

Abstract
BACKGROUND: Recent literature suggests that optimization of tidal driving pressure (ΔP) would be a better variable to target for lung protection at the bedside than tidal volume (VT) or plateau pressure (Pplat), the traditional indicators of ventilator-induced lung injury. However, the usual range or variability of ΔP over time for any subject category have not been defined. This study sought to document the ΔP ranges observed in current practice among mechanically ventilated subjects receiving routine care for diverse acute conditions in a community hospital environment.
METHODS: This was a retrospective, observational study in a university-affiliated and house staff–aided institution with respiratory care protocols based on extant lung-protective guidelines for VT. Demographic characteristics and measured parameters related to mechanical ventilation and hemodynamics were extracted from electronic records of intubated subjects for each 8-h period of the first 24 h in the ICU. Pplat values reported by the ventilator were validated by the respiratory therapist before those data were entered into the electronic medical record.
RESULTS: The mean ΔP was significantly higher at Time 1 (mean 16.1, range 7.0–31.0 cm H2O) compared to both Time 2 (mean 14.5, range 7.0–35.0 cm H2O) (P < .001) and Time 3 (mean 14.8, range 8.0–32 cm H2O) (P < .001). At all time points, the median ΔP was higher for completely passive breathing compared to triggered breathing. The widest difference between presumed entirely passive and presumed intermittently or consistently triggered breaths occurred at Time 1 (mean ΔP = 17.2 vs 14.9 cm H2O, respectively) (P = .01).
CONCLUSIONS: Suggested safety thresholds for ΔP are often violated by a strategy that focuses on only VT and Pplat. Our data suggest that ΔP is lower for passive versus triggered breathing cycles. Vigilance is especially important in the initial stages of mechanical ventilator support, and attention should be paid to triggering efforts when interpreting and comparing machine-determined numerical values for ΔP.
- ventilators, mechanical
- ventilator-induced lung injury
- lung injury
- driving pressure
- respiratory failure
- ventilator settings
Introduction
Lung-protective mechanical ventilation strategies aim to reduce the incidence of ventilator-induced lung injury. These strategies typically center on delivering relatively low tidal volumes (VT) of 5–8 mL/kg of predicted body weight (PBW) and restricting plateau pressure (Pplat) to 30 cm H2O.1–4 In an influential analysis of data from randomized trials of subjects with ARDS, Amato and colleagues reported that driving pressure (ΔP), the difference between Pplat and end-expiratory airway pressures assessed under passive conditions, was strongly linked to mortality risk.5 The implicit inference of this association is that ΔP could play a key causal role in ventilator-induced lung injury. Prompted by these persuasive data, recent literature suggests that optimization of ΔP would be a better variable to target for lung protection at the bedside than those in prior use (VT and Pplat). Although a ΔP of approximately 15 cm H2O has been commonly interpreted as the upper limit of safe ΔP for ARDS, the safety threshold is likely to vary among patients, and no specific numerical value has been prospectively tested for predictive accuracy.
Such questions need to be addressed for diverse patient populations. Failure to adhere to lung-protective ventilation strategies may lead to the development of ARDS6 as well as encourage adverse postoperative outcomes in patients without overt lung disease.7,8 Comprehensive surveys have reported that accepted standards for lung-protective practices in mechanical ventilation are not followed consistently.9–11
ΔP, which is the difference between end-inspiratory plateau and PEEP, is numerically equivalent to VT divided by the respiratory system compliance (CRS), a parameter usually determined primarily by the number of functional alveoli. Therefore, it can reasonably be argued that ΔP correlates better with functional (“baby”) lung size than does VT referenced to PBW. Because ΔP may be influenced not only by lung conditions but also by chest wall compliance, its absolute value may reflect body habitus, alterations in position, and muscular tone as well as tidal lung excursions and stretching forces imposed upon the alveoli.
Although ΔP is theoretically appealing as a convenient guide for targeting safe ventilation, we currently do not know its usual range in patients receiving putatively safe VT and Pplat, its variability in the same patient over time, or whether patients are currently being ventilated above or below proposed thresholds of safety for ΔP. Therefore, we sought to document over time the ΔP ranges observed in current practice among mechanically ventilated subjects receiving routine care for diverse acute conditions in a community hospital environment.
QUICK LOOK
Current knowledge
Driving pressure (ΔP), the difference between plateau pressure (Pplat) and end-expiratory airway pressure, has been reported to be strongly linked to mortality risk. Although its causative role has not yet been confirmed, a ΔP of approximately 15 cm H2O has been suggested as the upper limit of safe ΔP for ARDS.
What this paper contributes to our knowledge
In a university-affiliated and house staff–aided institution with respiratory care protocols based on lung protective guidelines for (VT) and Pplat, our data illustrate the mean amplitude and wide range of ΔP among hospitalized subjects with diverse acute conditions. Targeting (VT) and Pplat alone may not align with current thinking regarding limitation of dynamic strain and injurious forces driving inflation. The suggested safety threshold for ΔP is often violated by a strategy that focuses on only tidal volume and Pplat. Vigilance is especially important in the initial stages of mechanical ventilator support, and attention should be paid to triggering efforts when interpreting and comparing numerical values for ΔP.
Methods
Study Design and Population
In this retrospective, observational study, we reviewed the electronic medical records of 125 subjects who were mechanically ventilated for at least 24 h in the Medical and Surgical Intensive Care Units at Regions Hospital (St. Paul, MN) over a 12-month period spanning August 2013 to August 2014. The study was approved by the HealthPartners Institutional Review Board, which oversees research conducted at this site.
Data Collection
Data collection included age, gender, race, weight, height, body mass index, mode of mechanical ventilation, set breathing frequency, set VT, set PEEP, set FIO2, total breathing frequency, static CRS, Pplat, auto-PEEP, peak inspiratory pressures, exhaled minute ventilation, diagnosis for hospitalization, indication for initiation of mechanical ventilation, duration of mechanical ventilation, and medications used for sedation.
Our electronic medical record system (Epic, Madison WI) retains only caregiver-validated data. Therefore, all stored mechanical ventilator data had been collected, validated, and entered into the electronic medical record by trained respiratory therapists during routine care. At the time of data collection, the mechanical ventilator used was the Puritan Benett 840 Ventilator. Routine mechanical ventilator checks and measurements were performed every 4 h, according to hospital protocol (see the supplementary materials at http://www.rcjournal.com). The recorded single-point measurements of parameters for mechanical ventilation (ie, set and observed breathing frequencies, PEEP, FIO2, static CRS, Pplat, auto-PEEP, peak inspiratory pressures, and exhaled minute ventilation) were extracted from the electronic medical record for each subject approximately every 8 h for a total of 3 assessment time points over the 24 h immediately following intubation. ΔP values were calculated as ΔP = (Pplat − PEEPtotal), while CRS values were calculated as CRS = VT/(Pplat − PEEPtotal). All subjects were positioned with the head of the bed elevated to at least 30°. The algorithm of these ventilators for determining and displaying Pplat requires the absence of overt effort or instability during end-inspiratory circuit occlusion, but it does not assure entirely passive inflation (see the supplementary materials at http://www.rcjournal.com). To determine whether the subject was likely to be triggering the ventilator at the validated time point, the set breathing frequency was subtracted from the subject's observed breathing frequency. The subject was designated as triggering the ventilator (at least intermittently) if the difference between the between the subject's measured breathing frequency and set rate exceeded zero.
Statistical Analysis
Descriptive statistics were used to evaluate the demographic characteristics of the participants. The mean and standard deviation were used to summarize continuous measures, and the number and frequency were used to summarize categorical variables. Analysis of variance testing for repeated measures was used to compare the differences in mechanical ventilator parameters at 3 time points. In addition, adjustment for multiple comparisons by the Tukey test was used for pairwise comparisons at each time point. A 2-tailed, 2-sample t test was used to evaluate the differences in mean ΔP between passive versus active breaths and differences of data for female versus male subjects at each time point. Linear regression analysis was used to evaluate whether sex is associated with the variability in ΔP, adjusting for body mass index (continuous variable) and presence of chest wall restriction. Statistical significance was assigned to P ≤ .05.
Results
The baseline characteristics of the subjects are presented in Table 1. There was a statistically significant reduction of mean ΔP from Time 1 versus Time 2 (P < .001) and from Time 1 versus Time 3 (P < .001), but no significant difference between Time 2 and Time 3 (P = .16) (Figure 1). The proportions of all subjects exceeding ΔP of 15.0 cm H2O were 60%, 38%, and 47% at Time 1, Time 2, and Time 3, respectively. At Time 1, which was closest to initiation of mechanical ventilation, the group mean ΔP was 16.1 cm H2O (range 7.0–31.0 cm H2O). At Time 2, which was approximately 8 h after initiation of mechanical ventilation, the mean ΔP decreased to 14.5 cm H2O (range 7.0–35.0 cm H2O). At Time 3, which was approximately 16 h after initiation of mechanical ventilation, the mean ΔP was 14.8 cm H2O (range 8.0–32.0 cm H2O) (Table 2). The distribution of ΔP among mechanically ventilated subjects at Time 1, Time 2, and Time 3 are shown in Figure 1.
Baseline Characteristics
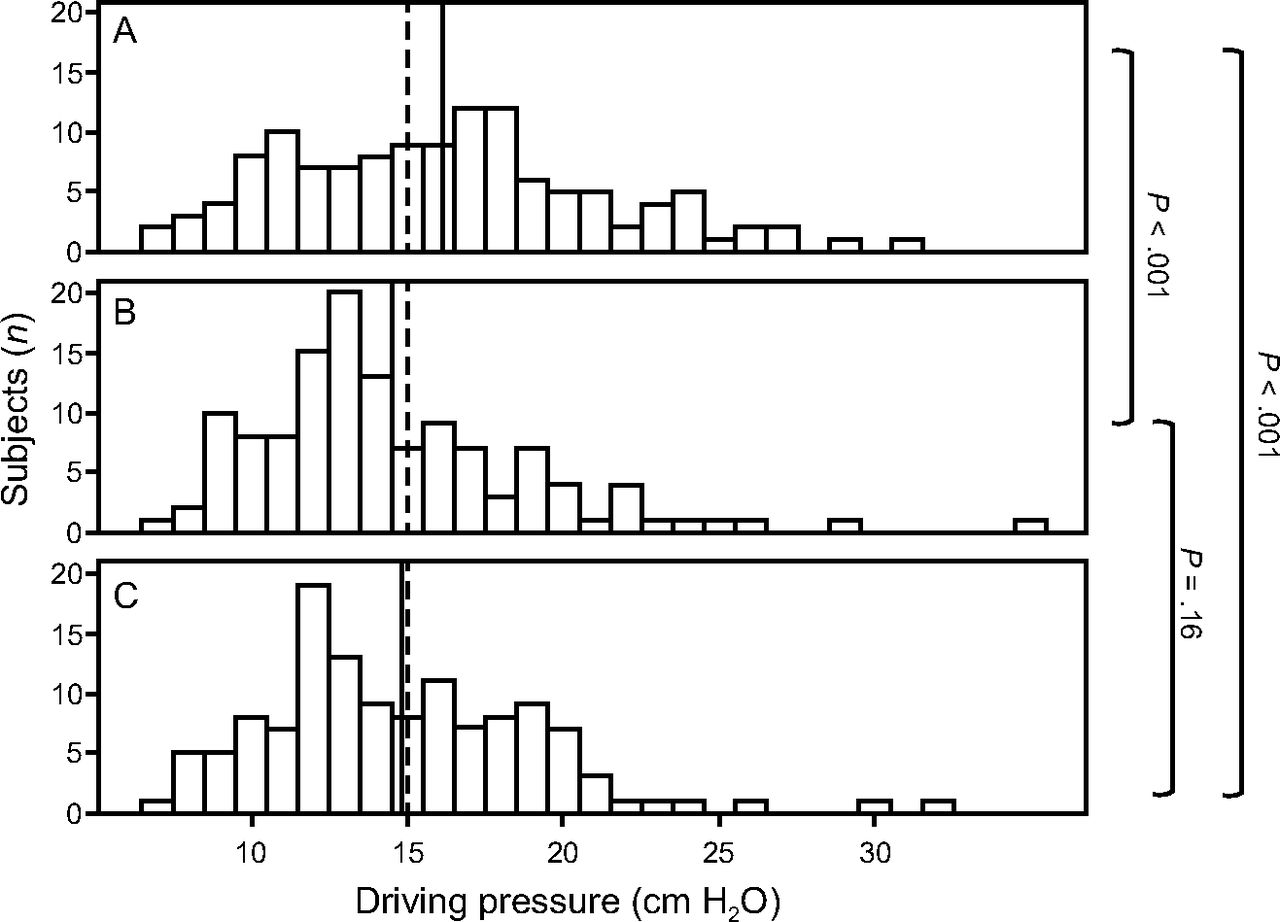
Distribution of driving pressure among mechanically ventilated subjects at 3 different time points (A: Time 1, B: Time 2, and C: Time 3). The dashed line marks ΔP of 15.0 cm H2O, and the solid black line marks the mean driving pressure at each time point.
ΔP and CRS at Time 1, Time 2, and Time 3
At all time points, the median ΔP was higher for passive breaths compared to breaths delivered to subjects who were likely to be triggering (at least intermittently) at the time of data entry while mechanically ventilated in the volume assist-control mode (Fig. 2). The mean (SD) ΔP values at Time 1 were 17.2 (4.0) versus 14.9 (4.1) cm H2O (P = .01) for passive versus triggered breathing, respectively. The mean ΔP values were 15.2 (4.1) versus 13.7 (4.1) cm H2O (P = .060) at Time 2 and 15.5 (4.1) versus 14.2 (4.0) cm H2O (P = .07) at Time 3 for passive versus triggered breathing, respectively.
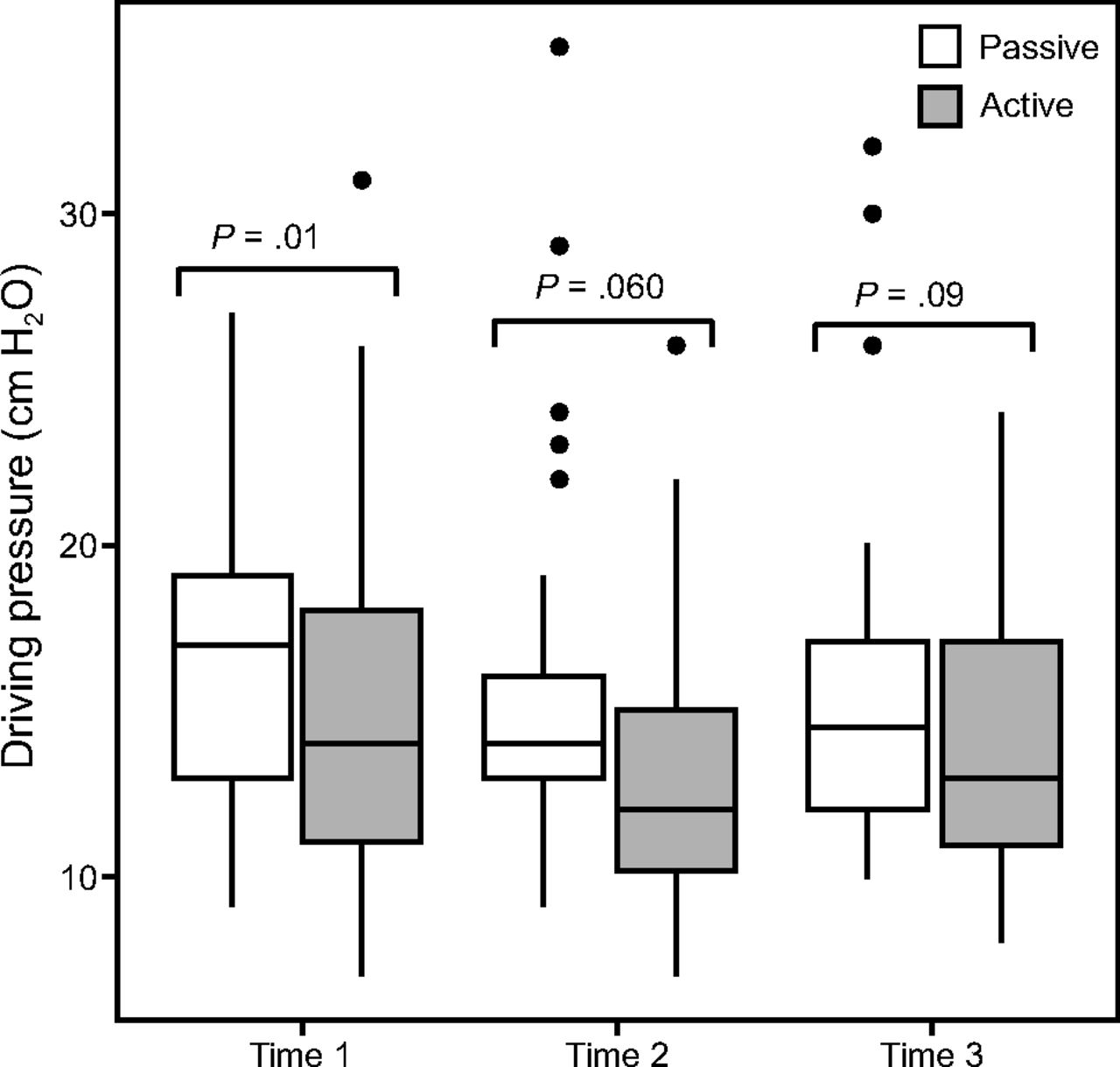
Driving pressure at 3 time points comparing mechanically ventilated subjects on volume assist-control mode during passive versus active breathing. Horizontal lines represent the median driving pressure.
At all time points, the mean ΔP values of females were higher than those of males (Fig. 3). The mean ΔP of females were 17.1, 15.4, and 15.8 cm H2O, while the mean ΔP of males were 15.1, 13.5, and 13.9 cm H2O at Time 1, Time 2, and Time 3, respectively (Table 3).
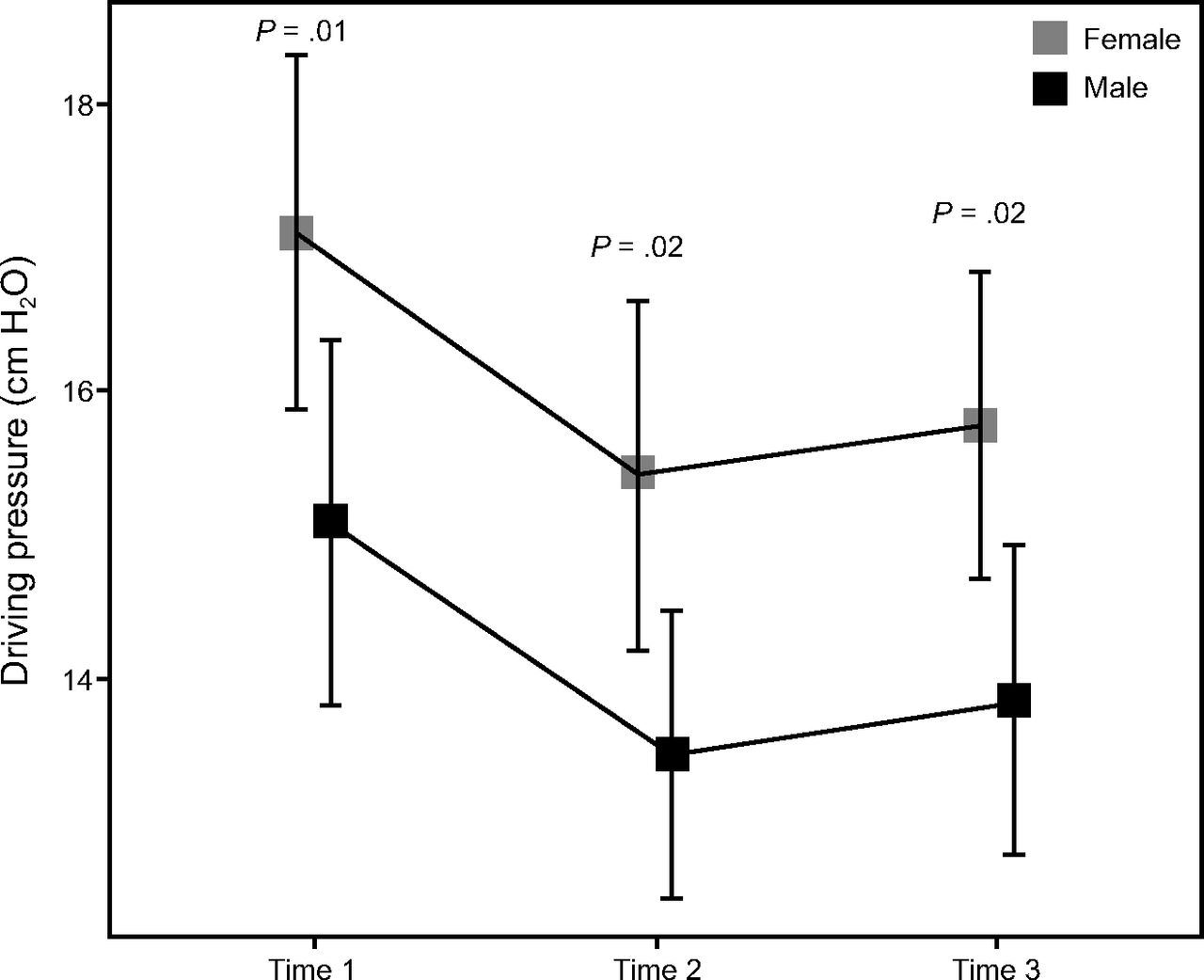
Mean driving pressure for females versus males at Time 1, Time 2, and Time 3. Vertical lines show confidence intervals.
Mechanical Ventilator Parameters Comparing Females vs Males
The values for set PEEP and Pplat (Time 2 and Time 3) were similar for female and male subjects (Table 3). However, males had higher minute ventilation and compliance values compared to females. The ΔP and the VT/PBW of males compared to females were also lower.
After controlling for body mass index, possible associated chest wall restriction, and VT/PBW, the adjusted odds ratio (adjusted OR) for every 1-cm H2O increase in ΔP is higher for females compared to males (adjusted OR 1.97, 95% CI 1.05 to 3.73, P =.036) (Table 4).
Odds Ratios Comparing Females vs Males
The mean CRS was lowest at Time 1 (Table 2). The mean (SD) CRS values were 33.4 (16.4), 39.7 (16.0), and 40.1 (16.3) mL/cm H2O at Time 1, Time 2, and Time 3, respectively.
Although there appears to be an increasing trend in ΔP with increasing body mass index, as illustrated in the scatter plots of ΔP versus body mass index, there was a very limited number of subjects with body mass index >40 kg/m2 in our subject sample, which precludes this determination (Fig. 4).

Scatter plots of driving pressure versus body mass index at A: Time 1, B: Time 2, and C: Time 3. BMI = body mass index.
Discussion
In a university-affiliated and house staff–aided institution using respiratory care protocols based on lung-protective guidelines for VT and Pplat (see the supplementary materials at http://www.rcjournal.com), our data illustrate the mean amplitude and wide range of ΔP among hospitalized, ventilated subjects with diverse acute conditions. These data emphasize that targeting VT and Pplat alone may not align with current thinking regarding dynamic strain and injurious driving forces.12
A safe value for ΔP is currently undefined and will vary across patients according to variables such as chest wall characteristics and position. Although this has yet to be determined prospectively, the suggested safe upper threshold value for ΔP (ie, <15.0 cm H2O) has already been incorporated into many care protocols worldwide. This was not, however, implemented at our own institution at the time of data collection. Our data, which preceded the publication of reports urging closer attention to ΔP,5 suggest that while safe VT and Pplat were recognized and well-respected goals of our ventilator management, ΔP often exceeded the currently suggested <15 cm H2O guideline. We found that the recorded ΔP among these subjects ranged from 7.0 to 35.0 cm H2O, with up to 60% ventilated with ΔP ≥ 15.0 cm H2O at the time of initiating mechanical ventilator support (Time 1). With VT unvarying, ΔP changed during the first 24 h, with the mean ΔP statistically highest within the first 8 h of initiating mechanical ventilation. Improved CRS, likely relating to gradual lung recruitment, treatment of the underlying acute illnesses, and adjustment in level of sedation, may account for the reduction in ΔP in later time periods. Our sample included too few subjects with body mass index >40 kg/m2 to attempt a valid correlation of ΔP to massive obesity. In addition, morbid obesity and other conditions that alter chest wall compliance can contribute to pleural pressure, and can therefore cause “elevated” Pplat measurements. Thus, careful interpretation of these measurements is warranted.
Although valid ΔP measurements can only be obtained when the subject achieves a stable end-inspiratory plateau and does not breathe actively during circuit closure (the machine algorithm precludes the latter), we noted that some subjects triggered the ventilator around the approximate times when the ΔP measurements were recorded. Subjects on volume-control mode who were presumed to be at least intermittently triggering assisted breaths had somewhat lower ΔP values compared to subjects who were not making respiratory efforts. Current generation ventilators will display a Pplat if the subject is gently triggering the assisted breath. Perhaps it is worth noting that virtually none of the randomized clinical trials in the literature addressing ventilator settings, including the most influential in current practice, rigidly assured passive breathing before data recording.
In our study, females had higher ΔP than males with similar set values for PEEP, but the ΔP was not statistically different (adjusted odds ratio 1.86, 95% CI .99 to 3.52, P = .054) between females and males after adjusting for body mass index and presence of chest wall restriction (Table 4). Although the observed compliance values of female subjects were >10 mL/cm H2O lower than those of male subjects, there is little reason to believe that specific compliance of the lung and principles of ΔP containment and ventilator-induced lung injury avoidance are gender-specific. Females are known to have smaller lung volumes by 10–12% compared to males, and therefore lower chest compliance, based on previously published work.13
Our population sample included only small numbers of subjects with ARDS. Force amplifiers place the lung tissues of such patients at increased injury risk and might lower the real threshold for safe ΔP. On the other hand, it appears from available evidence that subjects without ARDS also may be harmed by ΔP values that are not closely regulated to be lung-protective.14
Our study has a number of noteworthy limitations. First, this is a retrospective survey with a relatively small sample size. Second, the ΔP values are based on airway rather than transpulmonary pressure measurements, which conceptually are more precisely relevant to lung protection. Third, our data set was limited to the first 24 h after initiating mechanical ventilator support. Fourth, on average, our subjects were ventilated with VT approaching the upper boundary of lung-safe VT. Fifth, although we collected data on sedation, the specific data on medication dosing, strategies (bolus vs continuous infusion), and timing of sedation administration were not recorded. Sixth, clinically relevant outcomes such as ventilator-free days, ICU and hospital lengths of stay, and mortality are not presented in this study. Finally, as a relatively minor concern, the range of set PEEP values was relatively narrow.
Despite these limitations, this analysis does allow conclusions to be drawn with potentially important implications. The currently suggested safety threshold for ΔP is often violated by a strategy that focuses only on boundaries for VT or Pplat. Our findings, obtained in a diverse population of intubated subjects, extend observations and concerns for patients with ARDS.5 Should numerical values for ΔP based on airway pressure alone prove in prospective trials to be the key variable to constrain, vigilance would appear to be especially important in the initial stages of mechanical ventilator support. Finally, attention should be paid to triggering efforts when interpreting and comparing numerical values of ΔP.
Footnotes
- Correspondence: Arianne K Baldomero MD, 1 Veterans Drive (Pulmonary 111-N), Minneapolis, MN 55417. E-mail: baldo004{at}umn.edu.
The authors disclose a relationship with HealthPartners Research Foundation.
Supplementary material related to this paper is available at http://www.rcjournal.com.
See the Related Editorial on Page 1017
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}