

Abstract
BACKGROUND: High-flow nasal cannula (HFNC) enables delivery of humidified gas at high flow while controlling the FIO2. Although its use is growing in patients with acute respiratory failure, little is known about the impact of HFNC on lung volume. Therefore, we aimed to assess lung volume changes in healthy subjects at different flows and positions.
METHODS: This was a prospective physiological study performed in 16 healthy subjects. The changes in lung volumes were assessed by measuring end-expiratory lung impedance by using electrical impedance tomography. All the subjects successively breathed during 5 min in these following conditions: while in a supine position without HFNC (T0) and 3 measurements in a semi-seated position at 45° without HFNC (T1), and with HFNC at a flow of 30 L/min (T2), and 50 L/min (T3).
RESULTS: Compared with the supine position, the values of end-expiratory lung impedance significantly increased with the subjects in a semi-seated position. End-expiratory lung impedance significantly increased after HFNC initiation in subjects in a semi-seated position and further increased by increasing flow at 50 L/min. When taking the end-expiratory lung impedance measurement in subjects in a semi-seated position (T1) as reference, the differences among the medians of global end-expiratory lung impedance were statistically significant (P < .001), which amounted to 1.05 units in T1; 1.12 units in T2; and 1.44 units in T3 (P < .05 for all comparisons, Wilcoxon test). The breathing frequency did not differ between the supine and semi-seated position (T0 and T1) but significantly decreased after initiation of HFNC and further decreased at high flow. T0 and T1 were not different (P = .13); whereas there was a statistically significant difference among T1, T2, and T3 (P < .05, post hoc test with Bonferroni correction).
CONCLUSIONS: In healthy subjects, the semi-seated position and the use of HFNC increased end-expiratory lung impedance globally. These changes were accompanied by a significant decrease in the breathing frequency.
- high-flow nasal cannula
- oxygen inhalation therapy
- high-flow devices
- electrical impedance tomography
- end-expiratory lung impedance
- end-expiratory lung volume
Introduction
Use of high-flow nasal cannula (HFNC) is a therapy that allows the delivery of heated, humidified gas at high flow (up to 60 L/min).1 Its use in ICUs has increased in the past few years due to its proven benefit in certain clinical contexts, such as acute hypoxemic respiratory failure2 and prevention of orotracheal re-intubation.3 Likewise, there is evidence of its efficacy in other pathologies that require admission to ICU, for example, respiratory failure in patients who are immunocompromised.4–6 The mechanism whereby HFNC is effective in the aforementioned situations is still under discussion; however, the presence of positive airway pressure in addition to the high flow used,7,8 followed by an increase in lung volumes, could explain, in part, its effectiveness.9,10
Electrical impedance tomography (EIT) is a noninvasive lung impedance assessment method performed with portable equipment, at the foot end of the patient's bed, is free of radiation, and provides real-time images.11,12 Monitoring through EIT involves the application of a low electrical current and the measurement of the resulting voltages to determine impedance changes related to ventilation, especially those related to regional ventilation. It has been demonstrated that, in patients who are intubated, an adequate correlation exists between end-expiratory lung volume (EELV) and end-expiratory lung impedance.13,14 In recent years, EIT has been used to assess changes in lung volumes as a result of changes in the body position in healthy subjects.9,15,16 It has also been used to study changes in end-expiratory lung impedance related to the use of HFNC in subjects in the prone position.10 However, until now, to our knowledge, only one study assessed the impact on end-expiratory lung impedance of HFNC use at different flows and with the subject in the semi-seated position at a 45° angle, although the laboratory device used for such purposes is difficult to adapt to clinical practice.
Our primary objective was to assess end-expiratory lung impedance global changes induced by HFNC use at different flows in healthy subjects and with the subjects in the semi-seated position. The secondary objectives consisted of analyzing end-expiratory lung impedance behavior in different lung zones and the impact of HFNC use on breathing frequency.
QUICK LOOK
Current knowledge
The use of the high-flow nasal cannula (HFNC) in healthy individuals and in patients with acute hypoxemic respiratory failure when in the semi-seated position has been associated with an increase in end-expiratory lung impedance and a decrease in breathing frequency.
What this paper contributes to our knowledge
The end-expiratory lung impedance increase in healthy subjects was associated with the use of HFNC and with changes in body position. There was a significant increase in end-expiratory lung impedance when the position changed from supine to sitting, but this was not accompanied by changes in breathing frequency in the subjects when breathing room air. However, the use of HFNC with the subjects in a semi-seated position was followed not only by a gain in end-expiratory lung impedance but also by a decrease in breathing frequency.
Methods
We conducted a prospective physiological study between March 13 and April 7, 2017, in the ICU of Anchorena Hospital in Buenos Aires, Argentina. The investigational review board of Anchorena Hospital reviewed and approved the study protocol.
Participants
Healthy subjects >18 y of age and with no smoking history were included. Each participant gave informed consent to be included in the study. Confidentiality of the data was preserved through the creation of a coded registration form for each participant. The name or any other information that would make it possible to identify the subject was kept strictly confidential and was not, nor will be, made public under any circumstances.
Main Variables of Interest
We gathered the participants' demographic and anthropometric data as well as their breathing frequency, changes in end-expiratory lung impedance measured through the EIT, and their parameters during the use of HFNC. For interventions and measurements, an EIT (PulmoVista 500; Dräger, Lübeck, Germany), previously calibrated and self-tested according to the manufacturer's recommendations, was used, together with 16-electrode rubber belts selected in accordance with each participant's thoracic diameter. The belt was placed between the fourth and the sixth intercostal space, on the skin, which was previously wetted with liquid alcohol to improve contact of the electrodes and thereby generate an optimal signal recording. A reference gel electrode was placed on the anterior abdominal wall.
End-expiratory lung impedance measurements are regarded as a relative value, expressed in units, compared with a reference value. The global and regional end-expiratory lung impedance variation (region of interest) in different positions was recorded through the end-expiratory lung impedance. The region of interest function defines 4 sectors (1, 2, 3 and 4) (Fig. 1) within the impedance image of the global end-expiratory lung impedance. Each of these sectors inform us about the corresponding end-expiratory lung impedance variation value. Thus, the image can be divided horizontally or in quadrants. For this study, we obtained a high-quality signal and chose 4 regions of interest as quadrants. For the analysis of different regions, we considered regions of interest 1–2 and regions of interest 3–4.

The region of interest (ROI) function allows the definition of 4 regions (1, 2, 3, and 4 in the top left the figure) within the impedance image of the global end-expiratory lung impedance. For this study, with a high signal quality, 4 ROIs were defined as quadrants. Were considered toghether ROI 1–2 and ROI 3–4 respectively.
An AIRVO 2 (Fisher & Paykel, Auckland, New Zealand), a humidifier chamber with a heated wire circuit for adults (900PT501; Fisher & Paykel) and silicone nasal cannulae for high-flow oxygen therapy (Optiflow OPT844 medium and OPT846 large; Fisher & Paykel) were used as a high-flow oxygen therapy device. During implementation, the flow, temperature, and FIO2 used were recorded.
Four lung impedance measurements were taken. One with each subject in the supine position, at an angle of 180°, with no HFNC (T0). Afterward, 3 measurements with the subject in a semi-seated position, at a 45° angle, were taken; the first with no HFNC (T1, baseline), the second with HFNC at a flow of 30 L/min (T2), and the third with HFNC at a flow of 50 L/min (T3). The implementation of HFNC was carried out with a FIO2 of 0.21 and a temperature of 31°C in all the cases. The subjects remained in each of these positions for 5 min. There was a 5-min pause between one measurement and the next, during which time the volunteer remained in a supine position, at an angle of 180°, and with no HFNC to rule out a sum of effects. During the study period, the subjects were asked to maintain a nasal breathing pattern, at a normal rate and with the mouth closed. The main researcher (GAP) was responsible for both handling the tomograph and implementing the protocol, whereas an assistant (RAP, CMQ, MEA, JHD, RSG, PAD) was in charge of recording the data on a paper form in real time. At the same time, each of the measurements in digital format (screenshots) was filed by means of a data storage device connected to the PulmoVista 500 tomograph's USB port.
Statistical Analysis
Continuous data were expressed as mean ± SD or as median and interquartile range according to their frequency distribution. Categorical data were expressed as absolute values and/or percentages. The Shapiro-Wilk and the Kolmogorov-Smirnov tests of normality were conducted. To compare variables among the subjects, the non-parametric Friedman test was used for repeated measurements. Comparisons were made with the statistical Wilcoxon rank-sum test with the Bonferroni correction. Analysis of variance was conducted for repeated measures for variables with normal distribution, with post hoc contrasts with the Bonferroni correction. P values < .05 were considered significant. SPSS version 20.0 (IBM, Armonk, NY) was used for the statistical analysis.
Results
Sixteen healthy subjects (8 men and 8 women), with a median (interquartile range) age of 33 (32–38) y, height of 172 (166.7–173.5) cm, weight of 73 (61.2–76.1) kg, and body mass index of 23.2 (22.2–25.9) kg/m2 were studied (Table 1). All the subjects followed the instructions about preserving strict nasal breathing with the mouth closed throughout the study period. Global end-expiratory lung impedance was significantly different among all the conditions (P < .001) and increased from 0 to 1.05 (0.72–1.34) units with the subject in the semi-seated position and further increased, to 1.12 (0.8–2.01) units and 1.44 (1.05–2.16) units, during HFNC at a flow of 30 and 50 L/min, respectively (P < .05 for all comparisons, Wilcoxon test) (Fig. 2).
Demographic and Anthropometric Characteristics of the 16 Healthy Subjects Who Participated in the Study

Global deviation of the end-expiratory lung impedance (EELI) in the different positions according to the Friedman test (P < .001). Changes between groups according to Wilcoxon test were as follows: T0 vs T1 (P < .001), T0 vs T2 (P < .001), T0 vs T3 (P < .001), T1 vs T2 (P = .01), T1 vs T3 (P = .001), and T2 vs T3 (P < .001). T0 = supine position without HFNC; T1 = semi-seated position at 45° without HFNC (Baseline); T2 = semi-seated position at 45° with HFNC at a flow of 30 L/m; T3 = semi-seated position at 45° with HFNC at a flow of 50 L/m; HFNC = high-flow nasal cannula. Data presented as median (interquartile range).
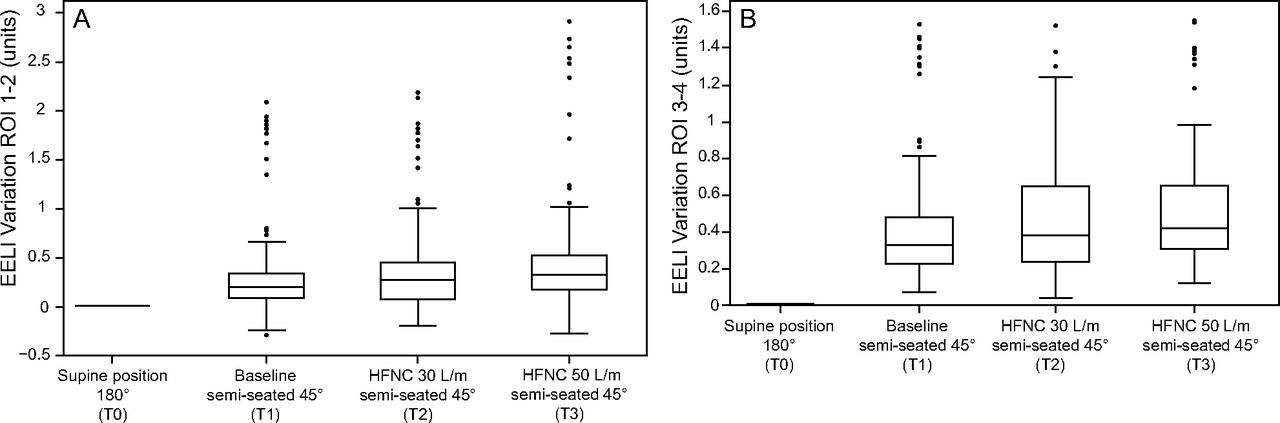
In addition, we found a significant difference when comparing the regions of interest grouped as regions of interest 1–2 versus regions of interest 3–4 (Fig. 3) (P < .001). The median (interquartile range) end-expiratory lung impedance variations were 0.2 (0.11–0.34) units, 0.27 (0.08–0.45) units, and 0.33 (0.18–053) units in regions of interest 1–2; and were 0.33 (0.23–0.47) units, 0.39 (0.24–0.64) units, and 0.42 (0.31–0.65) units in regions of interest 3–4, for T1, T2, and T3, respectively (P < .05 for all comparisons, Wilcoxon test) (Fig. 3). The ratio of end-expiratory lung impedance in regions of interest 1–2 and regions of interest 3–4 should ideally be 1, which indicates a homogenous ventilation. This ratio increased from 0.6 to 0.78 with the subject in the seated position, when adding HFNC at a flow of 50 L/min.

Regional variation of end-expiratory lung impedance (EELI) in different positions according to the Friedman test (P < .001). Changes between groups according to Wilcoxon test in regions of interest (ROI) 1–2 (A): T0 vs T1 (P < .001), T0 vs T2 (P < .001), T0 vs T3 (P < .001), T1 vs T2 (P = .01), T1 vs T3 (P = .001), and T2 vs T3 (P = .001). The change in EELI variation in ROIs 3–4 (B) was as follows: T0 vs T1 (P < .001), T0 vs T2 (P < .001), T0 vs T3 (P < .001), T1 vs T2 (P = .01), T1 vs T3 (P = .001), and T2 vs T3 (P = .001). T0 = supine position without HFNC; T1 = semi-seated position at 45° without HFNC (Baseline); T2 = semi-seated position at 45° with HFNC at a flow of 30 L/m; T3 = semi-seated position at 45° with HFNC at a flow of 50 L/m; HFNC = high-flow nasal cannula. Data presented as median (interquartile range).
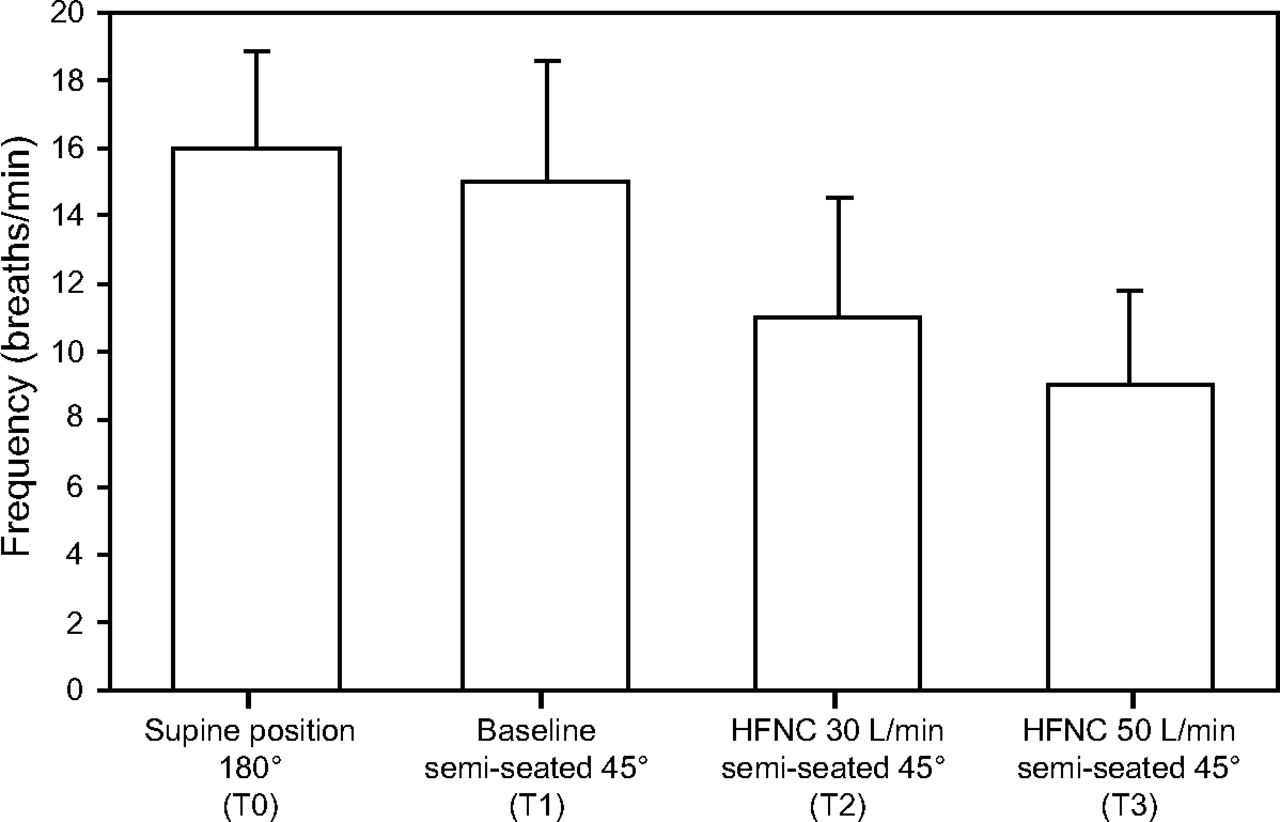
Moreover, a statistically significant difference was found when comparing the breathing frequency among all the measurements (P < .001, analysis of variance). In the post hoc analysis, this difference was attributed to a breathing frequency variation among T1 (15 ± 3.6 breaths/min), T2 (11 ± 3.6 breaths/min), and T3 (9 ± 2.8 breaths/min) (P < .05 for all comparisons, post hoc test with Bonferroni correction) (Fig. 4). On the contrary, T0 and T1 were not different (16 vs 15 breaths/min, respectively) (P = .13).

The average variation of breathing frequency in different positions according to the analysis of variance (P < .001). Differences between groups according to the post hoc test with the Bonferroni correction were as follows: T0 vs T1 (P = .13), T0 vs T2 (P = .02), T0 vs T3 (P = .001), T1 vs T2 (P = .01), T1 vs T3 (P = .01), and T2 vs T3 (P = .02). T0 = supine position without HFNC; T1 = semi-seated position at 45° without HFNC (Baseline); T2 = semi-seated position at 45° with HFNC at a flow of 30 L/m; T3 = semi-seated position at 45° with HFNC at a flow of 50 L/m. Data presented as mean (± SD).
Discussion
The use of the HFNC in healthy subjects was associated with a significant increase in end-expiratory lung impedance, a decrease in breathing frequency, and a more uniform distribution of alveolar ventilation between lung regions. In intubated patients who are mechanically ventilated, a positive correlation has been observed between the end-expiratory lung impedance and the increase in EELV,13,17 which represents an important pulmonary function marker that has been suggested by some resesarchers as an alveolar recruitment tool.18,19 In this study, the use of an increasing HFNC flow in healthy subjects when in a semi-seated position at a 45° angle, correlated with an increase in end-expiratory lung impedance, and, therefore, in EELV.
Corley et al9 demonstrated that the use of HFNC as opposed to a simple O2 mask in subjects with respiratory failure in the postoperative period of cardiovascular surgery was associated with an increase in global end-expiratory lung impedance. The researcher assessed the end-expiratory lung impedance with the subjects in a reverse Trendelenburg position (body supine at a 45° angle) and in a seated position, at a 90° angle, in an undifferentiated way; therefore, the changes in position could have determined changes in end-expiratory lung impedance, independent of those strictly generated by the use of the HFNC. Thus, in this study, it was decided that the subjects would be evaluated in a semi-seated position so as to differentiate the changes in lung volume that result from positional changes and to be able to compare the influence of HFNC. Our population of healthy subjects showed body mass index variability lower than that of the study by Corley et al9; therefore, we could consider that the effects achieved by the HFNC on end-expiratory lung impedance would apply to a more specific population. Finally, in the study by Corley et al,9 the recruited subjects had an average age higher than that of our population (65 vs 34 y); therefore, the age as well as the presence of comorbidities could have generated changes in ELLI independent of those caused by the use of the HFNC. Age is associated with gradual changes in pulmonary function and lung volume,20 which include an increase in lung compliance due to both the decrease in parenchymal elastic recoil and the increase in thoracic rigidity,21 which, consequently, cause changes in lung volumes.20,22
One of the research projects carried out in healthy subjects to date was that of the Spanish group Riera et al,10 who demonstrated an increase in end-expiratory lung impedance in relation to the use of HFNC among subjects who were in the supine position at an angle of 180°, and in the prone position. Our results were consistent with these findings, but the assessment was made with the subjects in a semi-seated position, which is the most frequently used position in spontaneously ventilated patients with acute respiratory failure. These findings were in agreement with Mauri et al,23,24 who demonstrated that the use of HFNC in the semi-seated position in subjects with acute hypoxemic respiratory failure improved end-expiratory lung impedance and pulmonary gas distribution. However, our study showed that this increase was not only related to the use of HFNC but also to changes in body position (Figs. 2 and 3).
As observed by other researchers,9,10,23 in our study, the use of the HFNC was associated with a decline in breathing frequency. Nevertheless, such a decline was more pronounced among our healthy subjects (a decrease of 4.4 and 6.3 breaths/min for a flow of 30 L/min and 50 L/min, respectively) compared with the subjects evaluated by Mauri et al23 (2 breaths), Corley et al 9 (3.4 breaths), or Riera et al10 (2.7 breaths). The subjects included in the studies by Mauri et al23 and Corley et al9 presented with acute respiratory failure; thus, the breathing frequency decline could have been secondary to the oxygen therapy itself rather than just to the use of high O2 flow. However, the healthy subjects of our study were subjected to a FIO2 of 0.21, which rules out the depressing effect O2 has on breathing frequency when acting on peripheral chemoreceptors.25 Furthermore, Parke et al26 described a significant decrease in breathing frequency among subjects when using HFNC at a flow of 30 L/min compared with semi-seated subjects with no HFNC; however, unlike our findings, the influence of the position on end-expiratory lung impedance was not considered, no differences existed in relation to the flow applied, and an unconventional device at unusual flows (up to 100 L/min) was used.
The breathing frequency reduction associated with the use of the HFNC, according to Pham et al,27 could be due to an improvement in pulmonary compliance caused by the increase in EELV, which, in turn, could decrease the work of breathing and thereby decrease breathing frequency. We were not able to confirm this hypothesis because, without the use of the HFNC, the difference between EELV in subjects in the semi-seated position and in the supine position, though significant, was not accompanied by changes in breathing frequency. In addition, we found a correlation between the use of increasing flows of O2 with HFNC and a progressive decline in breathing frequency. This decrease in breathing frequency could be associated with an improvement in alveolar ventilation28 and a fall in CO2 concentration in conducting airways29,30; whereas other variables related to breathing frequency decrease in critically ill patients, such as improvement in comfort or dyspnea,31 would not be relevant factors among our healthy subjects. Another plausible explanation for the decrease in breathing frequency caused by the use of HFNC at a flow of at least 50 L/min, is the generation of some kind of inspiratory support,7,8 which could translate into an increase of inhaled tidal volume and, consequently, a fall in breathing frequency for the same minute ventilation.
There were limitations of this study. This study was not blinded to the investigators or to the subjects, which could add bias; however, due to the study design, it was impossible to do. An assessment of end-expiratory lung impedance behavior through EIT was made in healthy subjects, which allows for a proper application of the technique that implies an adequate mouth closure and tolerance to high flows, conditions that are difficult to achieve in patients with acute respiratory failure with high ventilatory demand. Therefore, application in daily clinical practice could prove different.32 In addition, it was decided that the assessment would only include end-expiratory lung impedance changes in relation to the use of HFNC at flows of 30 and 50 L/min. Although the use of a flow different from these could have a special impact on end-expiratory lung impedance, the flow range used was the most commonly applied in usual practice. The EIT measurement technique could represent another limitation of the study because it only assessed a relatively limited surface, which related to the transverse plane in relation to where the 16-electrode rubber belt was placed. However, a good correlation was described between the EIT and other, more specific, lung-volume measurement techniques (r2 = 0.92).17
Conclusions
In healthy subjects, the semi-seated position at a 45° angle and the use of HFNC were associated with a significant increase in EELV in both lung regions, which resulted in a greater homogenization of alveolar ventilation. These changes were associated with the increase in the flow used and were accompanied by a significant decrease in breathing frequency. All these effects would decrease the respiratory work load through improvement of the relationship between minute and alveolar ventilation in patients with lung disease as well. More studies are needed for testing this hypothesis.
Footnotes
- Correspondence: Gustavo A Plotnikow PT, 1872 Tomás M de Anchorena Street, 1425 Buenos Aires, Argentina. E-mail: gplotnikow{at}gmail.com
The authors have disclosed no conflicts of interest.
Presented by Mr Plotnikow at the 27th Argentinian Conference of Critical Care, September 2nd, 2017 Córdoba, Argentina.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}