

Abstract
BACKGROUND: An exercise modality that has been gaining significant importance in the rehabilitation of subjects with COPD is resistance training. When considering that patients with COPD present alterations in autonomic cardiac modulation caused by the disease itself, it is necessary to investigate the behavior of the autonomic nervous system in relation to this type of exercise. Thus, the objective of this study was to compare the acute effects of resistance training with elastic tubes, elastic bands, and conventional weightlifitng on the behavior of cardiac autonomic modulation in post-exercise recovery in subjects with COPD.
METHODS: Thirty-four subjects with COPD performed an single session of resistance training divided according to the therapeutic resource used: elastic tubes (n = 10), elastic bands (n = 11), and conventional bodybuilding (n = 13). For analysis of cardiac autonomic modulation, the heart rate was obtained beat to beat at rest and immediately after the end of the session for 60 min in a seated position. Heart rate variability indices were obtained in the time and frequency domains.
RESULTS: The 3 therapeutic resource types used in the single session of resistance training promoted changes in heart rate variability linear indices in the time and frequency domains; however, post-exercise recovery time was similar for all protocols performed.
CONCLUSIONS: After single resistance training the elastic tubes group presented a minimum alteration in the post-exercise recovery of cardiac autonomic modulation in the subjects with COPD; however, at 5 min after exercising, the subjects with COPD had already recovered. Therefore, if the purpose of the training is to restore autonomic cardiac modulation, the use of elastic tubes is suggested, when considering their low cost and versatility.
- heart rate variability
- autonomic nervous system
- physical exercise
- resistance training
- COPD
- rehabilitation
- elastic tubes
Introduction
COPD is a preventable, treatable, but not fully reversible respiratory disease characterized by chronic airway obstruction.1,2 One of the main ways of treating COPD with the goal of improving muscle condition is pulmonary rehabilitation.3,4 Among the therapeutic modalities used in the rehabilitation of patients with COPD, resistance training has been gaining prominence.5 Researchers in the field are currently striving to detect possible treatment alternatives that offer greater versatility and better cost/benefit,6 and, within this perspective, elastic tubes7,8 and bands9,10 have become an important therapeutic possibility.
It should be noted that the updated training methods for patients with COPD are considered to be autonomous modifications that occur during implementation of the training period and a recovery period.11 Thus, heart rate variability has been used as a noninvasive measurement tool to verify the effects of physical exercise on the autonomic nervous system, both in physiological and pathological conditions.12,13
It is known that patients with COPD present with alterations in cardiac autonomic modulation that lead to an increase in resting heart rate and a reduction in heart rate variability, which indicates specifically that their evaluation plays a role in the morbidity and mortality of these patients.14,15 However, in patients with COPD, the influence of different types of resources used in resistance training on cardiac autonomic modulation and post-exercise recovery has been poorly explored. Thus, when considering physical exercise as a stressor agent of of the body withdrawing the body from a condition of homeostasis and producing alterations from metabolic to autonomic,16,17 it is important to study modifications in cardiac autonomic modulation of patients with COPD, which already presents heart rate variability changes caused by the disease itself.15,16
In addition, it is worth reiterating that, among the different types of physical exercises proposed for this population, resistance training has been gaining followers due to its potential benefits. Therefore, it is important to study which type of resistance exercise provides better recovery of autonomic cardiac modulation to ensure that the patient can safely receive a new stimulus, in addition to ensuring patient safety at the end of pulmonary rehabilitation and when prescribing home exercises.
The objective of the present study was to compare the acute effects of resistance training with elastic tubes, elastic bands, and conventional bodybuilding on the behavior of cardiac autonomic modulation in post-exercise recovery in subjects with COPD. It was hypothesized that elastic resistance training would provide greater modification in cardiac autonomic modulation in COPD by generating greater muscle demand because the elastic resistance offers a linear increase in tension from the beginning to the end of the contraction during the movement.7,8
QUICK LOOK
Current knowledge
It is known that patients with COPD present with alterations in cardiac autonomic modulation. Various physical exercises have been proposed in this population to improve health status, including resistance training with elastic resistance. However, identifying the effects of these therapeutic modalities on autonomic cardiac modulation is necessary to ensure safe prescription for the patient.
What this paper contributes to our knowledge
Subjects with COPD using elastic tubes for single resistance training had a minimum alteration in post-exercise recovery of cardiac autonomic modulation, and had already recovered at 5 min post exercise. Therefore, if the purpose of the training is to restore autonomic cardiac modulation, the use of elastic tubes is suggested because of their low cost and versatility.
Method
Population
For this study, data from subjects of both sexes diagnosed with COPD were analyzed according to the Global Initiative for Chronic Obstructive Lung Disease,2 clinically stable without exacerbations or changes in medications for at least 30 d and without participating in any type of physical activity and/or pulmonary rehabilitation in the previous 6 months.
The study did not include volunteers who presented any of the following characteristics: current smokers, the use of drugs that influence autonomic activity of the heart, people with alcoholism, people with known metabolic and/or endocrine disorders, home oxygen therapy, pathological conditions that impede the practice of physical training, unstable COPD, and participation in any other systematized exercise programs. Nonattendance in the training protocol for personal reasons, respiratory exacerbations during the training process, and time series of RR intervals that did not present >95% sinus beats were considered exclusion criteria for the study.
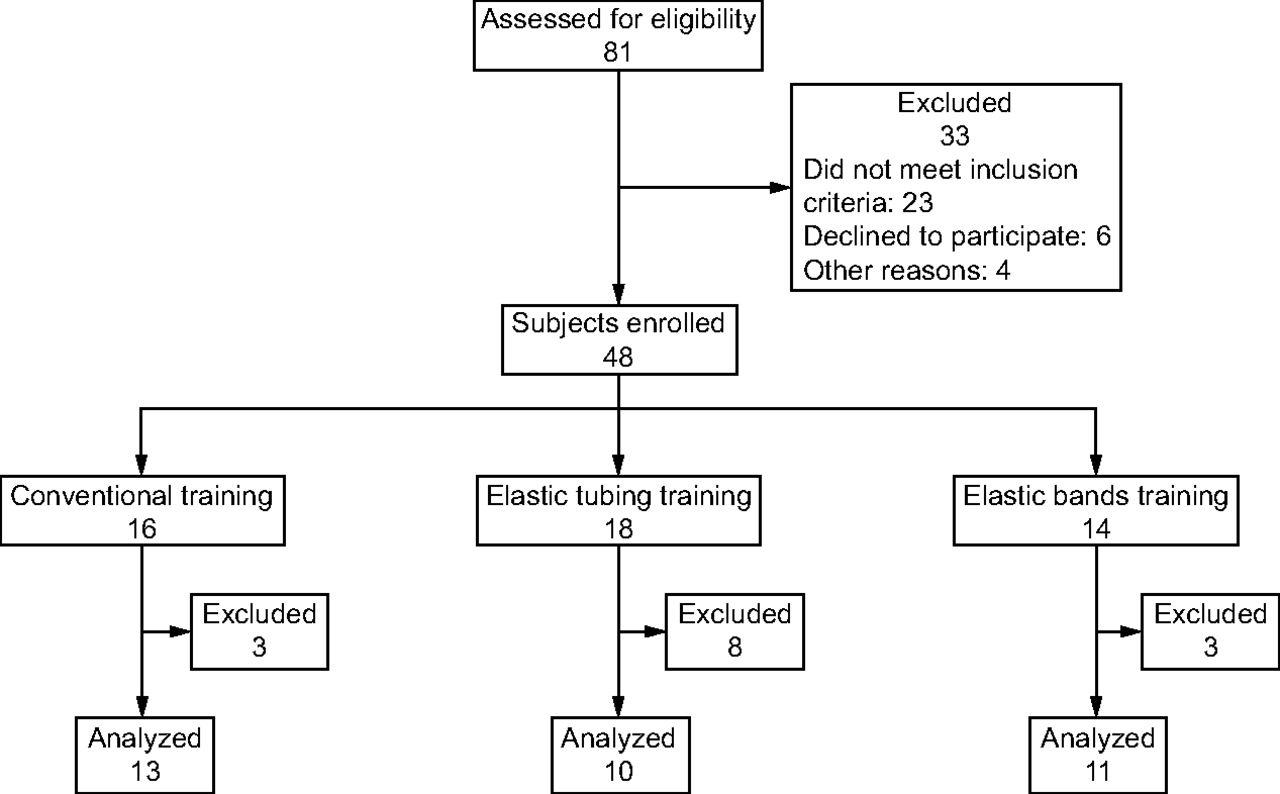
A total of 81 subjects without clinical and respiratory exacerbations with COPD were eligible for the study, and 48 subjects were included. The subjects were randomly allocated to the following 3 groups by drawing lots: conventional training (n = 16), elastic tube training (n = 18), and elastic band training (n = 14). Anonymity was preserved by allocating a number to each subject before the draw. Random assignment was achieved by an independent person who drew the sealed numbers before the start of the intervention. The participants were blinded to the study hypotheses. During the analyses, some volunteers were excluded due to errors in heart rate variability capture, so the final composition of the groups was as follows: conventional training (n = 13; degree II = 5, degree III = 6, degree IV = 2); elastic tube training (n = 10; degree II = 6, degree III = 4); and elastic band training (n = 11; degree II = 3, degree III = 6, degree IV = 2). The sample loss flowchart is presented in Figure 1.

Flow chart. Subjects excluded from final analysis due to mistakes in heart rate variability capture.
The volunteers were informed of the objectives and procedures of this study and, after agreeing, signed an informed consent form. All the procedures used were approved by the research ethics committee of the Universidade Estadual Paulista under protocol number CAAE: 46065315.7.0000.5402 and complied with Resolution 196/96 of the National Health Council. The clinical trial was registered in the Brazilian Registry of Clinical Trials under protocol number RBR-6v9sjj.
Study Design
This was a prospective experimental study started in March 2015 and completed in July 2016. Data collection took place in the Center for Studies and Assistance in Physiotherapy and Rehabilitation of the Faculty of Science and Technology – FCT/UNESP, in the morning to avoid variation in circadian cycle. To reduce the anxiety of the volunteers during the protocols, only a small number of people circulated through the site. Before performing the protocol, the volunteers were instructed to eat a light meal and dress in appropriate and comfortable clothes for the physical effort. In addition, they were instructed not to ingest coffee, black tea, or chocolate. After being instructed on these guidelines, the volunteers gave their written consent and were submitted to the procedures described below.
The collection was performed to verify the autonomic cardiac modulation recovery against the acute performance of 3 different resistance training protocols. On reaching the collection site, the following variables were verified: age, weight, stature, systolic and diastolic blood pressure, oxygen saturation, subjective effort scale (Borg), and breathing frequency. Information on the volunteer was identified through the medical history with questions regarding any severe cardiovascular-, neuromuscular-, skeletal-, or lung-associated diseases, and any history of diseases and current clinical state (medications currently prescribed, and the presence of diabetes, arterial hypertension, and smoking risk factors). Anthropometry was performed to characterize the population and to investigate the presence of excess weight and obesity.18 Spirometry was performed to confirm the diagnosis of COPD and classify the severity of the air flow.19
A heart rate monitor (model RS800cx; Polar Electro Oy, Kempele, Finland) was then placed on the volunteers to record the pulse rate throughout the protocol, while they remained at rest in a sitting position for 20 min. The participants were instructed not to talk, make sudden movements, or sleep during this period. At the end of the rest period, the volunteers performed resistance training according to their previously randomized group: conventional, elastic bands, and elastic tubes. Immediately after the end of the training, the volunteers were again instructed to remain in a seated position for 60 min, which thus initiated the heart rate variability recovery period. The heart rate variability analysis protocol was established based on studies that analyzed post-exercise recovery.20,21
Training Protocols
The exercise session lasted 60 min, and, at the beginning and end of the session, the vital signs were verified and overall stretches were performed, such as of the trunk musculature and the upper and lower limbs. For the 3 protocols, exercises were performed for shoulder flexion, elbow flexion, shoulder abduction, knee extension, and knee flexion, with 2 sets of 15 repetitions and a passive rest interval of 1–2 min between sets. For the resistance training, the load used for each subject was defined according to the maximum repetition test.
For the maximum repetitions test, the subject was required to perform 15 maximum repetitions; the number of repetitions used for the initial test. Therefore, the test was valid when performed with a load (tubes, bands, or machines) that allowed the execution of 15 maximum repetitions. The test was considered invalid if the subject did not complete the range of motion and/or compensations. Both the test and the training were tolerated to execute up to 2 maximum repetitions. The participants performed up to 3 trials with a 2-min interval between attempts, and verbal stimulation was given to the subjects throughout the trials.
For the conventional resistance training, bodybuilding equipment (Ipiranga, São Paulo, Brazil) was used, being a simple pulley for the upper limbs and a flexor and extensor chair for the lower limbs. Resistance training with elastic tubes was performed by using Lemgruber latex elastic tubes, of different diameters and thicknesses, in addition to metal rings, bundles (plastic cable) for fixing the elastic tubes to the rings, and a specific chair with hooks for fixing the tubes and handles for the upper limbs. For the resistance training with elastic bands, a variety of Theraband elastic bands (Theraband®, Akron, Ohio) were used (yellow [1.3-kg resistance with 100% elongation percentage], red [1.8 kg], green [2.3 kg], blue [3.2 kg], and black [4.4 kg]). Determination of the length of the elastic tubes and elastic bands was performed according to the distance from the upper or lower limb of each subject to the hook (fixed point) on the chair. Thus, the length differed from one subject to another according to the recommendations proposed by Ramos et al.8
Three senior physical therapists who specialized in pulmonary rehabilitation and/or musculoskeletal rehabilitation (FFL, BSAS and APCFF) and one physical therapist (FZ) were responsible for the assessment and management of the exercise sessions in the three intervention groups. The physical therapists provided close supervision during the sessions for all training protocols. The researcher who performed the data analyses was blinded to group allocation throughout the study.
Analysis of Heart Rate Variability
Heart rate variability analysis was performed from the series of RR intervals captured by using the Polar Electro Oy and linear methods, analyzed in the time and frequency domains.13 For this analysis, the time series of RR intervals was initially subjected to digital filtering by using Polar Pro Trainer software, complemented by manual filtering for elimination of premature ectopic beats and artifacts. Only series with >95% sinus beats were included in the study.22 Visual analysis of the time series was performed to verify the absence of ectopic artifacts or beats that could interfere with the heart rate variability analysis.
For the analysis of heart rate variability in the time domain, the root-mean square of differences between adjacent normal RR intervals in a time interval (rMSSD) and standard deviation of all normal RR intervals (SDNN)13 were used which reflect respectively vagal modulation and global variability. In the frequency domain, spectral components of low frequency (LF) (global variability) and high frequency (HF) (vagal modulation), in ms,2 and normalized units (nu), and the relationship between them (LF/HF) were used.13 The frequency bands used for each component were LF = 0.04–0.15 Hz and HF = 0.15–0.40 Hz. The spectral analysis was calculated by using fast Fourier transform.13 All heart rate variability indices were processed by using Kubios HRV software (Biosignal Analysis and Medical Imaging Group, Kuopio, Finland), version 2.0.23
The series of RR intervals were analyzed at the following moments: M1 (5 min at rest), M2 (5 min initial recovery), M3 (5th-10th min of recovery), M4 (15th-20th min of recovery), M5 (25th-30th min of recovery), M6 (40th-45th min of recovery), and M7 (55th-60th min of recovery), which contained 256 consecutive RR intervals in these intervals.12
Statistical Analysis
For analysis of the data of the population profile, the descriptive statistical method was used, and the results are presented as mean ± SD, median, minimum and maximum numbers, and CI. The normality of the data was evaluated by using the Shapiro-Wilks test. For comparison of the characteristics of the sample, one-way analysis of variance (ANOVA) was used with the Tukey honest significant difference test (age, weight, and body mass index) and the Kruskal-Wallis test with Dunn test (height).
The comparisons of heart rate variability indices among the protocols (conventional vs elastic tube vs elastic band) and moments (rest vs recovery times) were performed by using the technique of ANOVA for models of repeated measurements in the 2-factor scheme (mixed ANOVA). Repeated measurement data were checked for breach of sphericity by using the Mauchly test, and the Greenhouse-Geisser correction was used when sphericity was violated.
For analysis of the moments (rest vs recovery times), the Bonferroni test was used for parametric or the Dunnett test for non-parametric distribution and the analysis of the different moments between the groups was carried out by using one-way ANOVA or the Kruskal-Wallis test. Statistical significance was set at 5% for all analyzes.
The sample was calculated based on the study by Santos et al,24 in which an index of instantaneous recording of beat-to-beat variability (SD1) (reflecting vagal modulation) was selected. The difference to be detected was 7.97 ms and the SD was 6.45 ms. The significance level for the sample calculation was 5%, with a test power of 80% and a 2-tailed hypothesis test. The value obtained from the sample calculation was 10 subjects per group.
Results
The 3 groups analyzed did not present statistical differences in relation to the variables age, weight, height, or body mass index; therefore, they were considered homogeneous (Table 1). For the heart rate variability indices during recovery, the 2-way ANOVA analyzes showed that, during recovery, there was a moment effect for mean RR, rMSSD and HF [ms2] (P = .01). There was no effect among the groups for any index analyzed (Mean HR, P = .37; SDNN, P = .38; rMSSD, P = .18; LF [nu], P = .97; HF [nu], P = .97; LF [ms2], P = .43; HF [ms2], P = .13; LF/HF ratio, P = .95), in addition to which there were no moment or group interactions (Mean HR, P = .22; SDNN, P = .88; rMSSD, P = .45; LF [nu], P = .27; HF [nu], P = .28; LF [ms2], P = .66; HF [ms2], P = .36; and LF/HF ratio, P = .46).
Age, Weight, BMI, and Height of the 3 Groups Analyzed
The results of the mean HR variable in the rest and recovery conditions in the 3 groups studied are presented in Figure 2. For the elastic tubes group, there was a statistical difference at M2 in comparison with M1. For the elastic bands group, M2 and M3 presented significant differences in relation to M1. The conventional group did not present significant statistical differences between moments.

Mean ± SD Mean HR index in the elastic tubes, elastic bands, and conventional training groups in the rest and recovery conditions. M1 = final 5 min of rest; M2 = 5 min initial recovery; M3 = 5th-10th min of recovery; M4 = 15th-20th min of recovery; M5 = 25th-30th min of the recovery; M6 = 40th-45th min of recovery; M7 = 55th-60th min of recovery. Letters denote the comparison between a = moments only in the tubes training and b = moments in the elastic tubes training and elastic bands training.
The results of the statistical indices of heart rate variability analyzed in the time domain under the rest and recovery conditions in the 3 groups studied are presented in Figure 3. The SDNN index did not present statistically significant differences between moments for the groups analyzed. For the rMSSD index, which represents parasympathetic modulation, the elastic tube group presented a statistically significant difference at M2 when compared with M1.
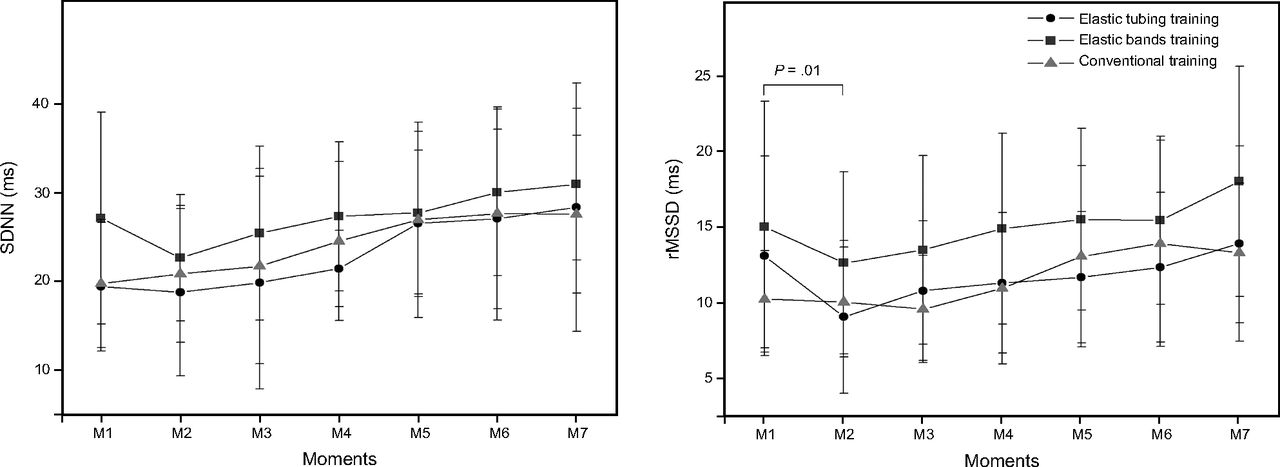
Mean ± SD of the SDNN and rMSSD indices in the elastic tubes, elastic bands, and conventional training groups in the rest and recovery conditions. M1 = final 5 min of rest; M2 = 5 min initial recovery; M3 = 5th-10th min of recovery; M4 = 15th-20th min of recovery; M5 = 25th-30th min of recovery; M6 = 40th-45th min of recovery; M7 = 55th-60th min of recovery. P value for comparison between moments only in the tubes training.
The results of heart rate variability analyzed in the frequency domain under the rest and recovery conditions in the 3 groups studied are presented in Figure 4. For the LF [nu], HF [nu], LF [ms2], and LF/HF ratio, no statistical differences were observed among the moments for the 3 groups analyzed. For the HF [ms2] index, representative of parasympathetic modulation, the elastic tubes group presented a statistical difference at M2 when compared with M1.
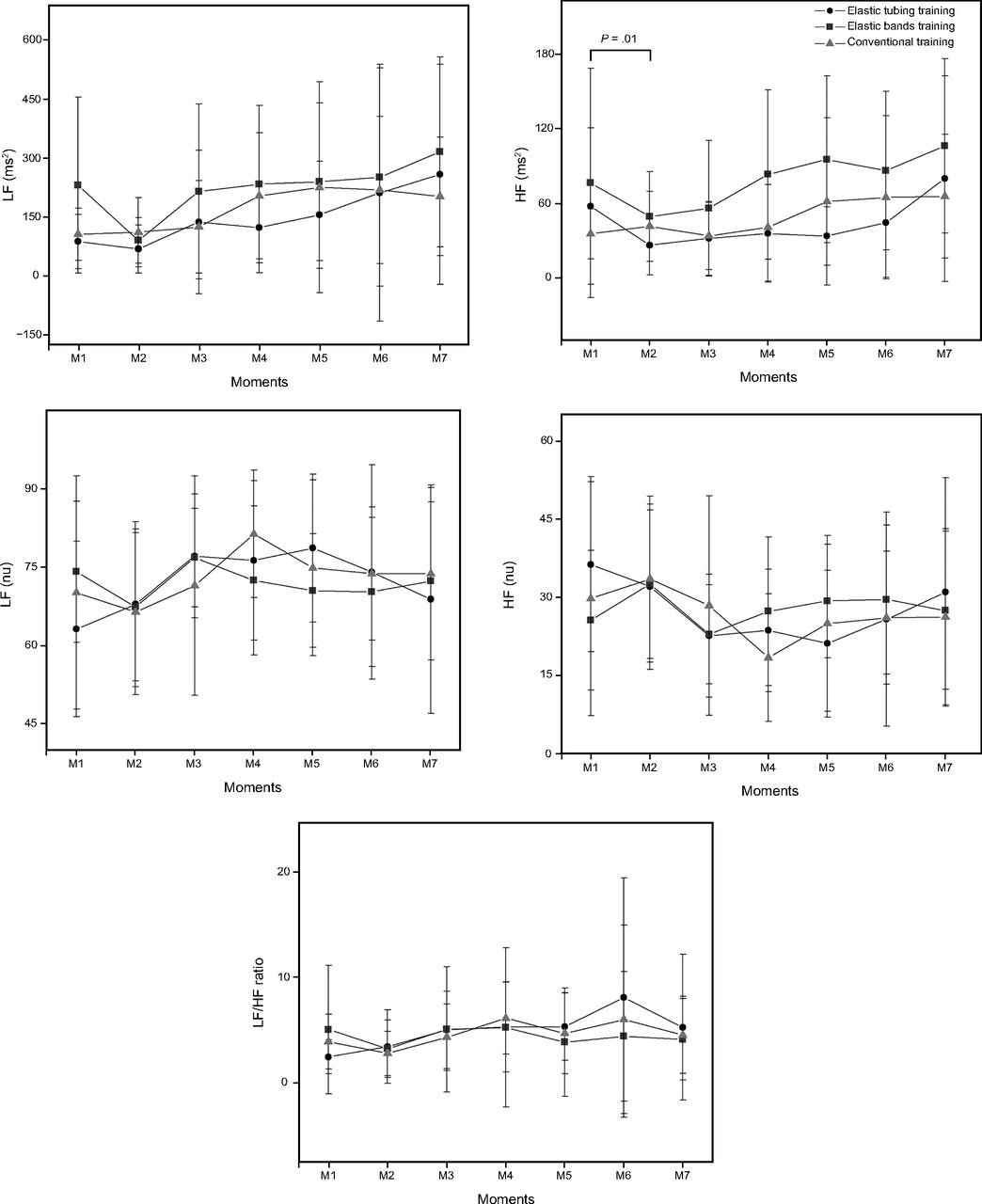
Mean ± SD of the LF (nu), HF (nu), LF (ms2), HF (ms2), and LF/HF ratio in the elastic tubes, elastic bands, and conventional training groups in the rest and recovery conditions. M1 = final 5 min of rest; M2 = 5 min initial recovery; M3 = 5th-10th min of recovery; M4 = 15th-20th min of recovery; M5 = 25th-30th min of recovery; M6 = 40th-45th min of recovery; M7 = 55th-60th min of recovery. P value for comparison between moments only in the tubes training.
Discussion
The present study aimed to evaluate the effects of different types of resistance training (conventional vs elastic tubes vs elastic bands) in post-exercise recovery, single session on cardiac autonomic modulation in subjects with COPD. The results showed that heart rate increased after a resistance exercise in subjects with COPD; however, it recovered quickly. There was minimal change in heart-rate variability during recovery, with little difference between exercise strategies and heart-rate recovery and variability. There were minimum changes with the elastic tubes, whereas subjects had no differences in heart rate or autonomic modulation in the elastic-bands or conventional groups.
The pertinent literature addresses the chronic effects of resistance training in subjects with COPD; however, there is a lack of evidence to demonstrate the behavior after a single session of this type of training on cardiac autonomic modulation. This highlights the importance of the present study and characterizes it as the first study to our knowledge to verify the influence of different types of therapeutic resources against a single session of resistance exercise.
Although there are studies that describe the behavior of heart rate variability after aerobic exercise,25–28 few describe the autonomic response after resistance exercise. The studies that analyzed heart rate variability in the recovery period after resistance exercise observed increases in sympathetic modulation and reductions in parasympathetic modulation.29,30 However, previous studies do not compare post-exercise recovery in subjects with COPD using different therapeutic resources for resistance training. In addition, this literature does not present data showing the exact moment of autonomic nervous system recovery, considering a long recovery period.
It is known that, during the performance of resistance exercise, sympathetic activation occurs to supply the metabolic and cardiorespiratory demands required by the effort.31 This is a hypothesis that may explain the findings in the mean HR, in which an increase in values in the recovery period was observed for a maximum of 10 min, which thus indicates sympathetic predominance due to exercise.31
During the recovery period, the heart rate gradually returns to basal values, mainly due to parasympathetic reactivation.31,32 The end of exercise promotes a loss of central control and cessation of baroreflex activation as well as other mechanisms that contribute significantly to increased parasympathetic modulation.32,33 This aspect can be observed by the behavior of the rMSSD index, which reflects parasympathetic modulation, which, at M2, corresponding to the initial 5 min of recovery, demonstrated a decrease in the values in relation to rest. These findings indicate sympathetic modulation caused acutely by resistance training, as these values approached baseline conditions (M1) at other moments, demonstrating a reactivation of parasympathetic modulation.
With regard to parasympathetic regulation after resistance exercise, Heffernan et al29 showed that 25 min after the end of the exercise, the HF index, which reflects parasympathetic modulation,13 was reduced when compared with aerobic exercise performed at 65% V̇O2 peak. These results may point to relative safety with respect to possible cardiovascular events when performing resistance exercise compared with maximum aerobic exercise.29 Oliveira et al34 also found a reduction in parasympathetic modulation after an exercise session in healthy men undergoing resistance training for 12 weeks when compared with maximum aerobic exercise, which once again reinforces the importance of evaluating cardiac autonomic modulation during the recovery period.
Mohammed et al35 verified, in a systematic review, that there is strong evidence to support the depression of baroreflex sensitivity in subjects with COPD. Possible contributors to this depression include alterations in intrathoracic pressure, hypoxia, and oxidative stress, which are common in patients with COPD. The baroreflex mechanism plays an important role in cardiovascular function, especially in the short-term regulation of blood pressure and heart rate.35 However, in our study, the impaired condition of COPD subject did not appear to influence post-exercise recovery following resistance training with different therapeutic resources, although further studies are necessary to prove this hypothesis.
The elastic tubes group was the only training group that presented statistical differences at M2 in relation to M1. Elastic resistance promotes greater physical demand required by the therapeutic resource because it provides a linear increase in tension from the beginning to the end of the contraction during the movement.7,8 This results are not unfavorable to the use of elastic tubes, as at M3 (5–10 min) these subjects had already recovered. In other words, subjects had reached resting baseline values at 5 min after cessation of the single session, demonstrating that they were prepared for a new stimulus from an autonomic point of view. In addition, studies show that the gain in muscular strength with elastic tubes is similar to conventional bodybuilding and, therefore, in view of the cost/benefit, elastic tubes represent a resource to be prescribed for resistance exercises.8
The SDNN index, which reflects global variability, demonstrated an increase in the recovery moments for all the groups, which indicated an increase in the time of variation of the RR intervals due to post-exercise vagal reactivation; however, no statistical difference was observed between moments and groups. Lima et al30 carried out a study to verify the effects of strength exercise on heart rate variability in young people and showed that, after resistance training at 70% of one maximum repetition, the global variability presented an increase during the recovery period compared with the pre-exercise moment.
For the HF index, which also reflects parasympathetic modulation, for the elastic tubes group, there was a difference at M2 in relation to M1 similar to rMSSD index. Javorka et al32 evaluated heart rate variability in healthy men after a functional capacity test and observed reductions in the HF index during exercise and a progressive increase during recovery, which indicated parasympathetic reactivation in the spectral indices. These researchers also verified an increase in the LF index during recovery and indicated that this index is directly influenced by modifications in vagal modulation that promote fluctuations in the spectral bands or are indirectly influenced by changes in the sensitivity of the baroreflex.32
Nicolino et al36 evaluated cardiac autonomic modulation after an acute resistance exercise session at different intensities of one maximum repetition in subjects with COPD. The HF and LF indices were higher at all recovery moments compared with the other indices in the training intensities of 60% and 90% of one maximum repetition. In addition, there was no statistical difference between the training protocols, which showed that the recovery of autonomic modulation in this population was similar regardless of the exercise intensity.
Karavirta et al37 found no effects of 21 weeks of resistance training on frequency-domain measures in healthy men age 40–67 y after twice weekly resistance training that consisted of 7–10 exercises. Training started with 3 sets of 15–30 repetitions at 40–60% of one maximum repetition and ended with 3 sets of 5–8 repetitions at 70– 85% of one maximum repetition. Similarly, Wanderley et al38 demonstrated no change in HF after 8 months of resistance training in older adults with an age of 68 ± 5 y, whether they presented uncontrolled hypertension or not.
Again, it should be emphasized that therapeutic resources with elastic resistance offer greater resistance at the end of the movement10; are highly versatile, which allows the patient to perform the exercise to its full range;7 are more practical because they require minimum space for training; and can be performed at home with a large number of movement arches, including both concentric and eccentric contractions.39,40 Thus, elastic tubes, despite modifying the rMSSD and HF [ms2] indices, were shown to be a more practical and low-cost method when compared with elastic bands and conventional bodybuilding apparatus.8
As in the present study, Nicolino et al36 did not observe statistical differences in the LF/HF ratio during the recovery period after resistance exercise. It is believed that the autonomic nervous system was able to act efficiently to restore and maintain the body's homeostasis in the face of physical effort. Such results may demonstrate the ability of patients with COPD to tolerate resistance training performed with different therapeutic resources.
Resistance training has been recommended to improve the autonomic function of patients with COPD.24,41 Santos et al24 investigated the influence of resistance training on cardiac autonomic modulation by using heart rate variability geometric methods in subjects with COPD. After 2 months of training, which ranged from 60 to 80% of one maximum repetition, the researchers observed a significant increase in the indices that reflect vagal modulation and global variability, and high beat-to-beat dispersion, which indicated an improvement in cardiac autonomic modulation as well as improved peripheral muscle strength.24
Ricci-Vitor et al41 found that resistance training was able to positively influence cardiac autonomic modulation of subjects with COPD when evaluated by the temporal and spectral indices of heart rate variability. However, it is again worth emphasizing that these studies24,41 show the chronic effects of training, whereas the present study demonstrated the acute results of cardiac autonomic after a session of resistance exercise.
As a limitation of the study, we pointed out the small sample size due to the specific geographic location and losses during the data collection process and analysis of heart rate variability. In addition, we should mention the influence of breathing frequency because it was not controlled as well and the lack of stratification of subjects according to severity of COPD.
It is important to study the heart rate variability indices in post-exercise recovery because an increase in sympathetic modulation in patients with COPD is associated with a higher rate of morbidity and mortality.42 In addition, low levels of parasympathetic reactivation in the recovery period can be considered an important risk factor for cardiac mortality.43 From an autonomic point of view, it can be inferred that the protocols proposed in this study can be safely applied because reactivation of the autonomic nervous system in the recovery period occurred in an efficient way.
Conclusions
The elastic tubes group, after single resistance training, promoted a minimum alteration in the post-exercise recovery of cardiac autonomic modulation in subjects with COPD, characterized by a decrease in the parasympathetic modulation immediately after exercise; however, at 5 min after exercise, the subjects with COPD had already recovered. Therefore, when considering its low cost and versatility, elastic tubes are a therapeutic resource option for resistance training in subjects with COPD.
Footnotes
- Correspondence: Franciele M Vanderlei PhD, Ciências e Tecnologia – FCT/UNESP, Departamento de Fisioterapia, Rua Roberto Simonsen 305, Presidente Prudente – SP CEP 19060-900, Brazil. E-mail: franmvanderlei{at}gmail.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}