

Abstract
BACKGROUND: Endotracheal tubes with standard polyvinyl chloride cuffs create folds on inflation into the trachea, which lead to potential leakage of subglottic secretions into the lower airways and cause lung colonization and pneumonia. The use of a double-layer prototype leak-proof cuff has shown effective prevention of the fluid leakage across the cuff. We hypothesized that the use of such a leak-proof cuff could prevent lung bacterial colonization in vivo.
METHODS: To simulate patients in the ICU, 13 pigs were placed in the semirecumbent position, intubated, and mechanically ventilated for 72 h. Five animals were prospectively intubated with an endotracheal tube with a leak-proof cuff (leak-proof cuff group). Data from 8 animals previously intubated with an endotracheal tube with a standard polyvinyl chloride cuff (standard cuff group) were retrospectively analyzed. Leakage of tracheal secretions across the leak-proof cuff was tested by the macroscopic methylene blue evaluation. Arterial blood gas exchanges and microbiology were tested in all the pigs at necropsy.
RESULTS: In the standard cuff group, all the pigs showed heavy bacterial colonization of the lungs after 72 h of mechanical ventilation, with an overall proportion of colonized lung lobes of 92% (44/48 lobes, 8/8 animals) compared with 27% (8/30 lobes, 5/5 animals) in the leak-proof cuff group (P < .001). These results were strengthened by the absence of methylene blue in the tracheal secretions below the leak-proof cuff. Furthermore, no hypoxemia was demonstrated in the pigs in the leak-proof cuff group after the 72-h experiment (PaO2/FIO2 change from baseline, leak-proof cuff group vs standard cuff group; median difference 332, 95% CI 41–389 mm Hg; P = .030).
CONCLUSIONS: A new leak-proof cuff for endotracheal intubation prevented macroscopic leakage of subglottic secretions along the airways. This mechanism led to the reduction of lung bacterial colonization, which could contribute to the prevention of hypoxemia in the pigs on mechanical ventilation while in the semirecumbent position.
- endotracheal tube cuff
- bacterial colonization
- acute hypoxemic respiratory failure
- ventilator-associated pneumonia
Introduction
Ventilator-associated pneumonia (VAP) is a nosocomial infection that develops in patients on mechanical ventilation for >48 h.1 VAP has an overall attributable mortality of 13%, which can reach up to 69% in surgical patients.2 The presence of a endotracheal tube (ETT) is the leading cause of VAP.2,3 In the ICU, patients who are critically ill and who are sedated, intubated, and on mechanical ventilation are usually in the semirecumbent position. Preclinical studies with large animal models in the semirecumbent position showed that gravity is the key factor that determines leakage of the subglottic secretions along the airways, despite the presence of an ETT cuff.4–7 The lack of a complete seal with an ETT cuff may allow lung colonization and serve as a source for VAP or postextubation pneumonia.8
In previous preclinical studies, our group demonstrated the limitations of the high-volume low-pressure polyvinyl chloride (PVC) cuffs in different experimental conditions.9–11 In an in vitro bench-top study,9 high-volume low-pressure PVC cuffs were not able to prevent fluid leakage, even at inflation cuff pressures as high as 50 cm H2O. Conversely, an ETT cuff prototype made with a double-layer guayule latex cuff (leak-proof cuff) completely prevented fluid leakage even at inflation pressures as low as 20 cm H2O for 24 h.9 The leak-proof cuff showed a superior performance compared with the high-volume low-pressure PVC cuff also in preventing fluid leakage when no positive pressure was applied.10 Furthermore, in an experimental animal model of pigs intubated with an ETT with a high-volume low-pressure PVC cuff and on mechanical ventilation for 72 h without antibiotic administration or bacterial instillation into the trachea, we observed the development of massive lung bacterial colonization.7
Therefore, we hypothesized that, in the absence of exogenous bacteria inoculation along the airways and without antibiotic prophylaxis, a leak-proof cuff could prevent lung bacterial colonization in an experimental pig model enterally fed and on mechanical ventilation for 72 h, which simulates the semirecumbent position of patients in the ICU. In this investigation, we aimed to assess the effects of an ETT with a leak-proof cuff on the prevention of lung bacterial colonization (primary end point) and acute hypoxemic respiratory failure (secondary end point) in an animal model in the semirecumbent position, with continuous enteral feeding and mechanical ventilation for 72 h and without any antibiotic treatment.
QUICK LOOK
Current knowledge
Endotracheal tubes with standard high-volume low-pressure polyvinyl chloride cuffs result in folds on inflation into the trachea, which do not provide an effective seal. The presence of cuff folds leads to potential leakage of subglottic secretions into the lower airways in the semirecumbent position due to the gravitational effect and causes lung colonization and pneumonia. The use of a double-layer prototype leak-proof cuff showed effective prevention of the fluid leakage across the cuff in vitro.
What this paper contributes to our knowledge
In pigs on mechanical ventilation for 72 h while in the semirecumbent position, a new leak-proof cuff for endotracheal intubation prevented macroscopic leakage of subglottic secretions into the airways. This mechanism reduced lung bacterial colonization in the lungs, as shown by the microbiologic findings, the absence of methylene blue below the endotracheal tube cuff, and the prevention of hypoxemic respiratory failure.
Methods
Housing and Husbandry
Animal experiments were conducted in accordance to the Institutional Animal Care and Use Committee at the National Institutes of Health Animal Research Laboratory, Bethesda, MD, where the study has been approved and conducted. National Institutes of Health guidelines were followed.12 The animals were housed in the stables of the animal laboratory of the National Institutes of Health (Bethesda, Maryland). The large animal stable housed multiple animals, and multiple animals were not separated into single cages. The bedding material was composed of wood shavings, wheat, and barley straw. The environmental temperature was kept at 70°F. The animals had free access to food and water. Before starting the experiment, animal welfare was assessed daily and behavioral changes, if present, were immediately reported to the responsible veterinarian of the National Institutes of Heath animal laboratory.
Tracheal Orientation and Animal Preparation
Nothing by mouth status was maintained for 12 h before animal preparation and intubation in both groups. We intubated and mechanically ventilated 5 adult female Yucatan miniature pigs. Animals were purchased by the staff of the animal laboratory (National Heart, Lung, and Blood Institute, National Institutes of Health, in Bethesda, Maryland) in the prone position for 72 h. Propofol (2–6 mg/kg/h) and fentanyl (2–20 μg/kg/h) were continuously infused to maintain general anesthesia. After anesthesia administration, at the time of orotracheal intubation, we intubated the animals with a Mallinkrodt Hi-Lo (Mallinckrodt, Staines-Upon-Thames, UK) with a guayule latex cuff of cylindrical shape (13 mm diameter) and 50–60 μm thick (Yulex, Maricopa, Arizona) draped over the Mallinckrodt Hi-Lo (inner diameter, 7.5 mm) ETT cuff (Mallinckrodt) (leak-proof cuff). A sterile gel (0.5 mL) (Surgilube, Altana, Melville, New York) was added between the 2 cuffs to allow an equal distribution of inflation pressure and to minimize friction among the cuffs (Fig. 1). Therefore, the leak-proof cuff could dilate at low pressures and adhere to the tracheal mucosa without developing folds.9 We named this group the leak-proof cuff group, and the animals received enteral feeding (30 mL/h) through an orogastric tube (Osmolite, diluted 1:1 with tap water, Ross Nutrition, Abbott Laboratories, Columbus, Ohio).

Prototype experimental leak-proof cuff. A layer of highly compliant guayule latex (dotted line) is draped around a standard high-volume low-pressure polyvinyl chloride cuff (dashed line). A sterile gel was added between the 2 cuffs.
We further evaluated, retrospectively, the data of 8 animals that we intubated with an ETT by using a cylindrical shaped high-volume low-pressure cuff (Mallinkrodt Hi-Lo, inner diameter 7.5 mm), an historical control group (no. = 8, two of which received enteral nutrition).7 The leak-proof cuff group was studied by the same investigators (MC, TK, and AZ) and in the same laboratory of the historical control (standard cuff group).7 Beside the study treatment (ETT cuff), the 2 groups only differed by the presence of enteral nutrition (all the animals in the leak-proof cuff group [no. = 5] and 2 of 8 animals in the historical control group). Enteral nutrition is an established risk factor of lung colonization and pneumonia,13–16 which could further challenge the performance of the leak-proof cuff compared with the standard cuff.
The ETT and the trachea were oriented 45° above the horizontal to simulate the semirecumbent position of patients who are intubated while in the ICU. The animals' position and preparation were performed according to Zanella et al7 as previously described. In summary, the extrathoracic part of the trachea runs in parallel with the ventral portion of the animal's neck, the intrathoracic part of the trachea designs an angle of 11° with the spine. To obtain the ETT and the trachea oriented 45° above the horizontal and to simulate a model of the semirecumbent position, the upper part of the bed was angulated 30° above horizontal and a foam pillow was positioned beneath the head of the animal. The study design is depicted in Figure 2.

Study design.
Animal Handling
Animals in the leak-proof cuff group underwent the same handling as the standard cuff group.7 Briefly, mechanical ventilation was adjusted to reach a stable PaCO2 ∼40 mm Hg with a tidal volume of 6–8 mL/kg, with a breathing frequency that ranged from 10 to 20 breaths/min, with an average of ∼14 breaths/min. PEEP was 5 cm H2O. The endotracheal cuff pressure was kept within a range of 25–30 cm H2O and was checked every 6 h from the start of the experiment by using a manual manometer. An open tracheal suction system was used to perform endotracheal suctioning in both groups every 6 h. Neither group was treated with antibiotics either before (≥1 month earlier) or throughout the study, and no bacteria was instilled into the trachea. In the leak-proof cuff group, the presence of macroscopic aspiration across the ETT cuff was further evaluated by methylene blue injection in the supraglottic space 2 times a day. The presence of blue was detected in the tracheal suction at each tracheal aspiration and in the trachea with a bronchoscope 1 and 3 h after methylene blue injection. Recordings of blood gas analyses, plateau pressure, breathing frequency, and mean arterial pressure were obtained at the beginning and at the end of the experiment (72 h). Hypoxemia was defined as an PaO2/FIO2 of <300 mm Hg.
Autopsy and Microbiologic Sampling
All the animals underwent non-recovery procedures. Euthanasia was performed by using an anesthetic overdose (intravenous pentobarbitone) according to the American National Institutes of Health guidelines12 and to Annex IV of the European Directive 2010/63/EU.17 Autopsy was performed after 72 h of mechanical ventilation in all the animals. Removal of the trachea and lungs during autopsy and microbiologic samplings were aseptically performed, as previously described.7 Concisely, lung tissue samples were excised from the innermost portions of each of the 6 lobes (Fig. 3). Lung samples for microbiologic analysis were shipped to the National Institutes of Health microbiology laboratory to evaluate the presence and quantify the levels of the bacterial load (Table 1). Bacteria colonization was expressed as colony-forming unit (CFU) per grams in each tissue sample. Bacterial colonization was defined in the presence of a bacterial load of ≥103 CFU/g.

Description of the 6 sampling sites for microbiologic evaluation along the lungs.
Lung Pathogenic Bacterial Load and Bacterial Colonization
Statistical Analysis
Gas Exchanges and Physiologic Variables.
Data normality was assessed with the Shapiro-Wilk test. Continuous physiologic variables (blood gas analyses [arterial pH]), PaCO2, PaO2/FIO2, respiratory system plateau pressures, breathing frequency, and mean arterial pressure were expressed as median (interquartile range) at different time points (baseline and 72 h). The change of the variables from baseline in each group was expressed as median (95% CI) difference (Table 2). To test the hypothesis that the leak-proof ETT cuff (exposure variable) may prevent acute hypoxemic respiratory failure (outcome variable) after 72 h of intubation and mechanical ventilation, the change in continuous physiologic variables over time was compared by using a 2-way analysis of variance for repeated measurements (72 h vs baseline) by testing the difference between the groups (leak-proof vs standard cuff groups) on the mean change from baseline (group-by-time interaction) (Fig. 4). The Bonferroni correction was used for post hoc comparisons. In addition, the difference of the differences between 72 h and baseline among the groups (leak-proof vs standard cuff groups) was reported as the median and 95% CI difference, and the P value, which compared the differences of the changes from 72 h to baseline between the groups was calculated by using the Mann-Whitney U test (Table 2).
Arterial Blood Gas Analyses and Physiologic Variables

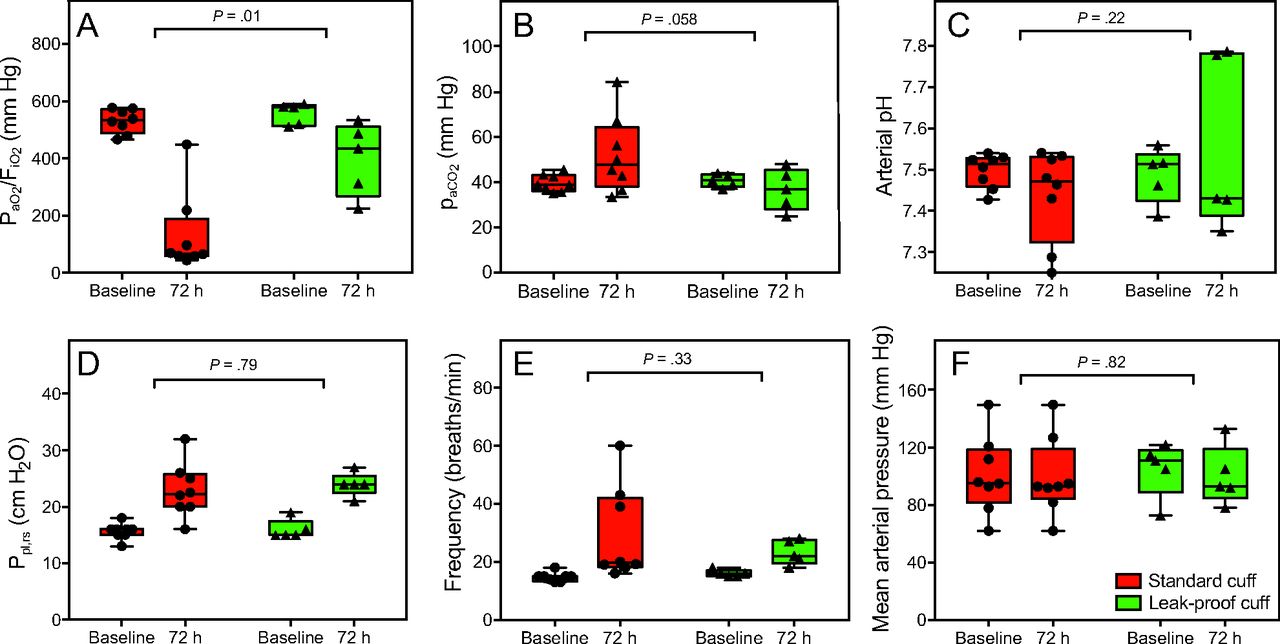
Blood gas analysis and physiologic variables changes over time (from baseline to 72 h) among the standard cuff group and leak-proof cuff group. A: PaO2/ FIO2. B: PaCO2. C: Arterial pH. D: Respiratory system plateau pressure (Ppl,rs). E: Breathing frequency. F: Mean arterial pressure. Continuous variables are graphically expressed as individual data (dots), box plots (median [interquartile range]) with whiskers (range, minimum-maximum). P values (2-tailed) compared groups on the mean change from baseline and were calculated with 2-way analysis of variance for repeated measurements over time.
Microbiologic Colonization.
Locations were expressed in terms of lung lobes (6 locations = 6 lobes). The bacterial load assessed within different animals (pig level) or within different colonized lung lobes (lung lobe level) was described as median (interquartile range) or range (minimum to maximum). To test the hypothesis that the leak-proof cuff (exposure variable) can prevent lung bacterial colonization (outcome variable) after 72 h of intubation and mechanical ventilation, differences between the groups were tested as follows: (1) difference in the proportion of colonized locations calculated as adjusted odds ratio and 95% CI by a logistic regression analysis with robust clustering, in which the presence of lung lobe bacterial colonization was considered the outcome variable, the ETT cuff was considered the exposure variable, and the pigs were considered the cluster variable to adjust the model for the within-animal correlation (primary end point) (Table 3); (2) median difference and 95% CI of the median bacterial loads of the lung lobes (lung lobe level) within different animals (pig level) between leak-proof and standard cuff group, with the P value calculated by using the Mann-Whitney U test (Table 4). The median of the bacterial colonization by location (lung lobes) in both groups was depicted by using the Karnaugh color map (Fig. 5).
Odds Ratio in the Number of Locations of Colonized Lung Lobes by Pathogenic Bacteria on Autopsy Between the Two Groups, Adjusted for Within-Animal Correlation
Median Difference (95% CI) of the Median Bacterial Loads of the Lung Lobes Within Different Animals on Autopsy Between the Two Groups
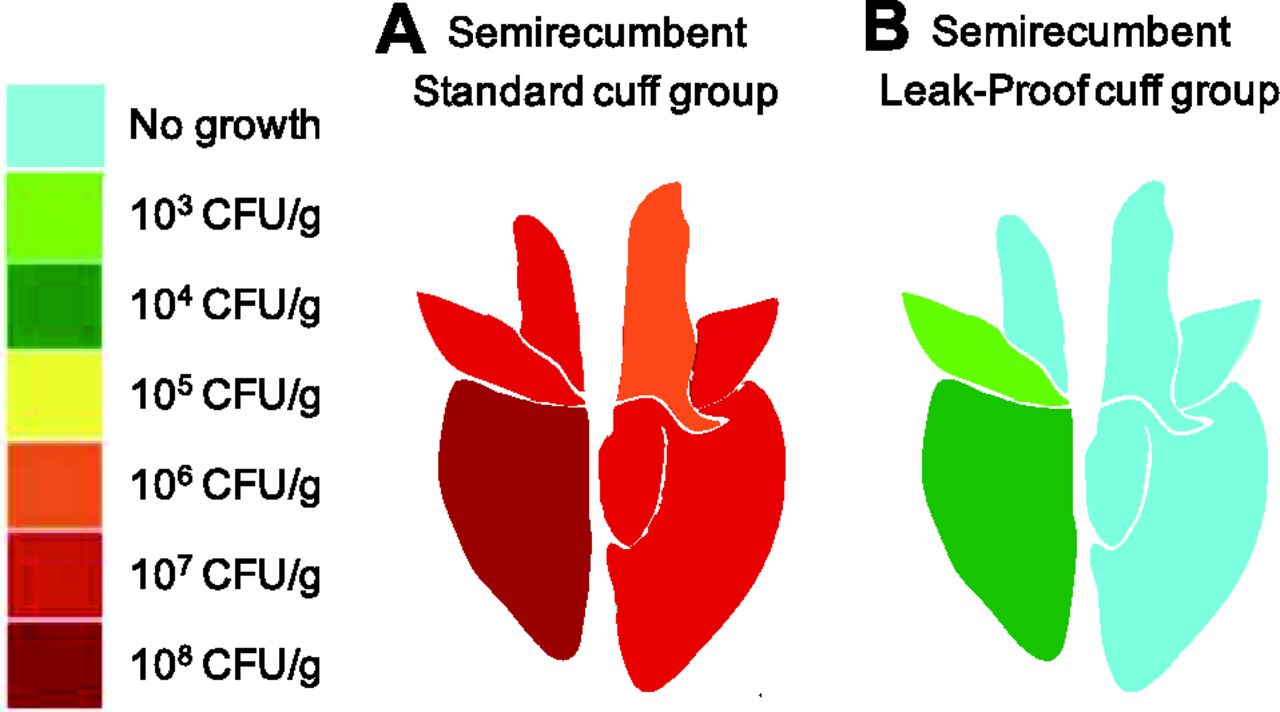
Median of bacterial colonization (CFU/g) in the standard cuff group (A) and in the leak-proof cuff group (B) by location into the lung lobes.
Methylene Blue Assessment.
To evaluate the performance of the leak-proof ETT cuff in preventing macroscopic aspiration into the lower airways, the presence of methylene blue in the subglottic space of the animals was reported as count and proportion.
Statistical significance was reached with P < .05 (2-tailed). Statistical analyses were performed by using STATA-14/MP (StataCorp, College Station, Texas), GraphPad Prism 7a (GraphPad Software, San Diego, California), and Microsoft Excel for Mac 2017, v15.32 (Microsoft Corporation, Redmond, WA).
Sample-Size Calculation
Based on previous studies from our group,7,9 we know that the leak-proof cuff was totally effective in preventing fluid leakage in vitro9 at an inflation cuff pressure at of 25–30 cm H2O. Furthermore, we previously demonstrated that all pigs intubated and on mechanical ventilation for 72 h while in the semirecumbent position showed a severe bacterial colonization at the end of experiment (100% proportion of colonization, outcome of colonization defined as the presence of a bacterial load of ≥103 CFU/g in the sampling locations).7 Our control group (standard cuff group) showed colonization in 44 of 48 lung lobes (92% proportion of colonization, outcome of colonization defined as the presence of a bacterial load of ≥103 CFU/g in the sampling locations (no. = 48, 6 lung lobes in 8 animals).7 We expected that the leak-proof cuff could effectively prevent lung colonization in the pigs intubated and on mechanical ventilation for 72 h with enteral feeding (no colonization [0%], outcome of colonization was defined as the presence of a bacterial load of ≥103 CFU/g in the sampling locations). When using the Fisher exact test to compare 2 independent proportions with a level of significance (α) of 0.05 (2-tailed) and a power (1 − β) of 90%, the minimum required sample size of pigs with the experimental leak-proof cuff was no. = 5. This article adhered to the Applicable Equator guidelines.18
Results
Study Population
Thirteen adult female Yucatan minature pigs (median (IQR) age, 8 [7–9] months; weight, 34 [27–37] kg) were studied and considered healthy based on clinical criteria, laboratory data, and chest radiographs performed the day before the experiment.
Gas Exchanges and Physiologic Variables
At baseline, we did not observe any difference in terms of gas exchange or physiologic variable measurements among the groups. In the standard cuff group, all the animals developed respiratory failure with severe hypoxemia. In the leak-proof cuff group, no animal developed respiratory failure, except one animal showed mild hypoxemia at the end of the experiment (PaO2/FIO2 224 mm Hg). The reduction of PaO2/FIO2 at 72 h in the standard cuff group was significantly greater compared with the PaO2/FIO2 decrease in the leak-proof cuff group (leak-proof cuff group vs standard cuff group, median [95% CI] difference of changes of PaO2/FIO2 from baseline, 332 [41–389] mm Hg, P = .030 [P value compared the median differences from 72 h to baseline between the two groups]) (Fig. 4A and Table 2).
Despite the effort to adjust mechanical ventilation to reach a stable PaCO2 of ∼40 mm Hg over time, PaCO2 at 72 h increased from baseline in the standard cuff group compared with a substantial PaCO2 stability in the leak-proof cuff group (leak-proof vs standard cuff groups, median difference of changes of PaCO2 from baseline −16, 95% CI −32 to −1 mm Hg; P = .030 [P value compared the differences from 72 h to baseline between the two groups]) (Fig. 4B and Table 2).
This happened despite breathing frequency increasing in the standard cuff group by a median 5, 95% CI 1–42; P = .015 breaths/min at 72 h from baseline, whereas the breathing frequency did not significantly change at 72 h compared with baseline in the leak-proof cuff group (frequency, median difference of the differences from 72 h to baseline among the groups 1, 95% CI −24 to 5 breaths/min; P = .91 [P value compared the differences from 72h to baseline between the two groups]) (Fig. 4E and Table 2). Arterial pH remained stable throughout the experiment in both groups (Fig. 4C and Table 2). Similarly, the respiratory system plateau pressure significantly increased from baseline to 72 h both in the standard cuff group (P = .001) and in the leak-proof cuff group (P = .004) (Fig. 4D and Table 2). We did not observe any significant difference in mean arterial pressure over time and between the 2 groups (Fig. 4F and Table 2).
Microbiologic Colonization
The sampling sites are highlighted in Figure 3. In the standard cuff group, 6 of 8 animals (nos. 5621, 5639, 5644, 5661, 8057, 8071) were heavily colonized by different bacteria (bacteria range within the pig level [2, 7] (minimum to maximum) in all 6 lung lobes [range 1.0 × 103 to 2.7 × 109 CFU/g]). The remaining 2 minature pigs showed bacterial colonization (bacteria range within the pig level [2, 3] (minimum to maximum) in 4 of 6 lung lobes (no. 5620, bacterial load range of 3.6 × 103 to 5.2 × 107 CFU/g in 4 colonized lung lobes; no. 5652, bacterial load range of 1.2 × 103 to 3.2 × 103 CFU/g in 4 colonized lung lobes) (Table 1).
In the leak-proof cuff group, pig no. 25 did not present sufficient bacterial load to meet criteria of colonization (28 CFU/g by 3 bacteria in the right middle lobe). Animal no. 19 presented with mild colonization (1.95 × 103 CFU/g) by a single bacterium (Bordetella bronchiseptica) in just 1 of 6 lung lobes. Pigs nos. 906 and 21 showed bacterial colonization (bacteria range within the pig level [2, 3] (minimum to maximum) in 2 of 6 lung lobes [nos. 906 and 21; bacterial load range of 2 colonized lung lobes within the pig level (1.53 × 103 to 1.45 ×106 CFU/g)]. Pig no. 903 presented colonization by 2 bacteria in 3 of 6 lobes (bacterial load range within 3 colonized lung lobes of 1.75 × 103 to 1.73 × 107 CFU/g) (Table 1).
The standard cuff group presented with a significantly greater colonization compared with the leak-proof cuff group, either in the number of locations or in the bacterial load. In the standard cuff group, the overall amount of colonized locations in all 8 animals was significantly greater compared with the number of colonized locations in the 5 animals of the leak-proof cuff group (fraction of colonized sampling locations, leak-proof cuff group vs standard cuff group, 27% vs 92%; adjusted odds ratio 0.03, 95% CI 0.01–0.16; P < .001 [P value of the risk of lung lobes colonization when accounting for the number of animals between the groups] (Table 3). The median (interquartile range) of the median bacterial loads of the 6 lung lobes calculated in each animal in the standard cuff group was considerably greater compared with the median bacterial loads of the lung lobes assessed in the 5 animals of the leak-proof cuff group (leak-proof vs standard cuff group, median difference (95% CI) of the median bacterial loads calculated at the animal level was median −4.5 × 107, 95% CI −2.2 × 108 to −9.3 × 105; P = .002 (Table 4). The median bacterial colonization of the respiratory system by location in the 2 groups are illustrated in Figure 3A (standard cuff group) and B (leak-proof cuff group) by using the Karnaugh color map.
Methylene Blue Assessment, Enteral Nutrition, and Regurgitation
We performed the methylene blue assessment below the ETT cuff in the leak-proof cuff group. None of the 5 animals exhibited any presence of methylene blue along the trachea (0% [0/5 animals]). Furthermore, we did not detect any regurgitation during enteral feeding throughout all the animal experiments in both the leak-proof and the standard cuff group.
Discussion
In this experimental pig model, we investigated the effect of a double-layer guayule latex leak-proof cuff on lung bacterial colonization and blood gas values after intubation, 72 h of mechanical ventilation, and continuous enteral feeding. The principal finding of our investigation was that an ETT with a leak-proof cuff prevented lung bacterial colonization compared with an ETT with a standard high-volume low-pressure PVC cuff. The microbiologic data of lung colonization in the leak-proof cuff group was reinforced by the absence of methylene blue in the tracheal secretions at the macroscopic evaluation.
In a bench-top in vitro trachea study that compared the ability of ETTs with different sealing cuffs to prevent fluid leakage, our group observed that the double-layer guayule latex leak-proof cuff was able to provide an effective sealing of a cylindrical glass tube. Contrarily, the standard high-volume low-pressure PVC cuffs did not effectively prevent the fluid leakage across the cuff. The difference in the average leakage flow among the 2 different cuffs was even more striking when the intra-cuff pressure was maintained as low as 20 cm H2O, and the leak-proof cuff still showed excellent sealing properties. The prototype experimental cuff has a unique mechanical property. The thin guayule latex layer was highly compliant and, when the double-layer cuff was inflated, did not present any folds along the surface. This translated to a physical advantage of the leak-proof cuff, which could prevent the fluid leakage across the cuff. On the contrary, the commercial high-volume low-pressure cuffs had folds along their surface, which allowed fluid leakage across the cuff caused by incomplete sealing of the in vitro trachea.9–11 Our results confirmed in vivo the efficacy of the prototype leak-proof cuff in preventing subglottic secretion leakage for the first time and, hence, in blocking the pathway to lung bacterial colonization. Therefore, although we could not exclude the presence of microaspiration because the bacterial load in the leak-proof cuff group was not abolished but remarkably decreased, the use of a macroscopic technique such as the methylene blue evaluation in the trachea indicated that a double-layer guayule cuff prevented leakage by averting macroaspiration.
Many factors are involved in the process that leads to lung colonization during mechanical ventilation. All of these factors are linked to the ETT, the key factor of lung parenchyma colonization. Colonized subglottic secretions that leak across the folds of the ETT cuff,7 ineffective mucociliary clearance caused by the cuff,5 impairment of the protective cough reflex after endotracheal intubation,19 aerosolization of the biofilm along the inner surface of the ETT that acts as a bacterial reservoir,20 and the development of atelectasis21 all contribute to increase the risk of lung colonization and, eventually, pneumonia. Furthermore, in the semirecumbent position, gravity directly acts on lung colonization and pneumonia, as described in both animal models4,7,8,22 and human subjects,23,24 and as recently confirmed by the Gravity-trial Network.24 As shown in clinical studies, although the shape does not affect the frequency of pneumonia,25,26 the material of the ETT cuff can exhibit a different performance in terms of pneumonia prevention.27–29 Of note, no animals in the leak-proof cuff group showed colonization of the left lobes. On the contrary, colonization was mostly present in the right middle and lower lobes, which suggested a gravitational effect on the development of colonization and confirmed previous findings reported by Li Bassi et al.30
Our pig model was suitable to consider a translation of the results into clinical practice because pigs are omnivores and share a similar physiology of the gastrointestinal tract to humans.31 However, even without bacteria inoculation in the trachea, lung bacterial colonization was most likely enhanced by a series of factors of the animal model studied, that is (1) prolonged intubation in semirecumbent position; (2) the position of the trachea below the esophagus further increased the likelihood of pooled secretions leaking into the subglottic area rather than into the esophagus; (3) a lack of oropharyngeal disinfection and antibiotic administration; and (4) a relevant bacterial load of the oropharyngeal flora compared with humans. Despite this, we observed that the use of a double-layer guayule cuff was able to substantially prevent lung bacterial colonization compared with a high-volume low-pressure PVC cuff.
A second finding in our investigation was the observation that the double-layer leak-proof cuff could prevent a significant worsening of the PaO2 compared with a standard high-volume low-pressure PVC cuff after 72 h of mechanical ventilation. Although the leak-proof cuff group presented a normal PaO2 at the end of the experiment, the standard cuff group presented with severe hypoxemia. Furthermore, in the standard cuff group, all the animals presented with respiratory distress, with a significant increase in breathing frequency to maintain normal PaCO2 levels. The difference in terms of lung lobe colonization among the groups could explain the difference in the blood gas variables between the 2 groups. Previous studies in sheep in the semirecumbent position showed a high incidence of lung colonization. This caused inflammation of the lung parenchyma and led to hypoxemia, a pathophysiologic sign of respiratory failure.4,5,7,8 Results of our study indicated that the change of a single variable during intubation and mechanical ventilation (ETT cuff) might play a major contributing role in the multifaceted pathogenesis of VAP because it can radically influence the risk of lung bacterial colonization.
A double-layer guayule latex leak-proof cuff effectively sealed the trachea because of the lack of folds within its surface, and this eventually prevented the development of acute hypoxemic respiratory failure and maintained the blood gas values within normal ranges. This finding was of potential clinical interest when also considering the relative minimum cost of the ETT cuff in a clinical scenario of high VAP health-care–associated costs.32 Of note, the outer layer of the leak-proof cuff was composed of guayule latex material, in which the presence of protein was negligible, which also makes it suitable for subjects who are latex sensitive.33,34
This animal work had several limitations that we should take into account. First of all, the study specifically focused on lung colonization and blood gas values without considering the clinical criteria of pneumonia, analyses of tissue macroscopy, and histopathology. Second, the 2 animal groups were not randomized. In the leak-proof cuff all 5 animals received enteral feeding, whereas 2 of 8 animals of our historical control (standard cuff group) received enteral feeding, which is an established risk factor of lung colonization and pneumonia.13–16,35 Enteral feeding might have allowed an underestimation of the efficacy of the leak-proof cuff in preventing lung bacterial colonization. Third, we did not analyze the bacteria of the oropharyngeal flora to determine whether there was any correlation with the bacteria reported in the lungs of the animals or if there had been any change in the nature of the bacterial species in the oropharynx from the beginning until the end of the experiment. Fourth, methylene blue evaluation by bronchoscopy was not performed in the historical control group. However, frequent cuff pressure checks (ie, range 25–30 cm H2O) and the delivered PEEP (ie, 5 cm H2O) were performed to maintain the same experimental conditions of the control group.
Conclusions
This study aimed to clarify, for the first time to our knowledge, the in vivo efficacy of a leak-proof cuff in the prevention of lung colonization after 72 h of mechanical ventilation in pigs by simulating the semirecumbent position of patients in the ICU. The results of the present animal investigation indicated that an ETT with a leak-proof cuff could effectively prevent lung colonization by completely sealing the trachea, which stopped the leakage of the subglottic secretions into the airways. This effect prevented respiratory failure and hypoxemia in our pig animal model. Future human feasibility and/or efficacy studies aimed at confirming the prevention of VAP and use of the leak-proof cuff for a prolonged period of time (>72 h) are warranted.
Acknowledgments
We thank Dr Robert F Hoyt, Randall Clevenger, Kelly Cole, Dave Caden, Phyllis Levin, Arthur Zetts, Timothy Hunt, Kenneth Jeffries, Karen Keeran, Gayle Zywicke, and Danielle Springer for their assistance throughout the animal studies. We thank Dr Katrina Cornish and Jali Williams (Yulex Corporation, Maricopa, Arizona) for manufacturing and providing the double-layer guayule latex leak-proof cuff to the authors without charge and without additional financial support.
Footnotes
- Correspondence: Alberto Zanella MD, Dipartimento di Anestesia, Rianimazione ed Emergenza Urgenza, Fondazione IRCCS Ca' Granda - Ospedale Maggiore Policlinico, Dipartimento di Fisiopatologia medico-chirurgica e dei trapianti, Università degli Studi di Milano, Via Francesco Sforza 35, Milan 20122, Italy. E-mail: alberto.zanella1{at}unimi.it.
This study was supported by the National Research Program, National Heart, Lung, and Blood Institute, National Institutes of Health, Intramural Research, Bethesda Maryland.
The study was performed at the animal laboratory of the National Institutes of Health in Bethesda, MD, directed by Dr Kolobow.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1170
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}