

Abstract
BACKGROUND: The balance of oxygen delivery and consumption is essential in patients who are critically ill. Mixed venous oxygen saturation (Sv̄O2) is a standard method to evaluate oxygen delivery and consumption during anesthesia. However, Sv̄O2 is monitored through a pulmonary artery catheter, which is invasive. Regional cerebral oxygenation (rScO2) reflects oxygen saturation in a small region of the frontal lobes and is monitored noninvasively through near-infrared spectroscopy. In the present study, the correlation between rScO2 and Sv̄O2 was calculated during off-pump coronary artery bypass grafting surgery to determine whether a positive correlation exists between rScO2 and Sv̄O2.
METHODS: A total of 56 subjects were consecutively enrolled in the study. Then rScO2 and Sv̄O2 were simultaneously monitored. The parameters were recorded at 5 time points: T1, 10 min after intubation (1.0 FIO2 for 10 min); T2, 20 min after intubation (0.60 FIO2 for 10 min); T3, at the end of the revascularization of the left anterior descending artery (0.60 FIO2); T4, after protamine infusion (0.60 FIO2); and T5, 10 min after protamine infusion (1.0 FIO2 for 10 min). The correlation between rScO2 and Sv̄O2 and the variation trend between rScO2 and Sv̄O2 when FIO2 increased from 0.60 to 1.0 were analyzed.
RESULTS: There was a significant positive correlation between rScO2 and Sv̄O2 at these 5 time points (r2 = 0.77, 0.81, 0.70, 0.83, and 0.92, respectively). There also was a significant positive correlation between Δ rScO2 and Δ Sv̄O2 (n = 112, r2 = 0.72, P < .001). Linear regression analysis revealed that Sv̄O2 had a positive correlation with rScO2 and cardiac output (r2 = 0.68, P = .013).
CONCLUSIONS: There was a positive correlation between rScO2 and Sv̄O2 during off-pump coronary artery bypass grafting surgery, and there also was a positive correlation in the variation trend between rScO2 and Sv̄O2.
Introduction
Maintaining adequate oxygen saturation is essential for patients who are critically ill. Mixed venous oxygen saturation (Sv̄O2) remains the accepted standard during anesthesia to evaluate the balance of oxygen delivery and consumption, especially during cardiac surgery.1 Sv̄O2 is monitored through the pulmonary artery catheter, but many complications are associated with pulmonary artery catheter placement, such as bleeding, arrhythmia, and pulmonary artery rupture.2 Hence, this cannot be routinely used during anesthesia. A noninvasive tool to monitor systemic oxygen balance would have a much wider application.
Near-infrared spectroscopy can noninvasively and continuously estimate the regional oxygen delivery-consumption balance in an underlying tissue. It is based on oxyhemoglobin and deoxyhemoglobin each having their own particular optical absorption characteristics.3 Near-infrared spectroscopy can monitor regional cerebral oxygen saturation (rScO2),4 which reflects oxygen saturation in a small region of the frontal lobes. Furthermore, rScO2 has been used in preterm and term neonates,5 in patients during cardiac surgery6 neurosurgery, and in patients with head trauma.7 Moreover, rScO2 can detect disturbances of regional tissue perfusion and oxygenation,8 and predict low output syndrome,9 cognitive decline, and a prolonged hospital stay after cardiac surgery.10
Results of one study indicated that rScO2 is useful for indicating global oxygen delivery and consumption,11 and the correlation between rScO2 and Sv̄O2 has been studied in adult and pediatric cardiac surgery patients.12,13 To determine whether rScO2 can be a noninvasive technique to reflect systemic oxygen balance, we investigated the correlation between rScO2 and Sv̄O2 in off-pump coronary artery bypass grafting surgery under both 0.60 and 1.0 FIO2 during mechanical ventilation. The purpose of this study was to determine whether both rScO2 and Sv̄O2 could be applied, instead of one or the other.
QUICK LOOK
Current knowledge
Mixed venous oxygen saturation (Sv̄O2) is a standard method to evaluate global oxygen delivery and consumption balance during anesthesia. The regional cerebral oxygen saturation (rScO2), which can be noninvasively monitored by near-infrared spectroscopy, indicates the regional cerebral oxygen saturation and provides information on regional cerebral oxygen delivery and consumption balance. Previous studies showed that the rScO2 could indicate global oxygen delivery and consumption, and there was correlation between rScO2 and Sv̄O2 under some condition, but whether the correlation was existed during off-pump coronary artery bypass grafting surgery was not explored.
What this paper contributes to our knowledge
rScO2 would be adequate in reflecting Sv̄O2 and the variation trend of Sv̄O2 during off-pump coronary artery bypass grafting surgery, the change in FIO2 can simultaneously influence the rScO2 and Sv̄O2 value, and the variation trend of rScO2 and Sv̄O2 was consistent.
Methods
The study protocol of this prospective observational study was approved by the ethics committee of the First Affiliated Hospital of Xi'an Jiaotong University. Written informed consent was obtained from all the subjects. From January to December 2015, a total of 56 subjects were enrolled into this study. Inclusion criteria were the following: age >18 y and elective off-pump coronary artery bypass grafting surgery for coronary heart disease. Exclusion criteria were the following: combined other cardiac surgeries, contraindication of pulmonary artery catheter placement, stroke, cerebrovascular disease, intra-aortic balloon pump or other ventricle support devices used during the operation, failure to insert the pulmonary artery catheter, and death during the operation. The enrollment procedure is shown in Figure 1.

Flow chart. PAC = pulmonary artery catheter.
Anesthesia Management
The subjects were routinely monitored by electrocardiogram, pulse oxygen saturation, arterial blood pressure, and central venous pressure. Anesthesia was induced by 0.05–0.10 mg/kg midazolam, 0.5–1.0 μg/kg sufentanil, 0.2–0.3 mg/kg etomidate, and 0.9 mg/kg rocuronium, which was maintained by 1.0–1.5% sevoflurane and 4–8 mg/kg/h propofol, muscle relaxation was achieved by rocuronium. Mechanical ventilation was performed in the volume control mode with a breathing frequency of 10 breaths/min and a tidal volume of 6–12 mL/kg. The tidal volume was adjusted to maintain the end-tidal carbon dioxide pressure at 35–45 mm Hg. FIO2 was 1.0 during anesthesia induction. This was reduced to 0.60 at 10 min after intubation and increased to 1.0 again after protamine infusion.
Sv̄O2 and rScO2 Measurements
Sv̄O2 and rScO2 were simultaneously monitored in all the subjects. After anesthesia induction, the pulmonary artery catheter (Swan-Ganz Continuous Cardiac Output Thermodilution catheter, Edwards Lifesciences, Irvine, California) was inserted via an 8.5 French sheath placed in the right internal jugular vein for all the subjects. Sv̄O2 was continuously measured through the pulmonary artery catheter connected to a Vigilance II monitor (Edwards Lifesciences). The location of the pulmonary artery catheter was verified by pressure curve analysis. The rScO2 was continuously measured by near-infrared spectroscopy. The near-infrared spectroscopy sensors (at a wavelength of 700–900 nm) were placed on the right side of the forehead with a flexible, self-adhesive bandage wrapped around the head. These sensors were connected to a EGOS-600A cerebral oximeter (EnginMed, Suzhou, China).
Data Collection
Next, rScO2 and Sv̄O2 were recorded at 5 time points: T1, 10 min after intubation (mechanical ventilation with 1.0 FIO2 for 10 min); T2, 20 min after intubation (mechanical ventilation with 0.60 FIO2 for 10 min); T3, the end of the revascularization of the left anterior descending artery (mechanical ventilation with 0.60 FIO2); T4, after protamine infusion (mechanical ventilation with 0.60 FIO2); and T5, 10 min after protamine infusion (mechanical ventilation with 1.0 FIO2 for 10 min). The demographics were recorded for all the subjects. Mean arterial blood pressure, central venous pressure, mean pulmonary artery pressure, cardiac output (Q̇T), PaO2/FIO2, PaCO2, and hemoglobin concentration were also recorded at these 5 time points.
Statistical Analysis
Continuous variables are presented as mean ± SD, and categorical variables are presented as numbers. Repeated-measures analysis of variance was used to assess the difference of mean arterial blood pressure, central venous pressure, mean pulmonary artery pressure, Q̇T, PaO2/FIO2, PaCO2, hemoglobin, rScO2, and Sv̄O2 among the time points. The correlation between Δ rScO2 and Δ Sv̄O2 was evaluated by using the Pearson correlation coefficient. Linear regression analysis was calculated among Sv̄O2 and rScO2, Q̇T, mean arterial blood pressure, central venous pressure, mean pulmonary artery pressure, hemoglobin, PaCO2, and PaO2/FIO2. Data were analyzed by using SPSS 17.0 for Windows (SPSS, Chicago, Illinois). Statistical significance was defined as P < .05.
Results
Subject Demographics and Details of the Operation
From January to December 2015, a total of 56 subjects were enrolled into the present study. Subject demographics and operation details are shown in Table 1.
Demographic Data and Details of Operations of the Subjects
Hemodynamic Data and Arterial Blood Gas Analysis at 5 Time Points During Off-Pump Coronary Artery Bypass Grafting Surgery
There was no significant difference in PaO2/FIO2, PaCO2, and hemoglobin among the 5 time points. The central venous pressure, mean arterial blood pressure, and mean pulmonary artery pressure were significantly higher at T3 than at the other time points, and Q̇T was significantly lower at T3 and significantly higher at T5 than the other time points. These data are shown in Table 2.
Hemodynamic Data and Arterial Blood Gas Analysis
Correlation Between rScO2 and Sv̄O2 Among the 5 Time Points
Sv̄O2 and rScO2 were significantly higher at T5 than at the other time points. There was a positive correlation between rScO2 and Sv̄O2 at the 5 time points. The data are presented in Table 3.
The Correlation Between Sv̄O2 and rScO2
Correlation of the Variation Trend Between rScO2 and Sv̄O2 Under Different FIO2
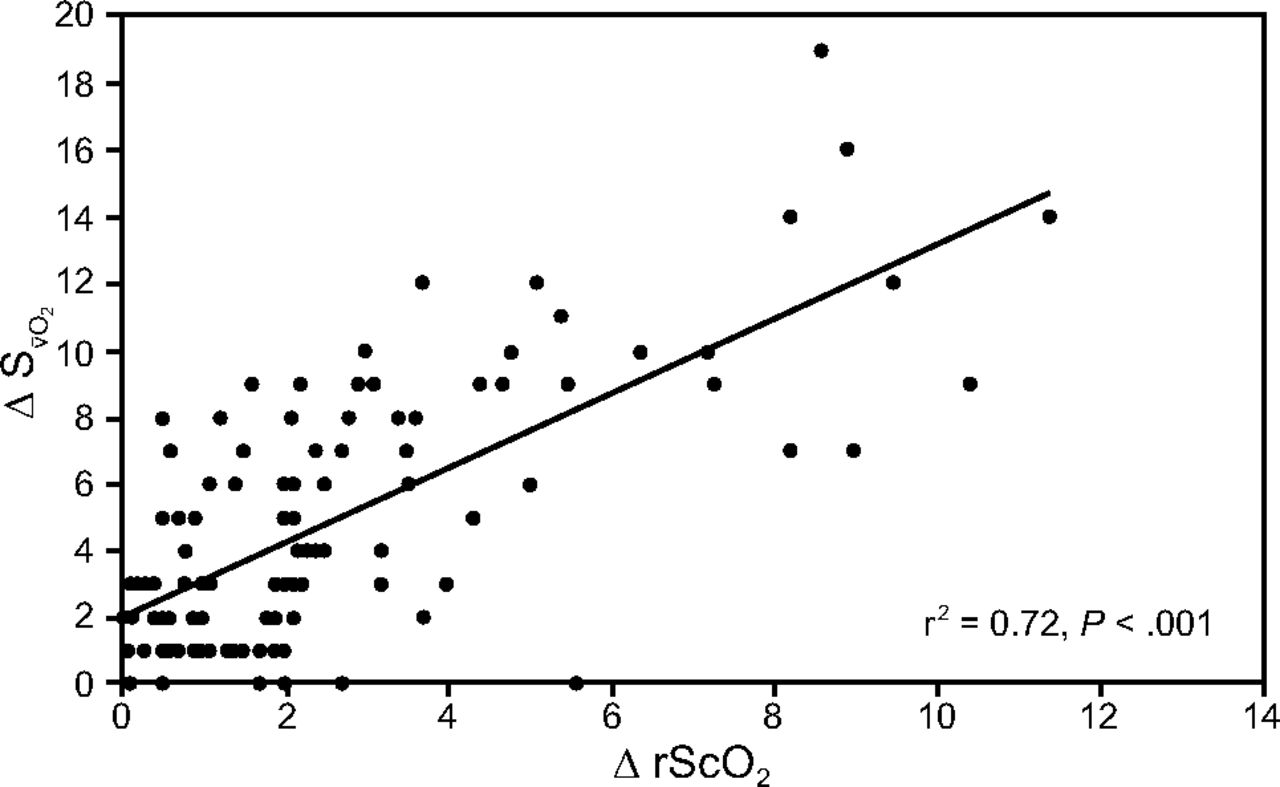
rScO2 and Sv̄O2 decreased when FIO2 decreased from 1.0 to 0.60 (T1 to T2), and increased when FIO2 increased from 0.60 to 1.0 (T4 to T5). The Δ Sv̄O2 was defined as Sv̄O2 (T1) − Sv̄O2 (T2) and Sv̄O2 (T5) − Sv̄O2 (T4), whereas Δ rScO2 was defined as rScO2 (T1) − rScO2 (T2) and rScO2 (T5) − rScO2 (T4). The mean ± SD Δ Sv̄O2 was 4.7 ± 4.1, and the mean ± SD Δ rScO2 was 2.5 ± 2.5. The variation trend between rScO2 and Sv̄O2 was consistent (r2 = 0.72, P < .001) (Fig. 2). Linear regression analysis was performed to examine the variables that best predict Sv̄O2. Then rScO2, Q̇T, mean arterial blood pressure, central venous pressure, mean pulmonary artery pressure, hemoglobin, PaCO2, and PaO2/FIO2 were used in the model. The linear regression analysis revealed that Sv̄O2 was positively correlated with rScO2 and Q̇T (r2 = 0.68, P = .01). The regression equation was Sv̄O2 = −16.082 + 1.393 × rScO2 + 1.304 × Q̇T.

Correlation between the change in the regional cerebral O2 saturation (ΔrScO2) and the change in the mixed venous O2 saturation (ΔSv̄O2).
Discussion
In the present study, a moderate-to-strong positive correlation was found between rScO2 and Sv̄O2 during off-pump coronary artery bypass grafting surgery. There also was a positive correlation on the variation trend between rScO2 and Sv̄O2 when FIO2 was changed.
The rScO2, which can be noninvasively monitored by near-infrared spectroscopy, indicates the rScO2 and provides information on rScO2 delivery and consumption balance. Sv̄O2 provides information on global oxygen delivery and consumption balance, and can be used as an indicator of the adequacy of whole-body oxygen, including venous saturation of the brain and of the upper and lower extremities.14 However, the trend of using a pulmonary artery catheter to monitor Sv̄O2 has declined due to complications.15
Although rScO2 reflects oxygen saturation in the small region of the frontal lobes and depends on cerebral perfusion and metabolism, Sv̄O2 represents the venous blood oxygen saturation of all organs and is dependent on whole-body oxygen delivery and consumption. Because blood in cerebral tissues mainly consists of the venous compartment, rScO2 is correlated closer to venous saturation than to arterial saturation.16 Hence, a positive correlation was found between rScO2 and Sv̄O2 in the present study. Because the variation range was greater in Sv̄O2 than in rScO2, there was a different r2 between rScO2 and Sv̄O2 at each time point.
Previous studies show that rScO2 can reflect global oxygen delivery and consumption balance. Ginther et al17 found that the correlation coefficient between cerebral near-infrared spectroscopy and superior vena cava oxygen saturation was 0.77 during cardiopulmonary bypass. During the varying hemodynamic conditions in subjects undergoing transapical transcatheter aortic valve implantation, rScO2 could reflect Sv̄O2.18 Furthermore, Schön et al19 found a positive correlation between rScO2 and Sv̄O2 in awake and spontaneously breathing subjects after cardiac surgery. Weiss et al20 concluded that rScO2 is associated with central venous oxygen saturation. Kirshbom et al21 found that rScO2 can reflect systemic perfusion in awake children with a single ventricle. Other studies found a positive correlation among rScO2, Sv̄O2 and central venous oxygen saturation in pediatric cardiac surgery subjects.22,23 Furthermore, a positive correlation between rScO2 and Sv̄O2 was also found during extracorporeal membrane oxygenation in a porcine model.24
Many factors can influence the rScO2 value. Dullenkopf et al12 found that there was a fair-to-moderate correlation in rScO2 with hemoglobin concentration and the cardiac index in adult subjects after cardiac surgery. Jugular bulb oxygen saturation, which can indicate rScO2,25 decreased during coronary artery anastomosis in off-pump coronary artery bypass grafting surgery.26 Hu et al27 found that rScO2 was positively correlated to cerebral perfusion pressure (approximately equal to mean arterial blood pressure–central venous pressure). In the present study, we found that Sv̄O2 was positively correlated with rScO2 and Q̇T, which indicated that the Sv̄O2 and rScO2 could be interactional.
During anesthesia induction, FIO2 was set to 1.0 to increase the oxygen reserve and to prolong the artificial ventilation suspending time during trachea intubation. A previous study revealed that 1.0 FIO2 during anesthesia induction did not induce obvious atelectasis.28 To avoid atelectasis during the operation, FIO2 was reduced to 0.60 after endotracheal intubation. In addition, because hemoglobin, SaO2, hemodynamics, and oxygen consumption were relatively stable within 10 min during general anesthesia, we can only change FIO2 to change the oxygen delivery, which further influences the values of rScO2 and Sv̄O2. A positive correlation on the variation trend between rScO2 and Sv̄O2 was also found.
There were limitations in the present study. First, the study was limited to 2 different clinical conditions, and we did not perform this study over a range of varying FIO2 concentrations. Second, the hemodynamics was stable in all the subjects during the operation. However, there was no way to conclude whether the obtained correlations would be valid under unstable hemodynamic conditions. Third, these results were based on this condition, namely, that the oxygen supply and consumption function were normal; there would be different results when oxygenation and oxygen transfer capacity are impaired. Also, our study was limited by the relatively small number of subjects; as such, there may be some selection bias.
Conclusions
According to the present study, rScO2 would be adequate in reflecting Sv̄O2 and the variation trend of Sv̄O2 during off-pump coronary artery bypass grafting surgery. Furthermore, the change in FIO2 can simultaneously influence the rScO2 and Sv̄O2 value, and the variation trend of rScO2 and Sv̄O2 was consistent, which has not been reported before.
Footnotes
- Correspondence: Jing-Jie Liu MD, Department of Neurology, The Second Affiliated Hospital of Xi'an Jiaotong University, No. 157 of Xiwu Road, Xincheng District, Shaanxi 710004, China. E-mail: liujingjie0923{at}163.com.
This work was supported by the Department of Cardiac Surgery, the First Affiliated Hospital of Xi'an Jiaotong University, Shaanxi, China.
The authors have disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}