

Abstract
BACKGROUND: Obstructive lung disease is diagnosed by a decreased ratio of FEV1 to the vital capacity (VC). Although the most commonly used VC is FVC, American Thoracic Society guidelines suggest alternative VCs, for example, slow VC (SVC), may offer a more-accurate evaluation of breathing capacity. There is recent evidence that using only FEV1/FVC underrecognizes obstruction in subjects at high risk and who are symptomatic. Previous studies have indicated that healthy individuals show a minimum difference between FVC and SVC; however, testing of individuals with asthma and who are symptomatic indicates that SVC can be markedly larger than FVC.
OBJECTIVE: To evaluate the differences among SVC, FVC, and SVC-based measurements in the diagnosis of symptomatic obstructive lung disease.
METHODS: A retrospective analysis was performed of spirometry and plethysmography measurements from studies conducted between 2011 to 2015. We established a pulmonary function database that incorporated predictive equations from the National Health and Nutrition Examination Survey III (NHANES III). The SVC to FVC difference was calculated. FEV1/SVC was compared with FEV1/FVC by using NHANES III lower limit of normal values.
RESULTS: A total of 2,710 studies with 2,244 subjects were reviewed. Spirometric obstruction, as defined by NHANES III, was identified in 26.1% of the studies (707/2,710). The mean (± SD) difference between SVC and FVC was 375.0 ± 623.0 mL and 258.8 ± 532.5 mL in those with and those without obstruction, respectively. Subgroup and multivariate analysis demonstrated age, body mass index, and FEV1 associated contributions to the difference between SVC and FVC. By using FEV1/SVC, the prevalence of obstruction increased from 26.1 to 45.0% (1,219/2,710) and identified 566 additional studies of subjects with obstruction. Fifty-four percent of the subjects with newly-identified obstructive lung disease (305/566) had smoking histories, and 67.4% (345/512) received medications for obstructive lung disease.
CONCLUSIONS: The isolated use of FVC-based diagnostic algorithms did not recognize individuals with symptomatic obstructive lung disease. Recognizing the difference between SVC and FVC measurements in subjects will improve testing and diagnosis of obstructive lung disease.
Introduction
Obstructive lung disease is characterized by airway inflammation and bronchospasms that limit expiratory air flow. COPD is a leading cause of mortality around the world, and symptomatic obstructive lung disease is a frequent cause of physician encounters and utilization of health-care resources.1 The American Thoracic Society 1994 guidelines2 standardized the diagnosis of obstruction by using FEV1/FVC. However, the use of FEV1/FVC is noted to have significant limitations. Studies demonstrated that inspiratory vital capacity (VC) and slow VC (SVC) measurements are larger than FVC measurements, with VC measurements having a flow-dependence.3,4 This flow-dependence is suggested to be more pronounced in subjects with COPD, which results in a truncation of expiratory volume in forced maneuvers.5 In acknowledging these limitations, the revised 2005 American Thoracic Society (ATS)/European Respiratory Society (ERS) guidelines6 note that alternative VC measurements may improve the diagnostic accuracy of pulmonary function tests; however, the clinical application of these VC measurements has been limited.
Subjects at high risk for obstructive lung disease can be symptomatic despite having a preserved FEV1/FVC, which questions the accuracy of FEV1/FVC for the diagnosis of obstructive lung disease.7,8 Results of previous studies showed that using FEV1/SVC does increase the prevalence in diagnostic testing for obstructive lung disease; however, systematic evaluation regarding incorporation of alternative VC measurements has not previously been conducted.9–11 It has been hypothesized that SVC can identify subjects with symptomatic obstructive lung disease and a preserved FEV1/FVC. The objective of this study was to determine if plethysmography-based SVC measurements can supplement the spirometry-based diagnosis of obstructive lung disease and to ascertain the utility of applying SVC to clinical practice.
QUICK LOOK
Current knowledge
The current guidelines propose incorporating the largest vital capacity measurement in the diagnosis of obstruction rather than defaulting to FVC; however, the literature has insufficiently described the expected alternative vital capacity values. Exclusive use of FVC-based diagnostic algorithms is known to underrecognize individuals with symptoms.
What this paper contributes to our knowledge
The routine use of SVC to FVC difference or FEV1/SVC improved identification of patients with obstructive lung disease. Recognition of differences between FVC and SVC may allow for earlier detection of disease and improved treatment outcomes.
Methods
This study was submitted and approved by the Brooke Army Medical Center Institutional Review Board (C.2017.004d). A retrospective analysis of pulmonary function test (PFT) studies completed in our pulmonary function laboratory between 2011 and 2015 was conducted. Completed spirometry with plethysmography studies of subjects ages ≥ 18 y, with a weight > 80 lbs (36.3 kg) and height > 45 inches (114.3 cm) were eligible for inclusion. Only pre-bronchodilator values were analyzed to maintain uniformity because bronchodilator testing was not routinely performed in all the subjects. All spirometric- and plethysmography-based measurements were conducted by using either Vmax (CareFusion, Yorba Linda, California) or Medgraphics (MCG Diagnostics, Saint Paul, Minnesota) diagnostic equipment. Testing protocols and calibration were conducted in accordance with the 2005 ATS guideline recommendations.6 Plethysmography testing was conducted after spirometry-based testing by using the same equipment and standard operating procedures.
Demographic information associated with each PFT was entered into established reference equations from the National Health and Nutrition Examination Survey III12 to calculate predicted and lower limit of normal reference values for FEV1, FVC, and FEV1/FVC.12 These predicted values were added to our pulmonary function database. A diagnosis of obstructive lung disease was established based on FEV1/FVC < FEV1 to lower limit of normal FVC ratio. We compared actual versus predicted FEV1 measurements, grading the percent of predicted FEV1 based on American Thoracic Society/European Respiratory Society 2005 guidelines.6 We then characterized FEV1 severity based on previously established markers of mild impairment characterized as an FEV1 of >70% predicted; moderate, ranging from 60 to 69% predicted; moderately severe, categorized as 50–59% predicted; severe as ranging from 35 to 49% predicted FEV1; and very severe as <35%.6 In addition, we placed those individuals with an FEV1 of >90% predicted into a normal FEV1 category.
To quantify the relationship between FVC from spirometry and SVC from plethysmography, we calculated the difference between SVC and FVC values in mL and FEV1/SVC by using the comparison of FEV1/SVC < FEV1 to lower limit of normal FVC ratio to diagnose the presence of obstruction. Clinical evaluation of the specified patient populations was conducted retrospectively through electronic medical record review. Information regarding demographics, smoking history, pulmonary diagnoses to include obstructive and interstitial lung diseases, active pulmonary symptoms, and medication prescriptions for lung diseases were recorded.
Mean ± SD, and standard error were used as summary statistics for continuous variables. Differences in means were analyzed by using the Student t test, analysis of variance, and Wilcoxon test. Multivariate analysis to determine the difference between SVC and FVC was conducted by using variables of sex, presence of obstruction, FEV1 (in L), age, and body mass index (BMI). Significance was established when P values were <.05. The multivariate and statistical analyses were performed by using JMP (SAS Institute, Cary, North Carolina) and SPSS v 22.0 (IBM, Armonk, New York).
Results
Demographics and Pulmonary Function Tests
Of the 6,226 eligible pulmonary function studies available, 3,516 were removed due to incomplete data. The remaining 2,710 studies from 2,244 unique subjects were included in the analysis. The study population was predominantly white (70.6%), male (58.0%) with a mean age of 59.0 y, and a mean BMI of 28.0 kg/m2. The baseline demographic data are shown in Table 1. By using National Health and Nutrition Examination Survey III reference equations,12 spirometric obstruction was identified in 707 of the studies (26.1%). Further spirometric details, based on sex, the presence of obstruction, and FEV1 severity are present in Table 2.
Demographic Chart of the Entire Cohort
Spirometric and Demographic Details of Obstructed and Non-Obstructed Cohorts Based on Sex and FEV1 Severity
Difference Between SVC and FVC
The mean ± SD difference between SVC and FVC was 289.0 ± 560.0 mL. The mean ± SD difference between SVC and FVC for individuals with and those without obstructive spirometry was 375.0 ± 623.0 mL and 258.8 ± 532.5 mL, respectively (Table 1). The difference between SVC and FVC variability across the cohort is presented in Figure 1A. When categorized based on BMI, the subjects with obstruction seemed to have a more uniform difference between SVC and FVC, whereas the subjects without obstruction had an increase in the difference between SVC and FVC with an increasing BMI (Fig. 1B).
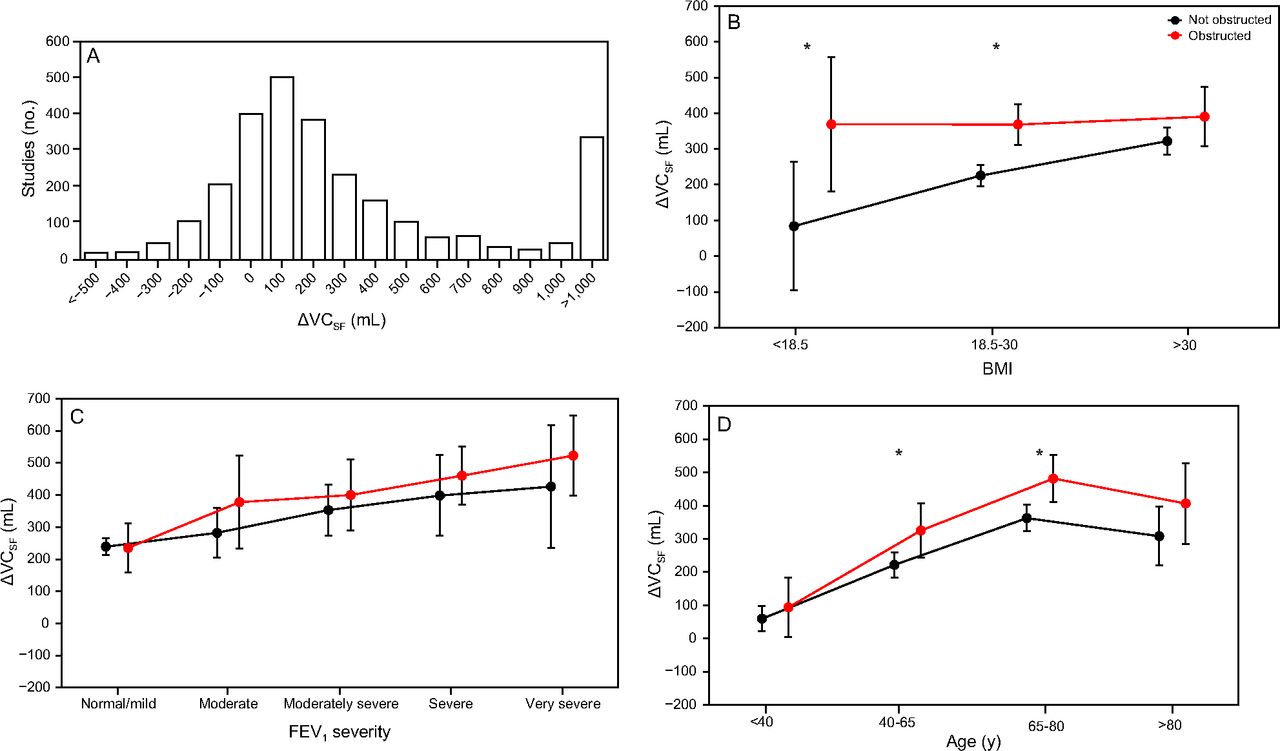
A: Histogram, depicting the difference between slow vital capacity (SVC) and FVC (ΔVCSF) over the entire cohort. Comparison of ΔVCSF to body mass index (BMI) (B), FEV1 severity category (C), and age (D). Values represent mean ± SD. Statistically significant differences regarding delVC (SF) between those with obstruction based on FEV1/FVC and those without obstruction is depicted by (*).
In both subjects with obstruction and subjects without obstruction, there was an increase in the difference between SVC and FVC with worsened FEV1 severity (Fig. 1C). When stratified based on age, the difference between SVC and FVC also increased with age (Fig. 1D), with a mild decrease in the mean difference in subjects ages >80 y. A Student t test was conducted between the cohorts with obstruction and cohorts without obstruction for each subgroup with statistically significant differences present in BMI and some age subcategories, but there were no differences in FEV1 disease severity subgroups. A multi-variate regression analysis was conducted to evaluate predictive markers for the difference between SVC and FVC. Statistically significant variables included sex, age, BMI, and FEV1 (mL), and the presence of obstruction. The associated weighting and predictive equation are listed in Table 3.
Coefficients Derived From Multi-Variate Analysis for Calculation of Predictive Equation for the Difference Between SVC and FVC
FEV1/SVC Based Obstruction
The 2005 ATS/ERS guidelines6 recommend using the largest VC to identify subjects with obstructive lung disease. Use of FEV1/SVC instead of the FEV1/FVC increased in the prevalence of obstruction from 707 of 2,710 studies (26.1%) to 1,219 of 2,710 (45.0%); 54 of 2,710 studies (2.0%) had obstruction based solely on an FEV1/FVC, and 653 (24.1%) studies had obstruction based on both FEV1/SVC and FEV1/FVC. Of the studies, 1,437 of 2,710 (53.0%) did not have obstruction when using either FEV1/SVC or FEV1/FVC, whereas 566 of 2,710 (20.1%) had an FEV1/SVC, suggestive of obstruction with a normal FEV1/FVC. A comparison between FEV1/SVC and FEV1/FVC was conducted by using an inter-rater reliability test with the inter-rater reliability kappa of 0.519. Clinical characteristics of the 566 cases with obstructive lung disease based solely on FEV1/SVC are listed in Table 4. The majority had a smoking history (59.6%), and nearly half carried a previous diagnosis of obstructive lung disease (49.8%). Long-acting β-agonists, inhaled corticosteroids, and/or anticholinergics were prescribed to 345 of the subjects (67.4%).
Clinical Characteristics of Studies With Obstruction Based on FEV1/SVC but Without an FEV1/FVC Suggestive of Obstruction
Discussion
There is recent evidence that those subjects with risk factors for obstructive lung disease and preserved lung function may have more exacerbations and health-care utilization costs than those without predisposing risk factors.8 Current PFT diagnostic algorithms exclude symptomatic, subjects at high risk with other evidence of obstructive disease. This single-center, retrospective PFT evaluation highlighted the large differences that can exist between the plethysmography-based SVC and the spirometry-based FVC maneuvers. We evaluated the difference between SVC and FVC, and the incorporation of an FEV1/SVC-based measurement.
The measurement of VC represents a complex and interdependent relationship among expiratory flow, intrathoracic airway, pleural, alveolar pressures, lung elastic recoil, and airway resistance.13 FVC/SVC has been proposed to detect small airway disease. This difference has been considered a potential marker of air-trapping and hyperinflation.14 Previous guidelines suggest an expected difference of 90–200 mL between FVC and SVC maneuvers in a selected reference population.4 Results of a few studies showed that larger VC differences in both subjects with asthma and subjects with COPD are associated with worse respiratory symptoms and decreased exercise tolerance5,15,16
The mechanism for the difference in VC volumes is unclear. Brusasco et al5 indicate that increased air-flow results in increased transmural pressures in peripheral airways and subsequent airway closure at higher volumes. O'Donnell et al17 theorized that increased airway compliance results in pulmonary relaxation and static lung hyperinflation. Quanjer et al4 found that heterogeneous gas compression resulted in the observed differences between FVC and SVC. Although the pathophysiology responsible for the difference remains under study, the recognition of the difference is important for accurate interpretation of PFTs.
Analysis of our data demonstrated a relationship between the difference between SVC and FVC and multiple variables. In all subgroup analyses, subjects with an FEV1/FVC-based obstruction had a larger difference than those without obstruction; however, there was a sizable difference between SVC and FVC present, even in those individuals without obstruction. When compared with BMI, there seemed to be a linearly increasing the difference between SVC and FVC in the subjects without obstruction, compared with the constant difference between SVC and FVC present in subjects with obstruction. Both obstructed and non-obstructed subjects demonstrated an increasing difference between SVC and FVC with age and FEV1. When combined in a multi-variate analysis, these variables, along with sex, indicate that the difference between SVC and FVC is influenced by variables other than solely BMI.18
Hyatt et al9 noted an increase in the diagnosis of obstructive lung disease by ∼50%, similar to several other studies across diverse ethnic groups.10,11 This study confirmed this observation, with an increased prevalence of obstructive lung disease from 26% with the use of FVC to 45% when applying FEV1/SVC criteria. Our study captured an additional 566 subjects who would be classified as having obstructive lung disease based on this measurement. The majority of these subjects were smokers treated with bronchodilators or had a diagnosis of obstructive lung disease but maintained a preserved FEV1/FVC.
The physiologic correlation of the SVC measurements in diagnosing obstruction remains unknown. It could be hypothesized that the difference between SVC and FVC represents a type of air-trapping present, with only mild exertion, which potentially helps to explain the discrepancy regarding symptoms among subjects. However, critics of SVC-based algorithms have questioned the utility of a submaximum effort because this volume is not used in normal breathing and cited the bias associated with BMI.9,18 Alternative diagnostic criteria, such as FEV1/Forced expiratory volume in six second and Forced expiratory volume in three seconds/FVC, have previously been suggested but likely rely on similar flow dynamics and elastic properties as FEV1/FVC measurements.19,20 Although the uncertainty regarding SVC to FVC difference remains present, recognition that these differences exist may improve diagnostic utility of PFTs.
Study limitations included demographics of <1% Asians and a potential overestimation of our Hispanic population because previous demographics misidentified the Asian race as Hispanic. However, the exact amount of overestimation cannot be determined. In addition, our cohort represented only referred subjects, most commonly with symptoms, which may have biased our VC difference measurements. Other limitations included the use of plethysmography to measure SVC rather than spirometric-based measurements, a failure to normalize SVC to FVC difference for common demographic markers (eg, age, height, and sex) and the lack of robust SVC-based reference equations.
Conventional teaching suggests that SVC is larger than FVC, albeit with small differences, whereas analysis of our data demonstrated select cases with FVC that were larger than SVC was present in subjects in select cases. These results were similar to those previously noted by Fortis et al,18 who postulated that the negative difference between SVC and FVC was secondary to the inspiratory reserve volume difference associated with BMI. Although a specific alternative mechanism for negative difference between SVC and FVC may be based on altered flow dynamics in those with a more depressed FEV1, which resulted in more-proximal obstruction during maneuvers of increased intrathoracic pressure. Comparatively, in individuals without obstruction or with mild FEV1 impairment, the increased intrathoracic pressure may serve to expel air from more distal alveoli with greater force, while also stenting open airways to allow for larger flow volumes during forced maneuvers. Alternatively, the negative difference between SVC and FVC may represent a testing error from using 2 separate methods of measuring VC: spirometry and plethysmography.18
Conclusions
The routine use of SVC to FVC difference or FEV1/SVC may offer improved identification of subjects with obstructive lung disease. The current use of only FVC-based diagnostic algorithms underdiagnose individuals with milder disease and individuals in whom increased intrathoracic pressure truncates the FVC measurement. Although the clinical implementation of SVC-based diagnostic criteria requires additional studies, recognition of differences between FVC and SVC may allow for earlier detection of disease and improved treatment outcomes.
Footnotes
- Correspondence: Nikhil A Huprikar, Pulmonary/Critical Care Service (MCHE-ZDM-P), Brooke Army Medical Center, 3551 Roger Brooke Drive, JBSA Fort Sam Houston, TX 78234. E-mail: nikhil.a.huprikar.mil{at}mail.mil.
Dr Morris discloses relationships with Vyaire and Janssen Pharmaceuticals. The remaining authors have disclosed no conflicts of interest.
The view(s) expressed herein are those of the authors and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army and Department of Defense or the U.S. government.
- Copyright © 2019 by Daedalus Enterprises





{kind=link}