

Abstract
Noninvasively applied positive airway pressure therapy (PAP) is available in 3 basic modes: continuous positive airway pressure (CPAP), bi-level positive airway pressure (BPAP), and adaptive servo-ventilation. These are in widespread use in home and hospital settings to treat a variety of disorders of ventilation or gas exchange, including obstructive sleep apnea, sleep-related hypoventilation, periodic breathing, acute and chronic hypercapnic respiratory failure, and acute respiratory failure. They are increasingly being used perioperatively to prevent or treat upper airway obstruction, hypoventilation, and periodic breathing, and they have been found to improve postoperative outcomes in the case of obstructive sleep apnea. An impediment to their use in this setting is a lack of familiarity with their application by hospital clinical staff. This review describes the modes of PAP therapy available, their indications, how therapy is initiated, how efficacy is assessed, common problems encountered with its use, and how these problems can be addressed.
- PAP therapy
- respiratory compromise
- obstructive sleep apnea
- opioids
- sleep-disordered breathing
- adaptive servo-ventilation
- CPAP
- BPAP
- hospital
- adult
Introduction
In recent years there has been a growing recognition that patients prone to disordered breathing during sleep are predisposed to abnormal breathing disturbances when sedated or anesthetized. Obstructive sleep apnea (OSA) is known to increase the incidence of cardiopulmonary complications in the perioperative period.1–7 Obesity hypoventilation is also associated with increased risk of perioperative complications, and it appears likely that sleep hypoventilation from other causes (eg, respiratory neuromuscular or advanced lung diseases) is similarly predisposed.8,9 These breathing disorders can be effectively treated with positive airway pressure (PAP) therapies delivered noninvasively via face or nasal mask. PAP therapies are increasingly used perioperatively to prevent or treat upper airway obstruction, hypoventilation, and periodic breathing,10 and they have been found to improve postoperative outcomes in the case of OSA.11 An impediment to the use of these therapies in the hospital setting is a lack of familiarity with their indications and application on the part of hospital clinical staff, which may lead to delays in seeking respiratory therapist expertise to implement therapy. This review describes the modes of PAP therapy available, their indications, how therapy is initiated, how its efficacy is assessed, common problems encountered with its use, and how these problems can be addressed. While the emphasis is on the perioperative care of patients with known, suspected, or emergent sleep-disordered breathing, many of the points made are generalizable to other perioperative noninvasive respiratory support applications, including prevention of postoperative pulmonary complications from other causes and treatment of postoperative respiratory failure in other settings.
Modes of PAP Therapy
There are 3 basic modes of PAP therapy available: CPAP, bi-level PAP (BPAP), and adaptive servo-ventilation. Both CPAP and BPAP are available as manually adjustable or auto-adjusting devices, while aspects of adaptive servo-ventilation are inherently automatic in their operation. A more recent addition to the PAP therapy group includes volume-assured pressure support (VAPS), another auto-adjusting therapy used in specific situations of hypoventilation. It should be noted that there are many synonyms in use for these therapies, although the terminology used here predominates.
CPAP
CPAP is the simplest of the PAP modes, providing continuous pressure to the upper airway and lower respiratory tract to provide a distending force, or pneumatic splint. It is commonly used to treat and prevent upper airway obstruction during sleep (ie, OSA) or when induced by sedation.12 It can also be used to distend the central airways (as with laryngomalacia or tracheomalacia),13 recruit alveoli (as with atelectasis or pulmonary collapse/consolidation),14 counter intrinsic PEEP in the case of COPD-associated dynamic hyperinflation,15 or redistribute lung water and decrease cardiac preload and afterload (as with pulmonary edema and cardiac failure).16
CPAP devices deliver air at pressures generally adjusted within a range between 5 and 20 cm H2O, depending on an individual's requirement. In OSA, the required level of pressure may be determined by titration during an attended overnight in-lab polysomnogram/CPAP titration study. In the hospital setting, when a patient has not previously been titrated on CPAP therapy, an empiric setting of 8 cm H2O is a reasonable starting point for a patient of normal weight.17 The pressure can be titrated from there, in steps of 0.5–2 cm H2O depending on tolerance and adequacy of control to control upper airway obstruction. While adequate control may be achieved at pressures < 10 cm H2O, higher pressures are commonly required, particularly in obese patients.18 Occasionally pressures in excess of 15 cm H2O are needed, which can be difficult to tolerate, particularly if the patient is naïve to therapy. Higher mask pressures are also associated with increased mask leak. In such cases, it can be advantageous to use CPAP in an auto-titrating mode (sometimes known as APAP) rather than at a fixed pressure. APAP is a CPAP application designed to treat upper airway obstruction and is now commonly used to initiate PAP therapy in place of supervised CPAP titration during polysomnography. APAP auto-titrates the pressure level within an adjustable range (predetermined by the prescriber, often in the 6–16 cm H2O range) to abolish flow limitation. The APAP device detects flow limitation by analysis of the respired flow signal, assessing for flattening of the inspiratory flow profile.19,20 Its advantage over fixed pressure is that the pressure varies according to need, so that it is low during wakefulness and, during sleep, may only reach higher pressures when the patient is supine or in rapid eye movement sleep, which are both circumstances conducive to worsening upper airway obstruction. Where high airway pressures are consistently required to control obstruction, BPAP (see below) may be helpful in providing some inspiratory assistance to relieve work of breathing.
Although termed continuous, the pressure delivered by CPAP may vary across the respiratory cycle. Some manufacturers provide an option that momentarily reduces pressure by a small degree during early expiration (expiratory relief). This serves as a comfort setting to alleviate the sensation of expiratory effort that some patients develop, particularly early in their exposure to CPAP.21
CPAP and APAP are primarily used in the out-patient setting for the management of OSA, and occasionally CPAP is used for some patients with central sleep apnea. CPAP can be used in the in-patient setting for ongoing management of sleep-disordered breathing, acute hypoxic respiratory failure from a variety of causes (eg, atelectasis, interstitial lung disease, pulmonary consolidation), recruiting of collapsible large airways (eg, tracheomalacia), non-hypercapnic COPD exacerbations where intrinsic PEEP may be an issue, and pulmonary edema.12–16 CPAP is not recommended as the primary therapy for sleep-related hypoventilation in the absence of co-existing OSA.
BPAP
There are many alternative terms to describe BPAP. These include generic terms such as, bi-level ventilatory assistance, and noninvasive pressure-support ventilation, as well as proprietary terms such as bi-level positive airway pressure (BiPAP, Philips Respironics) and variable positive airway pressure (VPAP, ResMed). For the purposes of this review, the term BPAP encapsulates all of these terms.
BPAP delivers different, independently adjustable pressures during expiration (ie, expiratory PAP [EPAP]) and during inspiration (ie, inspiratory PAP [IPAP]). This terminology is conventionally used in relationship to BPAP but is equivalent, respectively, to PEEP and inspiratory pressure, which are terms used in relationship to invasive mechanical ventilation. It should be noted, however, that with invasive mechanical ventilation, the term pressure support refers to the difference between the total inspiratory pressure and the PEEP and does not reflect the total inspiratory pressure. EPAP provides the same functionality as CPAP, delivering a background level of pressure that prevents upper airway obstruction or atelectasis. The IPAP level is set above the EPAP level, and the difference between these pressures provides pressure support to assist inspiratory effort. This augments ventilatory efforts, preventing or treating hypoventilation, and relieves the work of breathing in proportion to the delivered level of pressure support.22
In the acute phase, when patients are new to BPAP, a reasonable start point is an IPAP of 14 cm H2O and an EPAP of 6 cm H2O, although some would start lower. These pressures are typically adequate to provide at least partial control of hypoventilation and upper airway obstruction while generally being tolerable to a patient who is naïve to therapy. Further adjustments are made, generally in steps of 0.5–2 cm H2O, according to the patient's tolerance and response to therapy. It should be noted that ineffective therapy is poorly tolerated, so where incomplete control is achieved, an increase in pressures may lead to improved tolerance rather than the converse. While persisting upper airway obstruction is primarily addressed by increasing EPAP, IPAP has to be adjusted as well if the level of pressure support is to be preserved. Given that levels of IPAP much in excess of 20 cm H2O are often poorly tolerated because of pressure-associated mask leaks (with the need to apply the mask more tightly), mouth leaks (where a nasal mask is used) and aerophagia, the level of EPAP titration needs to be tempered because of incursions on pressure support levels as the tolerable limits of IPAP are reached. Fortunately, increasing IPAP has a stabilizing effect on the upper airway independent of EPAP, such that obstruction can be controlled at lower levels of EPAP than with conventional CPAP therapy alone.23
BPAP modes of delivery are spontaneous (S), spontaneous-timed (ST), and timed (T). In S mode, pressure support is automatically triggered by inspiratory effort. In ST mode, if no inspiratory effort is made within a predetermined interval, which can be adjusted (usually by setting a minimum back-up breathing frequency), the device will deliver pressure support in a mandatory fashion. In T mode (not often used), pressure support is delivered at set intervals (ie, at a predetermined breathing frequency).
Both EPAP and pressure support can be prescribed at a set level (determined by bedside titration or, in the out-patient setting, during an attended overnight in-lab polysomnogram/BPAP titration study) or automatically titrated to an effect level, within an adjustable range of pressures. In auto-titration, the device auto-titrates EPAP to prevent upper airway obstruction and adjusts pressure support to maintain an adequate level of ventilation within bounds set by the prescriber.
In the out-patient setting, BPAP is mostly used for management of OSA (often for patients who do not tolerate CPAP or those who require high pressures to control upper airway obstruction) and sleep-related hypoventilation (which may co-exist with OSA). For in-patients, BPAP can be used for the same conditions as well as for acute hypercapnic respiratory failure and acute hypoxemic respiratory failure.24,25 It has been found to be effective for patients with OSA and comorbid COPD, obesity hypoventilation syndrome, and respiratory neuromuscular disorders.8,26,27
VAPS is a relatively new mode of BPAP ventilation that is being used increasingly in the out-patient setting to manage patients with sleep-related hypoventilation syndromes with or without OSA.28 Like standard BPAP, it delivers an EPAP for upper airway obstruction or to recruit alveoli, but unlike BPAP it delivers a level of pressure support within a predetermined range to maintain a set minute or alveolar ventilation to more precisely control ventilation during sleep. Currently, VAPS ventilation is primarily being used for patients neuromuscular disease-associated with sleep-related hypoventilation, although some authors have suggested it should be considered in patients with other hypoventilation syndromes.29,30 Similarly to BPAP, VAPS is often referred to by its various trade names, which include AVAPS (average volume-assured pressure support; Philips Respironics) and IVAPS (intelligent volume-assured pressure support; ResMed).
Adaptive Servo-Ventilation
This mode of PAP therapy is used to treat periodic breathing either in isolation or in combination with OSA (so-called complex sleep apnea). As with BPAP, adaptive servo-ventilation delivers EPAP and pressure support. While the level of EPAP is adjustable in a manner similar to BPAP, adaptive servo-ventilation differs from BPAP in that the level of pressure support varies from breath to breath, decreasing as spontaneous effort increases and increasing as it decreases in an anticyclical or “antidromic,” fashion to stabilize breathing. This modulates the variable ventilation otherwise observed during periodic breathing. Untreated, periodic breathing can be quite disruptive to sleep, with arousals tending to occur during the excessive ventilatory response, or hyperpneic, phase.31
While adaptive servo-ventilation automatically varies the level of pressure support in the presence of variable inspiratory effort, the pressure support range within which this adjustment may occur is determined by the prescriber. EPAP can be manually adjusted, but many recent devices offer auto-titration of EPAP to levels adequate to prevent upper airway obstruction.
Adaptive servo-ventilation is used for the management of periodic breathing associated with preserved ejection fraction heart failure, opioid use, or treatment-emergent central sleep apnea.32–36 There has been recent controversy regarding its use in patients with low ejection fraction (<45%) heart failure. Initiation of this therapy for periodic breathing in this group of patients is not currently recommended.36 Adaptive servo-ventilation is not indicated for the management of uncomplicated OSA or for sleep-related hypoventilation.
Initiating PAP Therapy in the Hospital Setting
A series of decisions are required when initiating PAP therapy (Table 1). The first step is to determine whether PAP is required and, if so, which modality should be used and is it appropriate to deliver it noninvasively. Having judged these matters and decided to proceed with a noninvasively delivered PAP therapy mode, the next steps are to decide on the type of mask to be used, the device settings, whether to use the therapy continuously or semi-continuously, and whether adjunctive therapy such as oxygen is to be used.
Decision Tree for Positive Airway Pressure Therapies
Is PAP Therapy Required?
The main indications for PAP therapy in the perioperative period are uncontrolled upper airway obstruction or hypoventilation during recovery from anesthesia or during ongoing exposure to opioid or sedative drugs, particularly during sleep.37,38
Patients with known sleep-disordered breathing, obesity hypoventilation, and neuromuscular disorders are at increased risk of developing adverse events as a result of these problems. PAP therapy must be considered for such patients during sleep or when sedated. PAP therapy may also be necessary in patients not previously known to have sleep-disordered breathing but who are observed to obstruct or hypoventilate under these circumstances. Given common predisposing factors such as obesity, obstructive lung disease, or neuromuscular disease, these breathing problems can coexist.
Which PAP Therapy Modality?
When not associated with sleep-related hypoventilation or hypercapnic respiratory failure, upper airway obstruction can be treated with CPAP or APAP. When sleep-related hypoventilation or hypercapnic respiratory failure are present, with or without upper airway obstruction, BPAP is indicated (with its EPAP level adjusted to deal with upper airway obstruction where applicable).24
The role for adaptive servo-ventilation is very limited perioperatively, but it may be considered when periodic breathing is a prominent feature or in patients who are already on this therapy at home.35 Likewise, the role for the de novo institution of VAPS therapy in the perioperative period is generally not advocated as the use of BPAP is sufficient for the majority of hypoventilation cases. However, in patients on VAPS therapy at home, this can be continued in the perioperative setting.
Judging When to Start Therapy
A number of patients will present preoperatively with a known diagnosis of sleep-disordered breathing (eg, OSA, central sleep apnea, or hypoventilation) and may already be on some form of PAP therapy at home. Every effort should be made to ensure these patients receive their appropriate PAP therapy postoperatively. This may be accomplished by having patients bring their own device to the hospital (usually requiring a device check to ensure safety and correct settings) or having the hospital provide the patients with the correct PAP therapy. Local policies often dictate this process. However, it should be kept in mind that all forms of sleep-disordered breathing can worsen perioperatively and that monitoring to assess for adjustments of home therapy may be required.
For patients naïve to PAP therapy, judging when to start therapy in the perioperative context will involve various combinations of clinical observation, monitoring of ventilation and gas exchange, and measurement of arterial blood gases according to the circumstances of the case. Application of these therapies perioperatively must occur in a suitably monitored environment (eg, recovery room, stepdown unit). Among other things, use of PAP does not eliminate the need for adequate monitoring as the initiation of new therapy in this environment is subject to difficulties and may be removed or refused by the patient.39
In the case of upper airway obstruction, the problem may be quite obvious from bedside observation. Where unresponsive to simple measures, such as re-posturing or lessening sedation, and where there is not an immediate need for tracheal intubation, CPAP therapy can be considered. If not detected by bedside observation, the issue may be identified by monitoring of ventilation (eg, expired CO2 or other measures of oronasal air flow) or pulse oximetry. In the case of oximetry, care must be taken to account for the effects of oxygen therapy on obstruction-related desaturations, which may be masked or eliminated.40
In the case of hypoventilation, with or without obstruction, clinical context provides important clues. The existence of predisposing factors such as obesity, neuromuscular disease, or advanced pulmonary disease (particularly obstructive lung disease) should heighten awareness. An elevated HCO3− level on perioperative blood work-up can be a sign of chronic hypoventilation (indicating buffering of overnight CO2 retention) and may warrant closer scrutiny.41 Sedating medications, including opioid analgesics, may also increase the risk of acute hypoventilation.42,43 Inadequate respiratory efforts may be apparent at the bedside. Bedside monitoring may reveal sustained hypoxemia and elevated end-tidal CO2 levels. Where further information is required, an arterial blood gas measurement may reveal CO2 retention with attendant acid/base changes. If such hypoventilation is severe and not likely to immediately respond to other measures (such as reversal of sedation), then a strong case exists for tracheal intubation and invasive ventilation.44 However, if it the hypercapnia is of milder degree and unresponsive to other measures, then noninvasive BPAP may be considered.
Choosing the Interface
Having decided to apply PAP therapy and the modality to be used, the next decision is to choose a suitable interface: an oronasal mask that covers nose and mouth, a nasal mask that covers the nose, or a nasal pillow mask that delivers therapy directly to the external nares (Fig. 1). There are other less commonly used interfaces, such as masks that cover the entire face (the total face mask, Fig. 1) or helmets, which can be considered if there are difficulties in applying or tolerating other mask types.
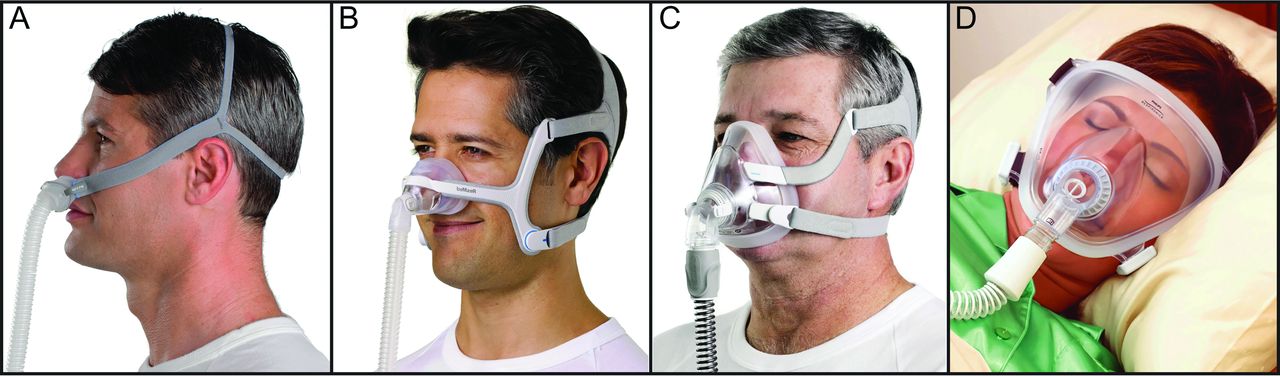
Interfaces. A = nasal pillow mask. B = nasal mask. C = oronasal mask. D = total face mask. Courtesy of Philips Respironics and ResMed.
For patients naïve to PAP therapies, oronasal masks can be a good starting point, particularly in acute situations as they provide more complete control of the airway. Furthermore, they are specifically indicated in the case of nasal obstruction. However, they are more intrusive than nasal masks or nasal pillow masks, which are favored by most patients for long-term therapy (provided they do not have nasal obstruction). Hence, once control of the ventilatory problem has been achieved and the patient has become accustomed to PAP, if there is a need for ongoing treatment, changing to a simpler, less cumbersome nasal mask or nasal pillow mask should be considered, providing they are not precluded by nasal obstruction. The choice between nasal mask or nasal pillow mask is largely according to patient preference.43 Nasal pillow masks are the least intrusive mask style and can be helpful where nasal valve narrowing is present. When nasal masks or nasal pillow masks are used, close attention to oral leaking is warranted because oral escape of air can be problematic in some patients when sedated/asleep, and it can limit the efficacy of therapy. A significantly dry mouth can be a clue to this issue. In such cases, a chin strap may overcome the problem. Where problems persist, changing to an oronasal mask may be required. However, it has been suggested that upper airway obstruction may be more difficult to control with oronasal masks in some patients who, if there is evidence of persisting obstruction despite use of high airway pressures, may benefit from a change to a nasal mask.45
Device Settings and Adequacy of Therapy
In patients already on PAP therapy, it is important to note that pressure settings used successfully at home may be insufficient in the postoperative setting. Pressure requirements may increase because of the depressant effects of opioid or sedative drugs on muscle activation, ventilatory drive and arousal responses, fluid retention, and the effects of upper airway edema in the case of upper airway surgery. Home settings may also be inappropriate in some cases because PAP therapy has been suboptimally titrated. These possibilities need to be kept in mind during implementation of therapy in the hospital setting. The first few postoperative days are likely to be times of particular vulnerability, given the tendency of sleep-disordered breathing to worsen during this period.46
In the case of CPAP applied to overcome upper airway obstruction, airway pressure is adjusted to eliminate the problem; titration end points encompass elimination of snoring and incomplete obstruction, not just major obstructive events. During out-patient use of CPAP therapy, pressure titration may be formally performed during an overnight attended polysomnography or, increasingly commonly, by use of APAP. APAP can be used indefinitely after therapy initiation, or the pressure requirement determined by it can be used to adjust a fixed-pressure CPAP appliance for subsequent ongoing use, which may be a less expensive solution. For patients using CPAP for the first time after surgery, these goals may initially be accomplished with APAP or with bedside manual titration of the pressure setting to eliminate snoring and witnessed obstructions or desaturations.
The CPAP devices themselves often have internal monitoring capabilities (eg, delivered pressure, apnea-hypopnea indices, leak, hours of use); however, depending on the specific device, these parameters may only be available by retrospective download rather than in real time. In addition to these parameters, bedside monitoring may include continuous measures of oronasal air flow (eg, by capnography or pneumotachography) and PaO2 saturation. Minimization of mask and mouth leaks and elimination of obstruction, flow limitation, and desaturation events are important end points. Persistent snoring, witnessed obstruction, or desaturation (≥ 3%) events suggest further adjustment of pressure is required.
Most APAP devices are quite effective in eliminating obstruction and air-flow limitation, although the algorithms for doing so vary between the manufacturers. APAP devices deliver a lower average pressure than manually adjusted devices as the pressure ranges up and down overnight according to the depth of sleep and body posture, only delivering the highest pressure when needed (eg, when in rapid eye movement sleep or supine). They are often better tolerated than manual devices in which high pressures are required to cope with such circumstances overnight. Indeed, excessively high CPAP levels (in general > 15 cm H2O) may be poorly tolerated and are associated with increased mask and mouth leak, tighter strap adjustment, and aerophagia. Sometimes the upper limit of applied pressure has to be adjusted to take this into account, even if it involves some compromise in efficacy. The usual working range of CPAP levels required to control upper airway obstruction is 8–14 cm H2O, although some patients have requirements outside this range.
Where BPAP is used, EPAP is titrated to ensure elimination of obstruction. The required level of EPAP is often less than the CPAP level needed to eliminate obstruction in an individual, which, together with the pressure support it provides, can make BPAP more tolerable and a useful substitute for CPAP when upper airway obstruction is proving difficult to control. However, the predominant indication for the pressure support provided by BPAP is to control hypoventilation/hypercapnic respiratory failure. In general, an initial arbitrary pressure support level is adopted (often of the order of 6 cm H2O above the EPAP setting), and pressure is then adjusted to ensure adequate chest wall displacement, measured tidal volumes (if the information is available from the device or other bedside measure), relief of dyspnea (where applicable), maintenance of PaO2 saturation, and CO2 elimination. While bedside monitoring of end-tidal CO2 can be helpful in the latter regard, it may not always be accurate, and arterial blood gas measurement may provide an important although intermittent assessment of treatment efficacy.43
An important bedside observation when on BPAP is that of patient–ventilator synchrony. Outward chest wall displacement should coincide with application of inspiratory pressure support. A lack of synchrony in this regard indicates either an upper airway obstruction or a large mask or mouth leak, either of which will cause the BPAP device to fail to detect patient inspiratory effort. Adjustment of the delivered pressures to overcome upper airway obstruction or adjusting the mask fit should eliminate this problem.
In addition to pressure settings, another important BPAP device setting option is breathing rate. While this does not apply to S mode, in the ST mode the set rate dictates the length of the expiratory pause before a mandatory breath is imposed in the absence of a patient-triggered inspiration. This back-up breathing rate is typically set at 20% below the spontaneous breathing rate. An additional device setting includes the capacity to set inspiratory breath time through minimum and maximum settings. These settings ensure that triggered breaths are sustained for an effective length of time, but not excessively long. Inspiration usually occupies 40% of the duration of each breath, and this would be a good starting point for most patients. BPAP devices also incorporate a number of comfort settings, with a delayed “rise time” to slow down (and thereby soften) the onset of inspiration, expiratory pressure release/flex control to facilitate expiration, and a ramp setting to delay onset of therapy at the prescribed settings to allow time for settling before therapy starts in earnest. With BPAP devices that titrate pressure support (auto-adjusting BPAP), target tidal volumes and minute ventilation can also be set.
Alarm functions include alerts for apneas, disconnections, low minute ventilation or tidal volume, and power failure. Some devices have a built-in battery in case of power failure, which provides a power supply within the limits of battery life.
Continuous or Semi-Continuous Use?
These therapies will usually require an initial period of continuous use, during which, if the problem is severe, the option of invasive ventilation must be kept in mind. However, as control of the situation is established, use can be changed to intermittent, provided the patient's status off-therapy allows. Even where hypoventilation remains an issue, CO2 accumulation off-therapy is slow, allowing short respites in the first instance, provided PaO2 saturation is controlled. With further improvement it may be that the therapy is only needed during sleep, sometimes supplemented by intermittent periods during the day. Monitoring of ventilation and oximetry, supplemented by intermittent blood gas measurement, helps determine this.47 However, in most cases, patients should be continued on their PAP therapy during all periods of sleep pending further evaluation to determine long-term need for therapy.
Additional Therapies
Other therapies are often used in conjunction with PAP. Oxygen can be added to the delivery system where there is persistent hypoxemia despite adjustment of ventilatory parameters and adequate control of hypercapnia. Some BPAP devices incorporate an O2 blender, using wall or cylinder O2 sources, allowing high inspired O2 concentrations to be delivered. Adjustment of body posture can be helpful by elevating the upper body to facilitate ventilation and adjusting lateral posture to reduce pressures required to control upper airway obstruction. Use of chin straps and heated humidification are common additions to improve the comfort and effectiveness of therapy.
Contraindications for Noninvasive PAP Therapies
Noninvasive PAP therapies should not be used where there is impending or actual respiratory arrest (ie, immediate intubation need); cardiac/hemodynamic instability; respiratory conditions (upper airway or lung) requiring application of high airway pressures; aspiration risk; copious secretions; recent facial, upper airway, or gastrointestinal surgery or trauma; interface (mask) problems; an uncooperative, confused, or agitated patient; or an undrained pneumothorax.24
Troubleshooting Problems Causing Therapy Discomfort
There are a number of sources of discomfort with these relatively intrusive therapies. Effective troubleshooting can substantially relieve these issues, improving adherence to treatment which, together with efficacy, determines the effectiveness of therapy.48
Mask-Related Problems
Mask discomfort demands mask adjustment and, if problems persist, a change to a different type or brand of mask. Claustrophobia can be an issue, and a change to a less intrusive mask (eg, nasal pillows) can help, as can desensitization. Eye irritation is often the result of escape of air into the eyes. When this occurs, the mask should be adjusted or changed to eliminate this. Skin breakdown, particularly across the nasal bridge, can result from excessive mask tightening, which should be avoided. If skin rashes occur, changing to a type or brand made of different materials may help. A protective barrier (eg, of non-plastic material) may also help.49
Pressure-Related Problems
Nasal congestion can occur. This often relates to mucosal drying, particularly if there are large mouth leaks present. Related symptoms include nasal and oral dryness, rhinorrhea, and occasionally epistaxis. If any of these problems occur, ensure adequate (heated) humidification of the delivered air and eliminate leaks. Consider using an oronasal mask if there are persistent mouth leaks despite use of a good-quality chin strap. Nasal topical sprays (ie, steroids, antihistamines) have a role in treating nasal congestion, but providers should avoid long-term decongestant use. If the patient is intolerant of pressure, lower the setting or, in the case of CPAP, consider options including conversion to APAP to avoid high pressures, use of expiratory pressure relief, or conversion to BPAP to provide some inspiratory assistance. Aerophagia can occur with PAP therapies. In general, this is relieved by reducing delivered pressures. Compromise on pressures is sensible if needed, so as to strike an effective balance between therapeutic efficacy and adherence to treatment, although closer monitoring may be required during this time.50
Conclusions
Noninvasive PAP therapies continue to evolve. They have an expanding role within the hospital setting and, arguably, have been underutilized in the perioperative setting. Improvement in the equipment used to deliver these therapies—devices, humidifiers, and interfaces—have increased their efficacy, versatility, and acceptability to patients. More sophisticated therapy modes are available, and masks are less intrusive. Devices now incorporate a range of comfort settings and auto-titrating capabilities. There is better understanding of pathophysiology and the optimal use of therapy. These developments are improving the capacity to tailor therapy to individual needs and circumstances and to facilitate transfers between operating room, ICU, stepdown units, ward, and home. One of the main barriers to the use of these therapies is a lack of familiarity by hospital clinical staff with their application, and it is hoped that this review may help reduce thresholds to their use.
Footnotes
- Correspondence: Carla Jungquist PhD ANP, University at Buffalo, 3435 Main Street, Buffalo, NY 14214. E-mail: carlajun{at}buffalo.edu.
Dr Hillman has disclosed a relationship with ResMed. Drs Jungquist and Auckley have disclosed relationships with Medtronic.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}