

Abstract
Background: Readmissions for COPD patients has become an issue for hospitals with the introduction of new Healthcare Law. In October of 2012 the 2010 Affordable Care Act (P.L. 111 148) required the Secretary of the Department of Health and Human Services (HHS) to establish the Hospital Readmissions Reduction Program (HRRP) and reduce payments to Inpatient Prospective Payment System (IPPS) hospitals for excess readmissions (Hospital Readmissions Reduction Program: Fiscal Year (FY) 2018 Fact Sheet). COPD was included in this readmission oversight program effective 2015 and readmissions are calculated based on an averaged one rolling year.
Methods: Houston Methodist Hospital initiated its COPD readmission program in stages. The first stage in 2015 began with data collection on COPD admissions by Respiratory Therapist. Lung Transplants, Lung Cancer, or Congestive Heart Failure exacerbations were excluded by physician review. The second stage was education of patients and family members on the disease process by Respiratory Therapy. In 2016, the third stage began with establishment of a hospital task force comprised of Physicians, Respiratory Therapist, Nurse Practitioners, Case Managers, Social Workers and project coordinators. A standardized care plan based on GOLD (Global Initiative for Chronic Obstructive Lung Disease) standards was established and implemented. In 2017, a weekly case based review of all COPD associated admissions by the task force was initiated; and the Houston Methodist Research Institute developed and implemented a Readmission Predictor app using a neural network drawing from the electronic medical record. Using this prediction tool, resources (including pharmacy, social service, social support groups, outpatient care centers) were engaged and focused on COPD patients most likely to be readmitted .
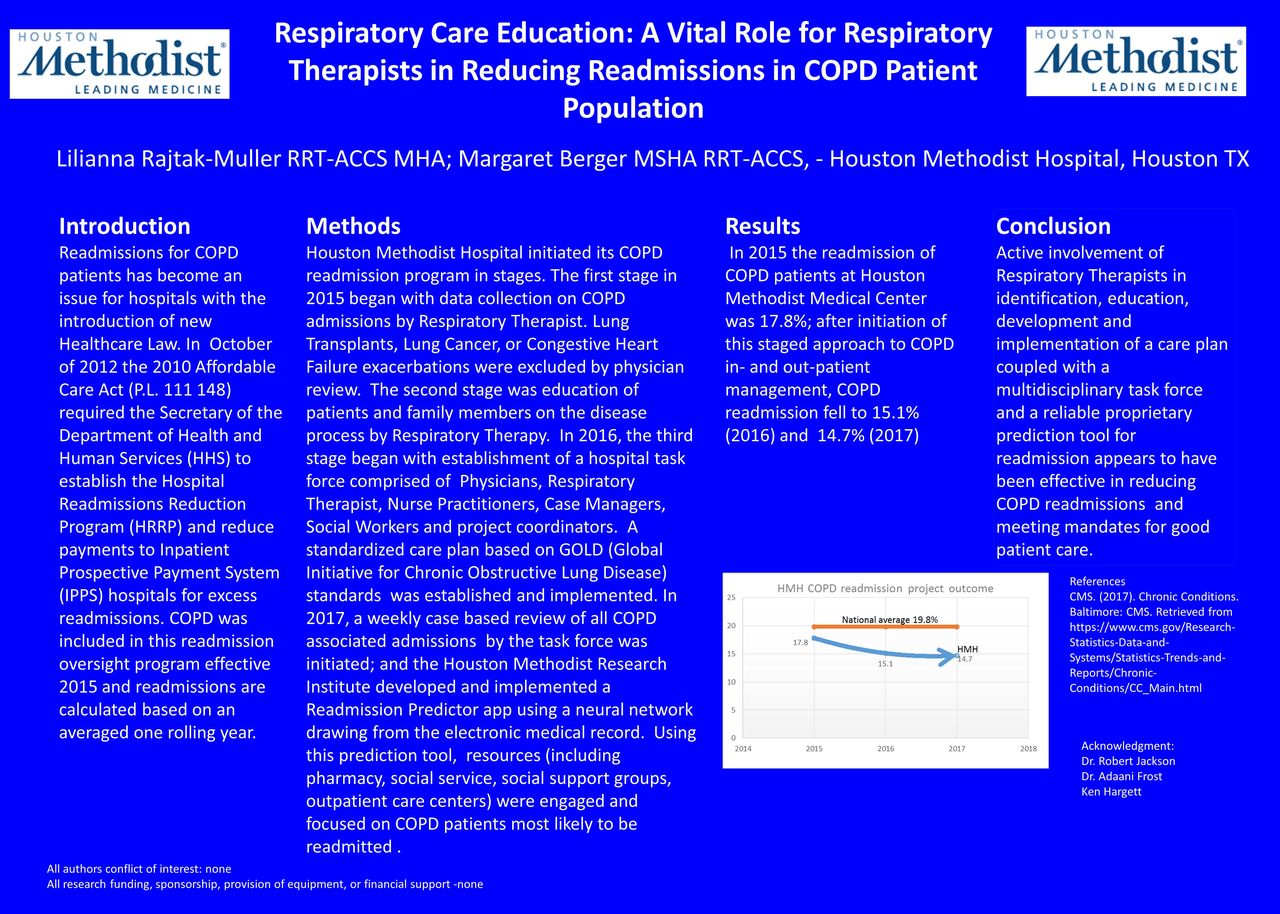
Results: In 2015 the readmission of COPD patients at Houston Methodist Medical Center was 17.8%; after initiation of this staged approach to COPD in- and out-patient management, COPD readmission fell to 15.1% (2016) and 14.7% (2017)
Conclusions: Active involvement of Respiratory Therapists in identification, education, development and implementation of a care plan coupled with a multidisciplinary task force and a reliable proprietary prediction tool for readmission appears to have been effective in reducing COPD readmissions and meeting mandates for good patient care.

Footnotes
Commercial Relationships: None
- Copyright © 2018 by Daedalus Enterprises




{kind=link}