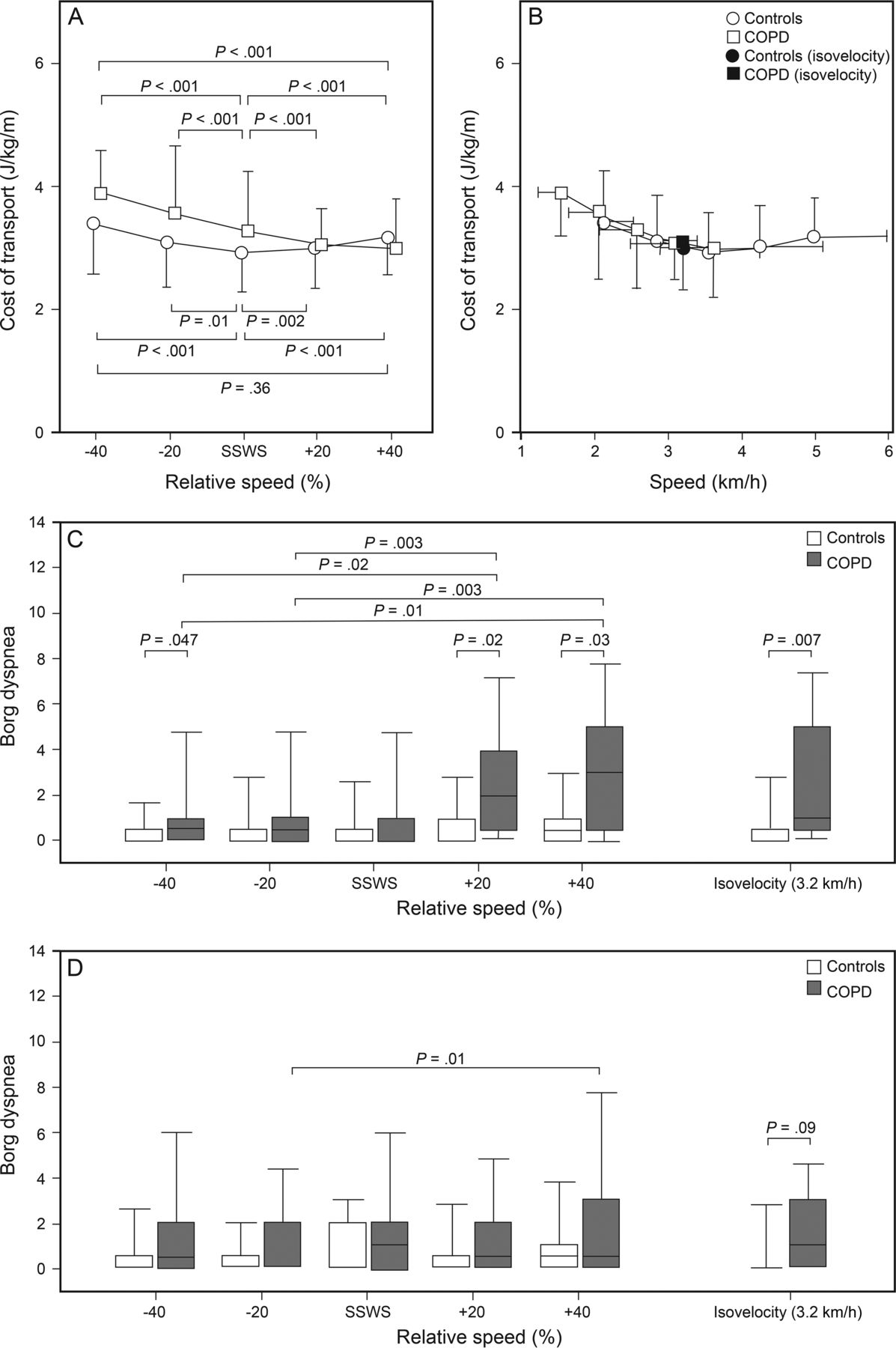
The cost of transport as a function of relative (A) or absolute (B) walking speed in healthy subjects and individuals with COPD. Values are mean ± SD. Dyspnea sensation and leg fatigue are shown as a function of relative velocity in C and D, respectively. Relevant comparisons between different relative speed levels are indicated above the plots for subjects with COPD and below for healthy subjects. SSWS = self-selected walking speed.
When the speed was equal or less than the self-selected speed, dyspnea sensation was independent of velocity and not different between healthy subjects and individuals with COPD (Fig. 1C). In contrast to healthy subjects, however, dyspnea sensation increased in subjects with COPD when walking speed exceeded the self-selected speed, doubling at + 40% of the self-selected walking speed (P = .03). At isovelocity, dyspnea sensation was markedly greater in subjects with COPD than in healthy subjects (P = .007) (Fig. 1C).
Leg fatigue was not different between the 2 experimental groups at each relative velocity (Fig. 1D). The perceived leg fatigue at isovelocity tended to be greater in subjects with COPD than in healthy subjects, but this difference was not statistically significant (Fig. 1D, P = .09).
At rest, ventilatory equivalent for CO2 was greater for subjects with COPD relative to healthy subjects (49 ± 3 vs 42 ± 2, P = .041). During walking, the ventilatory equivalent for CO2 remained greater in subjects with COPD than in healthy subjects at each absolute or relative speed (P = .004) and declined similarly in both experimental groups; the interaction between the speed level (within-subjects factor) and the experimental group (between-subjects factor) was not significant (P = .48), and the linear component of the within-subjects contrasts was significant (P < .001). The ventilatory equivalent for CO2 was greater for subjects with COPD relative to healthy subjects also at isovelocity (38 ± 5 vs 33 ± 3, P = .030) (Fig. 2).

The ventilatory equivalent as a function of relative walking or absolute speed. Values are mean ± SD. P values are control group versus subjects with COPD in the same relative speed. SSWS = self-selected walking speed.
Gait Variability
In 2 subjects (1 healthy and 1 with COPD), coefficient of variation data were missing due to a camera malfunction. For this parameter, normality was not present at −40% of the self-selected walking speed (P < .001), and sphericity was violated (P < .001). Consequently, nonparametric statistics has been applied.
Gait variability, as indexed by the coefficient of variation, tended to decrease with increasing relative walking speed in both groups (Fig. 3A). In the control group, significant differences were found between the −40% and +20% (P = .007) and between −20% and +20% of self-selected walking speed (P = .007), while subjects with COPD presented significant differences between −40% and +40% (P = .01) and between −40% and the self-selected walking speed (P = .047). Significant differences between healthy subjects and subjects with COPD were detected only at −40% (P = .035) and +20% (P = .035) of the self-selected walking speed. When the coefficient of variation was represented as a function of the absolute velocity (Fig. 3B), the differences between the groups disappeared, as indicated by the coefficient of variation measured at isovelocity (P = .28) in subjects with COPD and healthy subjects, 1.82% (0.24) and 1.45% (0.76), respectively (Fig. 3A).

The coefficient of variation as a function of relative (A) or absolute (B) walking speed in healthy subjects and subjects with COPD. SSWS = self-selected walking speed.
Overall, the relationship between the coefficient of variation and the cost of transport at the self-selected walking speed was significant (P = .041) with a positive slope (0.47 ± 0.21 J/m/kg/%), indicating that gait variability may be a determinant of the cost of transport (Fig. 4A). The cost of transport was negatively correlated with the self-selected walking speed (Fig. 4B). When a multiple linear regression was performed, using the cost of transport at self-selected walking speed as the dependent variable and the coefficient of variation and self-selected walking speed as independent variables, only in subjects with COPD were both the coefficient of variation and self-selected walking speed significant predictors of the cost of transport (P = .046 and .030, respectively), according to the following equation: cost of transport = −0.795 speed + 0.553 coefficient of variation + 4.360 (R2 = 0.62).

Correlation between the cost of transport with the coefficient of variation (A) and self-selected walking speed (SSWS) (B).
Discussion
The main finding of this study is that the relationship between the cost of transport and velocity in stable subjects with COPD was similar to that of healthy subjects. Contrary to healthy subjects, however, subjects with COPD did not choose spontaneously to walk at the speed corresponding to the minimal cost of transport. Instead, they chose a lower walking speed to avoid the abrupt increase of dyspnea sensation that develops at speeds higher than the self-selected walking speed. The concomitant rise in the cost of transport and gait variability at low speeds probably limits the reduction of the self-selected walking speed chosen by patients with COPD.
The pendular mechanism describes walking as an inverted pendulum because of the energy exchanges that occur at the body's center of mass.23 In this model, the transfer of kinetic and potential energy is greatest at intermediate speeds,24 reducing the total mechanical work that must be performed by muscles at those speeds. Actually, the observed minimum cost of transport at the optimal walking speed is consistent with both the contractile physiology of skeletal muscle and the mechanics of terrestrial locomotion.24 Notably, our study suggests that both experimental groups presented the same absolute optimal speed (Fig. 1B).
To our knowledge, this is the first study to measure the cost of transport in subjects with COPD. At the same absolute speed, individuals with COPD presented a cost of transport not significantly different from that of healthy subjects (Fig. 1B). This finding is in a sense surprising, because the cost of transport derives from the difference between the energy expenditure measured during walking at a given speed and at rest, and thus it includes the cost of the increase in ventilation. In healthy individuals, the metabolic cost of ventilation is low, especially in the ventilation range measured during walking. To the contrary, in patients with COPD, the cost of ventilation can become an important part of the total metabolic cost.25 The average difference in V̇O2 between healthy individuals and patients with COPD in the speed range between 2.9 and 3.7 km/h has been used to estimate an upper limit for the cost of breathing of patients with COPD. It has been assumed that the cost of breathing in healthy subjects in the ventilation range considered is practically nil,26 and that the cost of transport at a given absolute speed is equal for patients with COPD and healthy subjects. With these assumptions, the V̇O2 difference between healthy individuals and subjects with COPD divided by the ventilation measured in the latter group corresponds to the metabolic cost of ventilation. This estimate corresponds to a cost of breathing in individuals with COPD of 2 mL O2 per liter of ventilation, and is much less than that predicted by Levison and Cherniak.25 Such a discrepancy could be explained if, during walking, lactic acid production was high, but this apparently does not happen.27 Therefore, this old issue remains unsolved.25,28
The self-selected walking speed chosen by subjects with COPD did not correspond to the speed at which the cost of transport is minimal. A similar finding has been reported in patients with chronic heart failure,10 reflecting how one or more pathological processes may interfere with the optimization of locomotion.
Among the potential exercise-limiting factors, 3 have been investigated by this study: dyspnea sensation, leg fatigue, and gait variability. In our subjects with COPD, dyspnea sensation did not change with walking velocity below self-selected walking speed but increased abruptly at higher speeds (Fig. 1C). These results strongly suggest that patients with COPD choose the highest speed at which dyspnea sensation is tolerable, despite a worse walking economy. In this study, we did not measure inspiratory capacity, but it is tempting to speculate that dynamic hyperinflation, with its associated burden of increased respiratory work, decreased respiratory muscle efficiency, and deleterious cardiovascular effects, may be a primary factor in the genesis of breathlessness.5,29,30
In patients with COPD, leg fatigue has been advocated as a limiting factor of maximal exercise due primarily to alterations of the skeletal muscles6 or secondarily to reduced perfusion because of the functional stealing of part of the cardiac output by the respiratory muscles under stress.7 In our subjects, leg fatigue was not significantly different between healthy subjects and subjects with COPD at isovelocity (Fig. 1D), and it did not substantially change in the velocity range investigated. Thus it is unlikely that leg fatigue was a discriminating factor in the choice of the self-selected walking speed in our subjects with COPD.
Gait variability has received considerable attention in recent years, as it is a marker of fall risk in elderly patients31 and other populations such as hemiparetic,32 Parkinson's,33 and Alzheimer's34 patients. Contrary to heart rate variability, gait variability is usually considered a sign of pathology.19
Patients with COPD present an increased risk of falls,13 and lower limb muscle weakness,6,35 gait and balance deficits13,36 and abnormalities of their walking mechanics37,38 have been reported, especially in patients with a high frequency of exacerbations and with more severe COPD (group D, GOLD grade).39 Therefore, it was reasonable to hypothesize greater gait variability in subjects with COPD than in healthy subjects.
Contrary to our expectations, no difference in gait variability was detected at isovelocity or at self-selected walking speed (Fig. 3A). Regardless of the group, gait variability demonstrated a tendency to diminish as the walking speed increased.32,40 As the lowest walking speed for the COPD subjects was outside the velocity range of healthy subjects, we cannot say from our data whether the high gait variability the subjects experienced at −40% of the self-selected walking speed is abnormal or not, but comparison with a previously published work shows that the latter possibility is probably the case.41
A recent study39 based on a large number of participants (898 healthy subjects and 196 subjects with COPD) investigated the gait pattern in subjects with COPD, but comparisons with our results are difficult because the experimental conditions were very different from ours, as the participants walked on a 5.79-m electronic walkway, and not continuously on a treadmill. Moreover, the factors identified by the authors using principal component analysis on several gait parameters are not in a univocal relationship with gait variability, being correlated to multiple factors. However, they report that in subjects with COPD gait alterations are more related to a lower walking speed and step time rather than to an increase in gait variability. These results are in accordance with the low interaction between walking performance and gait variability described18 in subjects with COPD during a 6-min walk test. This last study demonstrated a decreased autocorrelation coefficient of the displacement of the trunk only in the mediolateral direction, which would indicate higher gait variability. However, as the decrease was found only in this parameter, it is not enough to state an overall gait instability in patients with COPD. Thus, these findings seem to be in line with our results.
In subjects with COPD, the cost of transport at self-selected walking speed increased with increasing gait variability (Fig. 4A) and decreased with increasing speed (Fig. 4B). This result can be easily explained taking into account the dependence of the cost of transport on the walking speed if the descending limb of the curve describing this relation (Fig. 1B) and the dependence of gait variability on the walking speed (Fig. 3) are considered. Multiple linear regressions including the cost of transport at self-selected walking speed as the dependent variable and the coefficient of variation and the self-selected walking speed as independent variables showed that both the walking speed and the coefficient of variation were predictors of the cost of transport. This result suggests that gait variability may be a determinant of the cost of transport in patients with COPD.
This work has some limitations that should be taken into account. The study was powered to reveal a moderate increase in the cost of transport at self-selected walking speeds, and not for a full characterization of the differences in walking mechanics between subgroups of subjects with COPD with different disease severity. Moreover, the possible role of gait variability in the determination of the cost of transport should be verified in a larger number of patients. Patients were excluded from this study if affected by comorbidities,42 even though at least some of these diseases may affect the walking behavior of patients with COPD. In the present work, gait variability has been indexed by the fluctuations of the stride frequency. We recognize that this is an arbitrary choice, as many other parameters (eg, step length or stride width) could have been considered, and these parameters are not necessarily related to the same control system.36 On the other hand, at least in young subjects, the coefficients of variation of step interval and length, and of stride interval and length, appear to change similarly with changes in walking speed.39 No attempt has been made to quantify the long-range correlations, which form the structure of the stride-to-stride fluctuations.43
In summary, subjects with COPD did not choose to walk at a speed at which the cost of transport is minimal, and their walking economy did not seem to be different from that of healthy subjects at the same absolute speed or at the self-selected walking speed. In addition, the self-selected walking speed chosen by subjects with COPD seems to be a perfect strategy to walk at the fastest possible velocity while mitigating dyspnea and avoiding excessive gait variability and cost of transport.
Acknowledgments
The authors thank Julia Schnandorf Japur and Jonas Santos for their hard work and assistance during pilot testing and data collection. We are grateful to Adalberto Sperb Rubin PhD at Federal University of Health Science of Porto Alegre, Daniel Umpierre PhD at Federal University of Pelotas, Marli Knorst PhD at Federal University of Rio Grande do Sul, and Locomotion Group of UFRGS for discussions and comments. Dr Peyré-Tartaruga is an established investigator of the Brazilian Research Council–CNPq, Brasília, Brazil.
Footnotes
- Correspondence: Leonardo A Peyré-Tartaruga PhD, Exercise Research Laboratory, Universidade Federal do Rio Grande do Sul, Rua Felizardo, 750, 90690-200 Porto Alegre, Brazil. E-mail: leonardo.tartaruga{at}ufrgs.br.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}