

Abstract
Research in the area of adult invasive mechanical ventilation is rich and diverse. With more than 3,200 articles on mechanical ventilation published in 2018, isolating the most relevant literature is a challenge. Separated into 5 themes (ie, ventilatory support, hyperoxia, ventilator-associated events, prevention of events, and ventilator liberation), this article will describe the most important papers published on adult invasive mechanical ventilation in 2018.
- mechanical ventilation
- ventilatory support
- hyperoxia
- ventilator asynchrony
- ventilator-associated events
- ventilator liberation
Introduction
Patients receiving invasive mechanical ventilation report feelings of pain, loneliness, discomfort, terror, and anxiety.1,2 Mitigation of these adverse events are common challenges for the ICU team. Improving synchrony, optimizing sedation, early mobility, and prevention of complications are all goals in the evidence based management of the ventilated patient.
There are 5 prevalent themes in recently published literature on mechanical ventilation. As they relate to an imagined wish list for mechanical ventilation, the themes are ventilator support and hyperoxia (with the aim to prevent injury), ventilator-associated events and ventilator asynchrony (with the aim to prevent iatrogenic complications), and ventilator liberation (with the aim to liberate the patient from the ventilator as soon as possible). Research in the area of adult invasive mechanical ventilation is rich and diverse. With more than 3,200 articles published in 2018, it is a challenge to isolate the most relevant literature published in the last calendar year. With these themes in mind, this article will review the pertinent literature published on adult invasive mechanical ventilation in 2018.
Ventilatory Support
Patients Without ARDS
The last 2 decades have provided a plethora of data supporting low tidal volume (VT) in patients with ARDS.3–6 Plausible benefits of using low VT in patients without ARDS are fewer complications and decreased ventilator days.7 To investigate the potential effectiveness of low VT versus intermediate VT on ventilator-free days, the Protective Ventilation in Patients Without ARDS (PReVENT) trial was conducted.7
Designed as a randomized control trial, the primary outcome of the PReVENT trial was ventilator-free days at day 28 in subjects without ARDS.7 A low-VT strategy was initiated in 475 subjects and defined as 6 mL/kg of predicted body weight. Comparatively, 480 individuals were assigned to a group with an “intermediate” VT of 10 mL/kg predicted body weight. Both groups had 21 (mean) ventilator free days with no significant differences in ICU length of stay (mean 6 vs 6 d) or hospital length of stay (14 vs 15 d). Other high-value outcomes of 28-d and 90-d mortality showed no significant differences between groups. There were no significant differences in adverse events (eg, development of ARDS, pneumonia, severe atelectasis, or pneumothorax) between groups.7
Recent post hoc observational analysis of previous ARDS trials completed found that decreased driving pressure (ΔP) is associated with increased survival.8 Schmidt et al9 shifted the focus on ΔP toward subjects without ARDS. A retrospective study of 622 subjects was conducted to determine association of ΔP with mortality on the first day of mechanical ventilation. Classification of non-ARDS versus ARDS was tested using the same model as Amato et al.8 Similarly, to confirm the accuracy of their analysis model, Schmidt et al9 validated data in 543 subjects. The study confirmed an association between ΔP and mortality in ARDS. However, an independent association between ΔP and mortality in subjects without ARDS was not established. This was further confirmed by a lack of association with secondary outcomes of hospital, ICU, and 6-month mortality.9
COPD
Due to reportedly higher mortality in subjects with COPD exacerbations, clinicians avoid invasive mechanical ventilation and opt for noninvasive ventilation. A retrospective study by Gadre et al10 included subjects with severe COPD and respiratory failure and sought to describe characteristics and outcomes in subjects with COPD who received invasive mechanical ventilation. Baseline diagnosis of COPD according to the Global Initiative for Obstructive Lung Diseases standard was confirmed using pre-hospital pulmonary function tests. A total of 670 subjects with a pre-morbid diagnosis of COPD were included in the study, 88% of whom were intubated for other etiologies, most commonly pneumonia.
Overall hospital mortality was 25%, with mortality being significantly lower in subjects with COPD exacerbations without additional comorbidities. Subjects with primary COPD exacerbations were more likely to be admitted directly to the ICU from the emergency department. Median duration of mechanical ventilation was 3 d, median ICU length of stay was 5 d, and median hospital length of stay was 12 d. ICU mortality and hospital mortality were lower in subjects with COPD exacerbations. Twenty-six percent of the subjects were readmitted and mechanically ventilated within the 4-y study period. Shorter durations of mechanical ventilation and discharges to home were more prevalent in subjects without comorbidities. Discharges to home were also associated with overall improved survival.10
The application of mechanical ventilation in any disease process is complicated and unique. The fact that patients without ARDS had no significant differences in clinical outcomes raises new questions about what variables may influence duration of mechanical ventilation when using a low-VT strategy. As our understanding of a low-VT strategy continues to evolve, more research will be needed, not only in subjects with or without ARDS, but also in patients with other etiologies. The use of low-VT strategies in COPD, for example, may lead to improved outcomes in a patient population that continues to increase. Similarly, future research may elucidate the role of ΔP in subjects with etiologies other than ARDS.
Hyperoxia
The detrimental effects of oxygen on the lungs has been known for more than a century.11 Harm caused by hyperoxia may not only resemble ARDS, but it may also do more lung damage in patients with ARDS.11,12 Two recent studies have reported hyperoxia to be common in mechanically ventilated subjects.12,13
Aggarwal et al12 extracted data from several ARDSNet studies and reviewed cases with a PaO2 > 80 mm Hg. Hyperoxia, or above-goal oxygen exposure, was defined as a difference between set FIO2 and 0.5 FIO2 when FIO2 was > 0.5 and PaO2 was > 80 mm Hg. Criteria for hyperoxia was met in 2,994 subjects who had a mean excess FIO2 of 0.24. In this population, mortality was higher and subjects had fewer ventilator-free days than those with normoxia. Furthermore, fewer hospital-free days were reported, and the authors concluded that high O2 exposure was associated with worse overall clinical outcomes.12
A second observational study regarding hyperoxia in mechanically ventilated subjects was performed in Japan by Egi et al.13 The aim of the study was not only to observe the relationship of FIO2 and PaO2, but also to observe how FIO2 was managed by clinicians in the setting of hyperoxia. The study included 454 subjects from 28 ICUs who were intubated and mechanically ventilated for > 48 h.
Subjects had FIO2 set at 0.3–0.49 for the majority of their ventilator course. With a median PaO2 equal to 90 mm Hg, 47% of subjects had PaO2 > 100 mm Hg during the study.13
Hyperoxia and the resulting ill-effects are clearly not conjectural in nature. These studies give ICU clinicians guidance on how to better manage oxygenation in critically ill patients. These data may also lead to future changes in clinical practice guides regarding the oxygen management in mechanically ventilated populations.
Ventilator-Associated Events
Effects in or on Prolonged Weaning
In 2013, the Centers for Disease Control and Prevention (CDC) published supportive literature to better define ventilator-associated events (VAEs).14 This has led to an increase in publications related to identification, prevention, and treatment of ventilator-associated conditions (VACs), infectious VACs (IVACs), and ventilator-associated pneumonia (VAP), three mutually exclusive conditions under the category of VAEs.15–18
A single-center, retrospective cohort conducted by Kobayashi et al19 enrolled 404 subjects to determine clinical outcomes in patients with VACs, IVACs, and VAP. Subjects enrolled had been mechanically ventilated for at least 4 d. Subjects were categorized as IVAC, non-IVAC, or non-VAC. Study results reported 54 subjects with VACs and 23 with IVACs. Twenty-one subjects were diagnosed with VAP. These conditions developed a mean 9.2 d from initiation of mechanical ventilation, with a median of 4.5 d. Median days on invasive mechanical ventilation and ICU stay were 7 d and 11 d, respectively. Hospital mortality was independently associated with IVACs, whereas VAP was not associated with hospital death. VACs had a similar association, but it was not statistically significant. The study concluded that VAP does not increase mortality, but VACs and IVACs do increase mortality.
Prevention of Events
Monitoring patient cuff pressures is necessary to prevent aspiration of secretions.20 There is, however, no accepted standard of practice for the frequency of monitoring cuff pressures. Letvin et al21 randomized subjects to frequent monitoring or infrequent monitoring to determine non-inferiority. A total of 166 subjects were randomized to frequent monitoring, defined as after intubation, regardless of location (ICU vs hospital ward); upon admission to the ICU, every 8 h; and when clinically indicated (eg, cuff leaks). Infrequent monitoring (n = 139) was carried out only every 8 h and when clinically indicated. In total, 1,531 cuff pressures were recorded in the frequent group, and 336 cuff pressures were recorded in the infrequent monitoring group. VAEs were monitored for occurrence and frequency. Secondary outcomes included 30-d and 100-d mortality, length of hospital stay, witnessed aspiration events, and VAP rates, and 30-d readmissions.21
The number of VAEs observed was not found to be statistically significant. Similarly, the number of witnessed aspirations and VAP rates were the same in both groups. There was no statistical significance found for 30-d mortality or hospital stay. Only 30-d hospital readmission was found to have a statistically significant difference between groups. As a result of these findings, the authors concluded that more frequent cuff endotracheal tube cuff monitoring was not associated with any outcome benefits.21
When an agency such as the CDC changes recommendations or guidelines, there is a reasonable chance that new research will ensue. Publication of clinical outcomes in patients presenting with VAEs, with or without VAP, will most certainly lead to a better understanding of how to prevent such events. Although not all interventions have outcome benefits, studies of clinical interventions with potential benefits help narrow the focus on what interventions should be changed in the clinical management of invasively ventilated patients.
Ventilator Asynchrony
Sedation
Ventilator-induced lung injury (VILI) can be caused by ventilator asynchrony.22 Using pressure-time, flow-time, and volume-time data, Sottile et al22 developed machine learning algorithms to detect 4 types of ventilator asynchrony. To determine the association between ventilator asynchrony and sedation, 4.26 million breaths were analyzed. Thirty-four percent of the breaths measured were determined to be asynchronous. VT > 10 mL/kg predicted body weight were found in double-triggered and flow-limited breath profiles. In addition, although deep sedation was found to reduce the frequency of asynchronous breaths, only neuromuscular blockade eliminated ventilator asynchrony.22
This prospective cohort study described an exciting area of study in ventilator asynchrony in patients at risk for ARDS.22 The authors added to previously described data that used automated systems to detect asynchrony. However, this is the first time that accuracy, sensitivity, and specificity were tested. Time will tell if artificial intelligence and clinicians' ability to identify unsafe conditions via remote clinical applications could lead to greater patient safety.
Frequency of Asynchrony
Recognizing that double-triggered breaths lead to greater than expected VT, de Haro et al23 analyzed the incidence, mechanism, and physiology of double-triggered breaths. This prospective, observational study continuously monitored 67 subjects and collected a total of 9.69 million breaths. Although double-triggering occurred in just 0.6% of the breaths analyzed, all of the subjects included in the study exhibited double-triggering. Interestingly, double-triggering occurred more frequently in pressure-controlled ventilation than in volume controlled ventilation. This was true regardless of volume controlled breaths with or without decelerating flow. Despite these findings, VT values were higher in volume controlled ventilation with constant flow and with decelerating flow patterns than in pressure controlled breaths.23
The data from these articles emphasize the importance of vigilance when observing patients for double-triggering and ventilator asynchrony. The door has been opened for developing more research regarding artificial intelligence and machine learning. Larger-scale research may lead to further understanding about ventilator asynchrony and clinicians' ability to apply machine learning in an ICU environment. Furthermore, having a deeper understanding of patient interaction with mechanical ventilation may guide research concerning timing of, and patient response to, pharmacologic interventions.22
Ventilator Liberation
Although mechanical ventilation is necessary supportive care, the goal is safe and effective liberation.24 Spontaneous breathing in concert with daily sedation interruption have been shown to decrease the duration of mechanical ventilation.24,25 Length of spontaneous breathing trials (SBT), the use of noninvasive ventilation, and the use of conservative sedation were recently studied.25–27
SBT and Sedation Protocol in ARDS
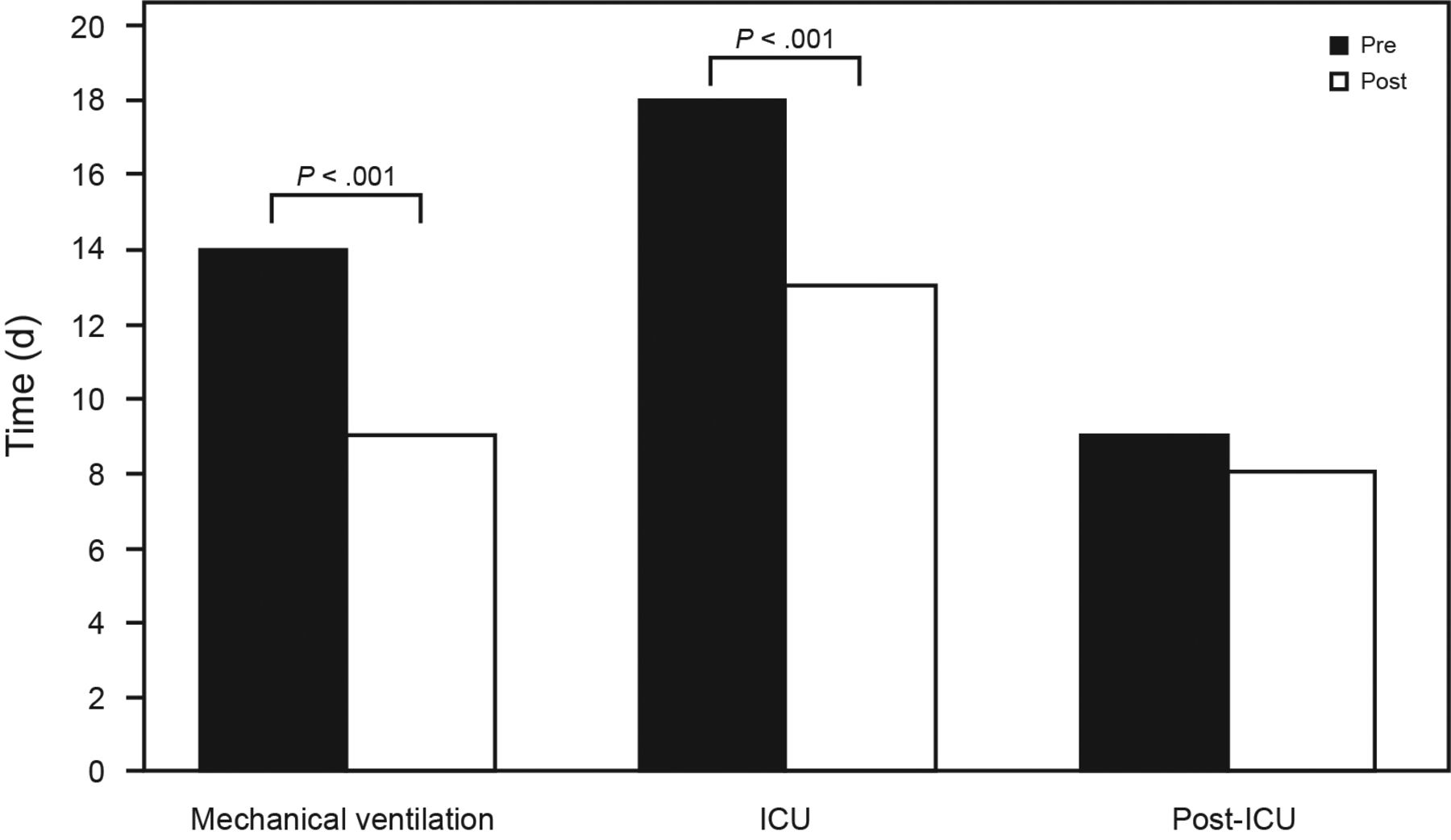
Kallet et al25 investigated the reduction of mechanical ventilation days in ARDS after the implementation of an SBT and sedation protocol. The authors compared 397 pre-protocol subjects and 656 post-protocol subjects. Patients with ARDS who were managed with the protocol saw a significant decrease in the number of ventilator days. Similarly, a statistically significant decrease in ICU days was seen after the protocol's implementation. A median of 2 SBTs were needed for subjects to achieve ventilator liberation. Improved outcomes were also associated with higher pulmonary compliance in patients managed with the SBT and sedation-reduction protocol. These results show that, despite longer duration of mechanical ventilation, subjects with ARDS were not as difficult to liberate from mechanical ventilation as one might assume (Fig. 1).25

Differences in median duration of mechanical ventilation, ICU length of stay, and post-ICU length of stay between the pre-protocol group and the post-protocol group whose weaning and sedation were governed by spontaneous breathing trials and daily sedation interruptions. From Reference 25.
30-min Versus 120-min SBT
Pressure support ventilation used to perform a 30-min SBT may overestimate a patient's ability to spontaneously breathe. Liang et al26 described this in a prospective study of 352 ICU subjects. All of the subjects passed a 30-min SBT prior to moving to a 120-min SBT; 311 subjects successfully passed the 120-min SBT, whereas 41 subjects failed. Physiologic data revealed that subjects in the failure group had a higher heart rate and higher PaCO2during the 30-min SBT than subjects in the success group. Subjects who failed the 120-min SBT also had higher heart rates, breathing frequencies, PaCO2, and rapid shallow breathing index after passing the 30-min SBT. Demographic data revealed that subjects in the failure group were older, had longer durations of mechanical ventilation, and underwent more (unsuccessful) trials before passing the SBT.
For statistically significant findings, the authors applied a point-based system to create decision trees for clinicians to determine whether patients should move from a 30-min SBT to a 120-min SBT. For each of the 4 physiologic parameters that had statistical significance, points were applied to help determine overall success or failure of the SBT. Subjects in the 30-min SBT group with ≤ 2 points failed at a lower rate than subjects with > 4 points. In the 120-min SBT, group the 5 physiological parameters with statistical significance were used for a similar decision-making tree. Like the 30-min study group, subjects with ≤ 2 points had a low failure rate. Subjects in the 120-min group only needed a score of > 2 points to identify failure. These findings reflected a great risk of overall failure in the 120-min SBT group.26
Extubation to Noninvasive Ventilation
Some patients experience difficulty weaning from invasive mechanical ventilation.24 Perkins et al27 randomized subjects to either protocolized weaning and extubations to noninvasive ventilation or standard invasive weaning to determine effectiveness. Time from randomization to ventilator liberation, both invasive and noninvasive, was the primary outcome. Secondary outcomes included duration of invasive mechanical ventilation, re-intubation or tracheostomy, and survival.
Extubations to noninvasive ventilation did not shorten the time of liberation from all types of mechanical ventilation.27 Liberation from all forms of ventilation was 4.3 d in the noninvasive group versus 4.5 d in the invasively weaned group. For subjects extubated to noninvasive ventilation, less time was spent invasively ventilated overall (1 d vs 4 d). The total number of ventilator days was not different between groups (3 d vs 4 d). Re-intubations, tracheostomies, adverse events, and survival were all similar between the study groups.27
Liberation from all forms mechanical ventilation is the ultimate goal of supporting subjects through their disease process. Regardless of etiology, all subjects who meet clinical criteria should have daily interruptions to sedation and SBTs initiated.24 Although some subjects may require longer duration of mechanical ventilation, these concepts can safely and effectively be applied across disease processes. Despite removal from invasive mechanical ventilation being a theme of this review, subjects should also be liberated from noninvasive ventilation in a timely manner.27 Future epidemiologic research may provide further insight into how outcomes and ventilator-free days may be improved.
Summary
Research in the area of adult invasive mechanical ventilation is rich and diverse. The studies summarized here represent a small portion of the publications from 2018. The purpose of this review was to highlight the most relevant publications in the last calendar year. The themes found in these articles help organize relevant publications and summarize the findings.
Footnotes
- Correspondence: Karsten J Roberts MSc RRT, Hospital of the University of Pennsylvania, Department of Respiratory Care Services, 3400 Spruce Street, Ground Floor, Founders Building, Philadelphia, PA 19104. E-mail: karsten.j.roberts{at}gmail.com.
Mr Roberts presented a version of this paper at the Year in Review of the AARC Congress 2018, held December 4-7, 2018, in Las Vegas, Nevada.
The author has disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises





{kind=link}