

Abstract
BACKGROUND: High-frequency oscillatory ventilation (HFOV) is used in cases of neonatal and pediatric acute respiratory failure, sometimes even as the primary ventilatory mode. Allowing patients (at least neonates) on HFOV to breathe spontaneously soon after intubation has been shown to be feasible, and this is becoming a more generally used approach for infants and small children. However, such an approach may increase the imposed work of breathing (WOB), raising the question of whether the imposed WOB varies with the use of newer-generation HFOV devices, which operate according to different functional principles.
METHODS: A bench test was designed to compare the pressure-time product (PTP), a surrogate marker of the imposed WOB, produced with the use of 7 HFOV devices. Scenarios corresponding to various age groups (preterm newborn [1 kg], term newborn [3.5 kg], infant [10 kg], and child [25 kg]) and 2 respiratory system conditions (physiologic and pathologic) were tested.
RESULTS: The PTP varied between devices and increased with the oscillation frequency for all devices, independent of the respiratory system condition. Furthermore, the PTP increased with age and was higher for physiologic than for pathologic respiratory system conditions. We considered a change of ≥ 20% as being of clinically relevant; the effect of oscillation frequency was the most important parameter influencing imposed WOB during spontaneous breathing.
CONCLUSIONS: Variations in imposed WOB, as expressed by PTP values, during spontaneous breathing depend mainly on the oscillator frequency, respiratory system condition, and, though to a lesser extent, on the device itself.
- high-frequency oscillatory ventilation
- neonatal intensive care
- work of breathing
- spontaneous breathing
- respiratory insufficiency
Introduction
High-frequency oscillatory ventilation (HFOV) has been used for many years in neonatal and pediatric health care, mainly as a rescue mode of ventilation in cases of severe hypoxic respiratory failure. More recently, especially in the field of neonatal care, HFOV in the very early phase of acute hypoxic respiratory failure has been suggested.1–3 This strategy, while allowing for spontaneous breathing during HFOV, has been shown to render direct weaning to CPAP feasible.4 The maintenance of spontaneous breathing during conventional mechanical ventilation has been shown, at least in adult patients, to enable better ventilation perfusion matching, improve cardiopulmonary function, and shorten ICU length of stay.5–10 However, allowing for spontaneous breathing during HFOV considerably increases the imposed work of breathing (WOB).11 In neonates, who have lower maximal inspiratory flow demands, this increase in imposed WOB is less pronounced.11 Newer-generation HFOV devices use various concepts to build up the mean airway pressure (̄Paw) and to generate oscillation waves.12,13 Therefore, questions arise as to whether the imposed WOB varies with the use of different oscillators and/or settings, and/or in patients with different respiratory system conditions. To investigate these questions, we designed a bench test to compare the imposed WOB that is imposed by HFOV devices while simulating typical breathing patterns of preterm newborns, term newborns, infants, and children with various respiratory system conditions.
QUICK LOOK
Current knowledge
The imposed work of breathing during high-frequency oscillatory ventilation (HFOV) while allowing the patient to breathe spontaneously is greater for pediatric and adult patients than for newborns and infants. Therefore, heavy sedation and even muscle paralysis are often required in older patients, whereas these are usually not needed in newborns and infants, in whom it is furthermore feasible to extubate directly from HFOV.
What this paper contributes to our knowledge
Imposed work of breathing varies mainly with the oscillator frequency and respiratory system condition. Therefore, although it is recommended to use high oscillation frequencies in restrictive lung disease, it might be reasonable to lower these during the weaning phase from HFOV, when lung function has improved and the patient has to take over more spontaneous breathing efforts, since this will allow to reduce imposed work of breathing.
Methods
Ventilators
We used 3 piston HFOV devices: Sensormedics 3100A (CareFusion, San Diego, California); Fabian-HFO, with neonatal and pediatric modes, which uses an electromagnetically driven vibrating diaphragm (Acutronic Medical, Hirzel, Switzerland); and HummingX, which is a linear motor piston pump device (Metran, Saitama, Japan). We used 4 contemporary non-piston devices: Babylog VN500, which uses concepts like flow-modulated sine wave generation (Dräger, Lübeck, Germany); SLE 6000, which is a valveless system (SLE, South Croydon, United Kingdom); Stephanie, a 2-valve oscillation pressure-generation device (Stefan, Gackenbach, Germany); and a Servo-n HFOV prototype, which is a newer concept that relies on the inertia of air in the patient circuit when the pressure at airway opening is modified rapidly, combined with very rapidly responding inspiratory valves and high-flow capability (Maquet, Solna, Sweden). The features of the HFOV devices are described in the supplementary materials (see the supplementary materials at http://www.rcjournal.com). The study was conducted in the pediatric and neonatal ICU in the Department of Pediatrics at the University Hospital of Geneva, in Geneva, Switzerland.
Lung Model
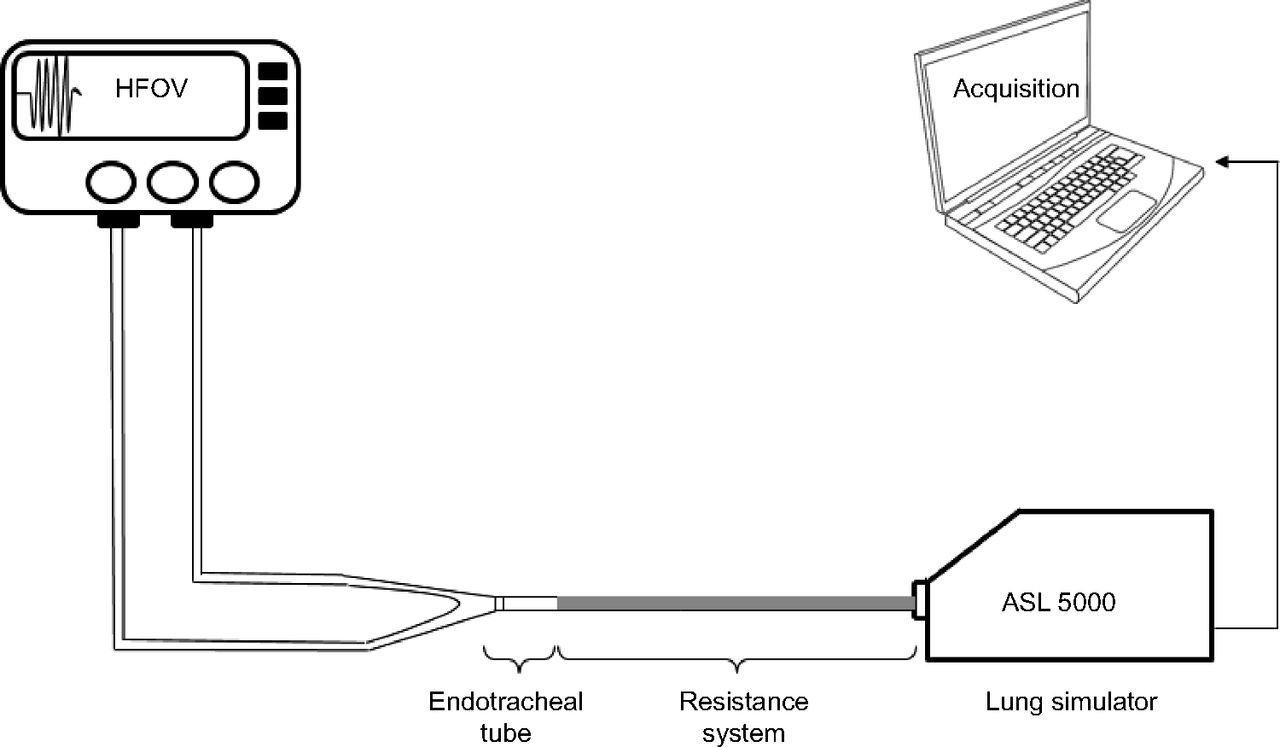
To simulate spontaneous breathing and to test different lung-compliance scenarios, a lung simulator (ASL 5000, IngMar Medical, Pittsburgh, Pennsylvania) was used. In this simulator, flow is generated by a motor-driven piston. System compliance was set directly, and resistance was determined and modified using associations of various resistive tubes. The endotracheal tube and the resistance system were then placed between the lung model and the tested ventilator (Fig. 1). Data were acquired online from the ASL 5000 and stored in a laptop computer for subsequent analysis.
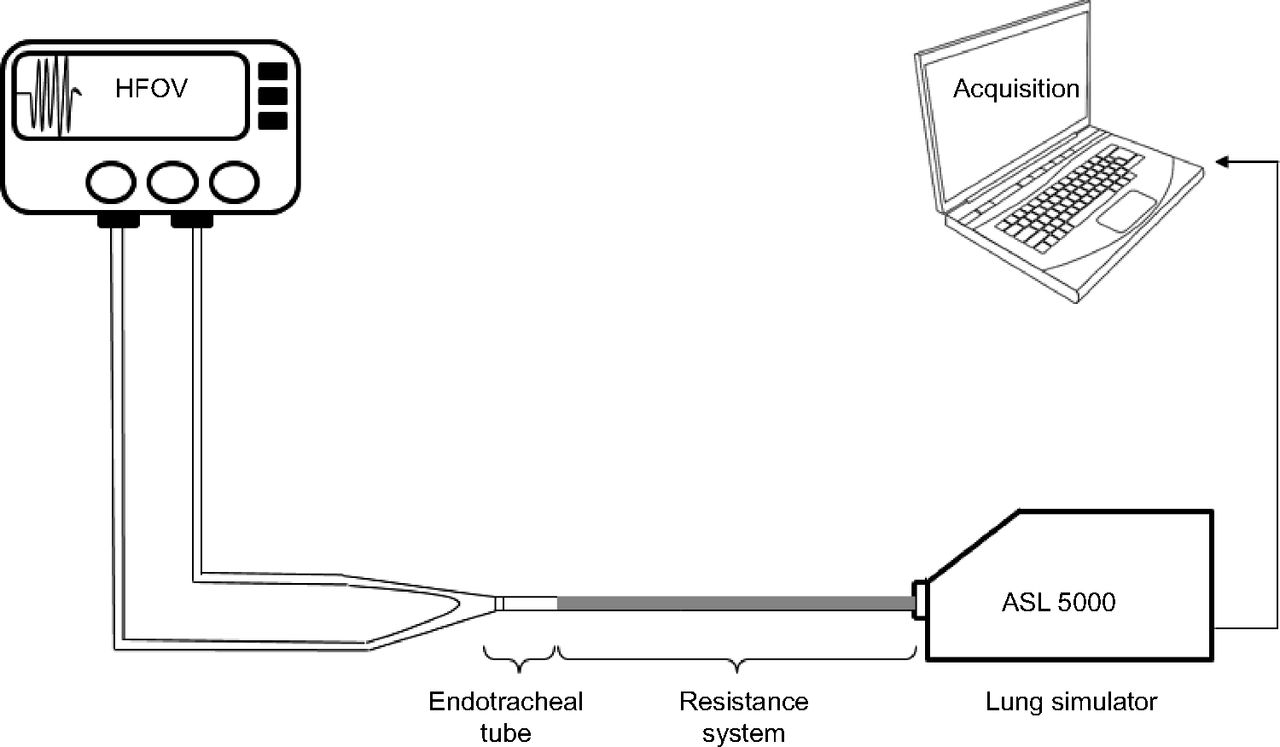
Experimental setup. The endotracheal tube and the resistance system were placed between the mechanical lung model (ASL 5000) and the tested ventilator. Resistance was set using associations of different resistive tubes.
Scenarios
Scenarios corresponding to various age groups (a preterm newborn weighing 1 kg, a term newborn weighing 3.5 kg, an infant weighing 10 kg, and a child weighing 25 kg) and physiologic and pathologic respiratory system conditions were tested. Scenario details are provided in Table 1. The scenarios were developed in accordance with previous publications.14–18 The pathologic conditions were characterized for each age group by poor compliance and normal resistance to simulate restrictive pulmonary disease, corresponding to the most frequent alteration of respiratory mechanics encountered in neonatal and pediatric patients (see the supplementary materials at http://www.rcjournal.com).
Respiratory System Mechanics for Various Scenarios in Pathologic and Physiologic Conditions
Ventilator Settings
HFOV settings were selected according to current clinical practice (Table 2) using:
one continuous distending pressure level set at 12 cm H2O;
2 bias gas flows (10 and 20 L/min), when the device permitted modification of this parameter;
2 oscillation frequencies (10 Hz and 15 Hz for the preterm scenario, 8 Hz and 12 Hz for the term scenario, 5 Hz and 9 Hz for the infant scenario, and 5 Hz and 8 Hz for the child scenario);
an inspiratory-expiratory ratio of 1:1;
an amplitude pressure (ΔP) set to obtain a target tidal volume (VT) of 1.5 mL/kg, measured with an external hot wire anemometer (Florian, Acutronic Medical).19
Because oscillation power varies among oscillators, we chose a clinically relevant VT to enable comparison of similar conditions by targeting HFOV efficiency. To facilitate comparison of ΔP values among devices for the same scenario, ΔP was expressed as a percentage of the maximum amplitude for each oscillator. For this, the scenario was used without spontaneous breathing, and the ΔP was set to the required value up to the maximum permitted by the oscillator.
Settings for the HFOV Devices Tested
Parameters Measured
For each experimental condition, a 1-min period was recorded. The final 3 breaths were then analyzed. The modified Campbell diagram20 is recognized as the accepted standard for imposed WOB measures in patients. Unfortunately, we could not obtain reliable Campbell diagram graphics in our bench setting because the high oscillation frequencies created too many artifacts. We therefore used the pressure-time product (PTP) measure as a surrogate marker of the imposed WOB of the simulated patient breaths, after filtering out the high-frequency oscillation pressure waves with a low-pass filter (set at 2 Hz). The PTP was analyzed as the integral of ̄Paw as a function of time (expressed in cm H2O × s), which corresponds to the area under the curve between the start of the negative deflection of the Paw signal and the return to Paw baseline (Fig. 2).

The PTP was analyzed as the integral of ̄Paw as a function of time (expressed in cm H2O × s), which corresponds to the area under the curve between the start of the negative deflection of the Paw signal and the return to Paw baseline. PTP = pressure-time product; ̄Paw = mean airway pressure.
The second parameter analyzed was the oscillator ΔP, expressed as a percentage of the maximum amplitude for each oscillator corresponding to the power of each ventilator. For this study, we defined an oscillator as sufficiently powerful when the amplitude needed to generate the target VT was < 50% of the maximum ΔP setting, reflecting the capacity to increase the ΔP if disease worsens further.
Statistical Analysis
Data are presented as mean ± SD. We used analysis of variance for multiple comparisons with a post hoc Tukey test for pairwise comparisons between ventilators to examine differences in PTP between ventilators under equivalent test conditions. We used t tests to compare the 2 various bias flow of the Sensormedics 3100A and the Fabian-HFO, the only devices able to modify the bias flow. We considered differences in PTP values of ≥ 20% as potentially clinically relevant. Data were analyzed using Acqknowledge software (version 3.7.3, Biopac Systems, Goleta, California). P values < .05 were considered to be significant.
Results
PTP
PTP values are presented as mean ± SD in Table 3. Statistics for PTP values obtained with the 7 ventilators under 16 conditions are presented in Supplementary Table 2 (see the supplementary materials at http://www.rcjournal.com). PTP values for the premature newborn and term newborn scenarios are illustrated in Figure 3 and 4. Values for the infant and child scenarios are not represented because we chose to illustrate only differences that might be relevant in the clinical setting (ie, ≥ 20%).
Factors Affecting Imposed Work of Breathing During HFOV for Spontaneously Breathing Neonatal and Pediatric Models
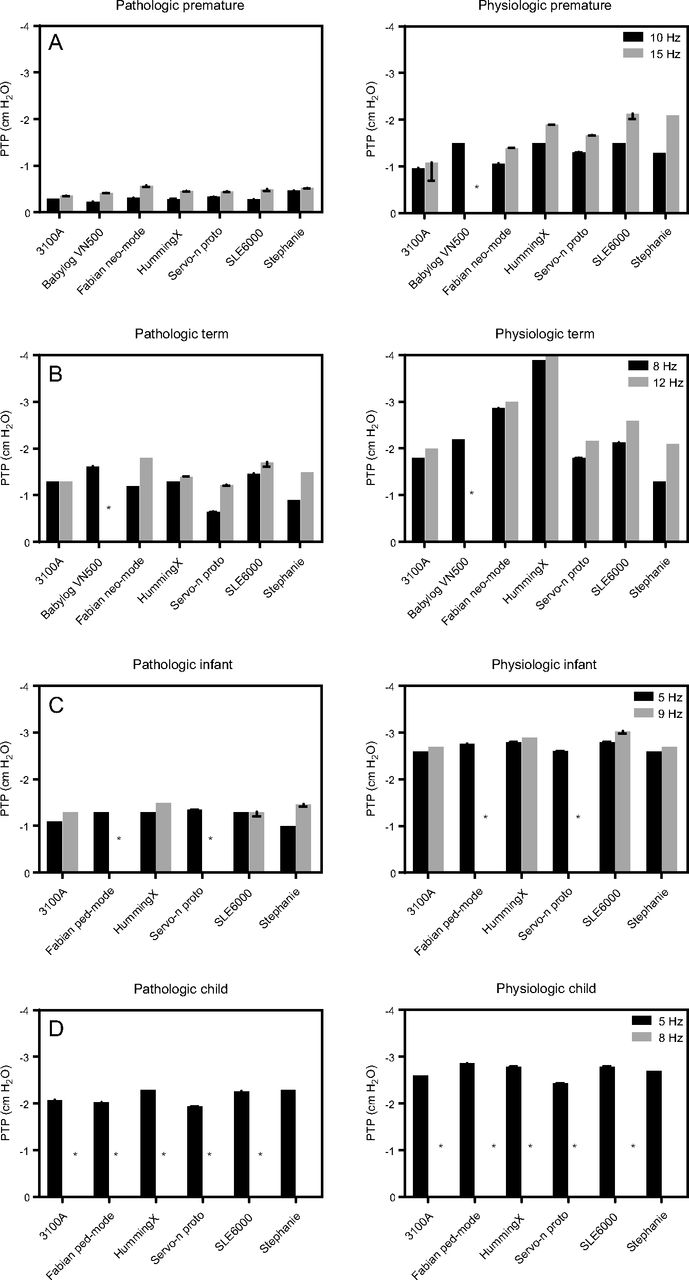
Influence of the frequency, patient type, and respiratory system condition on the PTP. * Conditions under which the oscillator could not deliver the target tidal volume of 1.5 mL/kg. PTP = pressure-time product.
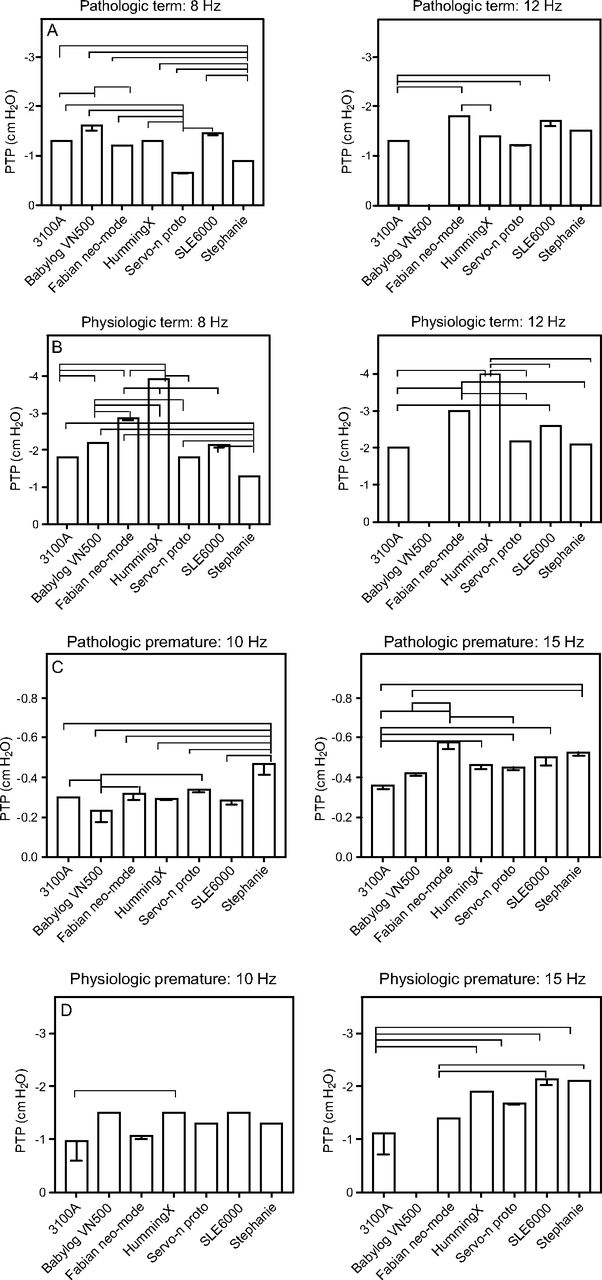
PTP values for premature and term settings. Brackets between devices indicate significant differences (P < .05). Only differences that might be relevant in the clinical setting (≥ 20%) are shown. PTP = pressure-time product.
Influence of Bias Flow.
The 3100A and Fabian devices permitted testing with bias flows of 10 L/min and 20 L/min. No difference in PTP was observed between bias flows, except for the 3100A device in the physiologic term scenario (−2.3 cm H2O × s for 10 L/min, −1.9 cm H2O × s for 20 L/min) (P = .007).
Influence of Frequency.
No oscillator could deliver the VT at 8 Hz for the child scenario. The PTP increased with frequency independent of the respiratory condition and oscillator in all conditions (Table 3, Fig. 3). This increase was less pronounced for the infant conditions.
Influence of Patient Type and Respiratory System Condition.
Under pathologic and physiologic premature and pathologic term conditions, no ventilator was superior to any other in terms of imposed WOB as measured by PTP (Fig. 4). Under the physiologic term condition, the HummingX produced the highest PTP values (−3.88 cm H2O × s at 8 Hz, −4.04 cm H2O × s at 12 Hz), which were approximately double the values obtained with the other oscillators (Table 3, Fig. 3). The infant and child conditions were not tested with the Babylog VN500, which is cleared only for neonatal use. For the other devices, PTP values were similar under the pathologic and physiologic infant and child conditions. In general, measured PTP values were age-dependent, with higher values in older-patient scenarios.
Device Power
For the premature newborn and term newborn scenarios, all but 1 of the tested ventilators were able to deliver the target VT via HFOV; the Babylog VN500 failed to do so under the physiologic premature and pathologic and physiologic term conditions at 15 Hz and 12 Hz, respectively (Supplementary Table 3; see the supplementary materials at http://www.rcjournal.com). For the infant and child scenarios, the tested ventilators were able to deliver the target VT, with 2 exceptions: the Fabian-HFO (even when used in the pediatric mode), and the Servo-n prototype at 9 Hz in the infant scenarios. The 3 most powerful ventilators were the 3100A, the HummingX, and the SLE 6000, independent of the clinical condition tested and the frequency chosen.
Discussion
The main result of this study is that variations in the imposed WOB (as expressed by PTP values) during spontaneous breathing depend on the oscillator frequency, respiratory system condition, and, less importantly, the HFOV device. The second finding is that the power of the tested oscillator, as reflected by the ΔP required to obtain the target VT, varied notably among devices.
Influence of Bias Flow
The shift from 10 L/min to 20 L/min only marginally reduced the PTP obtained with the 3100A. This finding is in part consistent with the results reported by van Heerde et al,11 but that group increased the bias flow from 20 L/min to 60 L/min.
Influence of Frequency
The increase of oscillation frequency raised the PTP specifically for premature and term scenarios. These results can be explained by the rapid back-and-forth flows in the tubing system against which the patient must breathe. This dependence of the imposed WOB on oscillation frequency seems to call for the use of low-oscillation frequencies when allowing for spontaneous breathing. However, the use of higher frequencies with unchanged amplitude settings not only results in lower VT, but also decreases the magnitude of pressure swings and flow spikes transmitted downstream to the proximal and distal lung compartments,21,22 thereby reducing the risk of barotrauma and/or rheotrauma. Pressure-wave damping is known to be least pronounced in the stiff, poorly compliant lung, and most pronounced in the compliant lung.23–25 Despite this knowledge, frequencies as low as 8 Hz in newborns and even lower in adults with poorly compliant lungs are often used to increase ventilation efficiency. In the acute stage of restrictive lung disease, preference is often given to the reduction of frequency because of the fear of using “high” pressure amplitudes, as measured at the airway opening. In contrast, in the weaning phase frequencies are often increased, which will result in the need for higher amplitude levels for a relative short time period. Both concepts seem to be incompletely thought out. The approach of using low frequencies in patients with restrictive respiratory-system conditions may increase the risk of barotrauma and/or rheotrauma, due to poor downstream oscillation pressure-wave damping.26,27 In the more compliant lung (eg, during weaning from HFOV, when more effective spontaneous breathing efforts by the patient can be allowed), oscillation pressure-wave damping becomes much more important because it reduces the risk of barotrauma. Therefore, lower frequencies can be used, and oscillation pressure amplitudes at the airway opening can be further reduced while maintaining the same ventilation efficiency. This approach also reduces the risk of rheotrauma as a result of high peak airway flows. Thus, the reduction of frequency and oscillation amplitude might be suggested when lung conditions (ie, lung compliance) improve. This approach would help reduce the imposed WOB in spontaneously breathing patients during the weaning phase. When introducing the concept of the corner frequency during HFOV, Venegas and Fredberg26 addressed the selection of the optimal protective oscillation frequency according to the mechanical conditions of the lung in much more detail.
Influence of the Respiratory System Condition and Patient Age
The imposed WOB, as measured by PTP, increased with simulated age. This can be explained by the higher inspiratory flows older patients will generate during spontaneous breathing efforts. These results are consistent with those reported in a previous publication11 and with the observation that neonatal patients not only tolerate spontaneous breathing during HFOV more than do older children and adults, without requiring deep sedation or neuromuscular blockade,28 but also can be more easily be weaned directly from HFOV.4
Power
Regardless of simulated condition or oscillation frequency, the 3 most potent ventilators were the 3100A, the HummingX, and the SLE 6000. These findings are in agreement with previous reports29 and should render the user attentive to the fact that not all HFOV devices are equally powerful or can be used over the same range of patient age and/or body weight. Furthermore, all devices showed less power reserve at higher frequencies, which was a major limitation for some devices in some of the clinical scenarios tested.
Conclusions
The main result of this neonatal and pediatric oscillator bench test study was that the PTP, a surrogate marker of the imposed WOB, depended on the oscillator frequency, respiratory system condition, and, though to a much lesser extent, on the HFOV device used. Our observations might have a major impact on the development of recommendations for the selection of optimal oscillation parameters, such as the oscillation frequencies in the acute phase of restrictive lung disease and later, in the weaning phase, when lung function improves and spontaneous breathing efforts are permitted.
Footnotes
- Correspondence: Alice Bordessoule MD, Service of Neonatology and Pediatric Intensice Care, Department of Pediatrics, University Hospital of Geneva Rue Willy-Donzé 6 1211 Geneva, Switzerland. E-mail: alice.bordessoule{at}hcuge.ch.
Dr Bordessoule discloses relationships with SLE, Stefan, and Maquet. The other authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
See the Related Editorial on Page 1191
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}