

Abstract
BACKGROUND: Studies on the effect of transitional care on hospital readmissions have reported inconsistent findings, and the effect on mortality has not been reviewed systematically. This systematic review and meta-analysis of randomized controlled trials aims to examine the effect of transitional care interventions on COPD-related readmissions, all-cause hospital readmissions, and all-cause mortality rates in subjects with COPD.
METHODS: Electronic databases (CINAHL, Embase, Scopus, MEDLINE, Cochrane, PubMed, Web of Science, Airity, BMJ Respiratory Research Journal, and National Digital Library of Theses and Dissertations) were searched from inception to April 26, 2017. Online searches were conducted using key words and MeSH terms for COPD and transitional care. Entry terms for searching included chronic obstructive pulmonary disease, COPD, COPD transitional care or care transition, continuity of patient care, patient discharge, and patient transfer. The quality of the included trials was assessed using the Cochrane Collaboration tool.
RESULTS: 13 randomized controlled trials met the inclusion criteria. Transitional care significantly reduced the risk of COPD-related readmissions (odds ratio = 0.599, 95% CI 0.421–0.852) and all-cause hospital readmissions (odds ratio = 0.720, 95% CI 0.531–0.978), but not that of all-cause mortality (odds ratio = 0.863, 95% CI 0.576–1.294) in subjects with COPD. The effects of transitional care on hospital readmissions were moderated by the duration of interventions, type of care providers, and use of telephone follow-up as an element of the intervention.
CONCLUSIONS: There was a significant effect of transitional care on both COPD-related and all-cause hospital readmissions in subjects with COPD. Duration of interventions, type of care providers, and use of telephone follow-up appeared to moderate the beneficial effects of transitional care.
Introduction
COPD affects 210 million people globally and accounts for 4 million deaths annually. In 2002, it was the fifth most common cause of death, and it is projected to become the fourth most common cause of mortality by 2030.1 COPD is a common, preventable, and treatable disease with characteristics including persistent respiratory symptoms and chronic air-flow limitation caused by airway narrowing or alveolar abnormalities as a result of cumulative exposure to harmful gasses and particles combined with host factors.2 The pathological characteristics of COPD include irreversible air-flow obstruction and abnormal inflammatory responses in the lungs that represent innate and adaptive immune responses to long exposure to toxic agents. This response may lead to hypersecretion of mucus, tissue destruction, and disruption of normal repair and defense mechanisms, all of which result in inflammation of small airways and fibrosis.3 When advanced, these responses can cause pulmonary hypertension, cor pulmonale, and left heart dysfunction.4,5 Thus, morbidity from COPD may be directly related to physiological defects and can be concomitant with other chronic conditions. Furthermore, the worsening of pulmonary inflammation in COPD might cause frequent disease relapse, prolonging physiological recovery and leading to repeated acute care demands.6,7 High COPD exacerbation incidence strongly corresponds to high morbidity, mortality, and hospital readmission rates; high frequency of emergency visits; worsened health-related quality of life; and high costs.6–11
These issues exacerbate various burdens on individual patients, families, and the health care system. Patients with COPD discharged without home care are likely to be readmitted.12 Approximately 24% and 43% patients with COPD are readmitted at least once for any reason within 30 d and 90 d after discharge, respectively.13 The risk factors for rehospitalization in patients with COPD vary depending on the patient's conditions,14,15 care provider, and system factors.14 Other risk factors for rehospitalization include old age at diagnosis, COPD severity, current smoking habit, patient deprivation, intervention before admission, low body mass index, and comorbidities.14,16 Among these factors, 2 modifiable risk dynamics of early readmission for patients with COPD are provider and system aspects.14 When the readmission rate is high and unexplained, it reflects problems in the transition process and post-discharge management.17 Health care providers in acute care settings should carefully review the discharge process to mitigate readmission risks.13 Furthermore, because evidence indicates a correlation between the readmission rate and mortality rate, health care services should ensure proper comorbidity management and resource allocation to identify, review, and increase management for patients with COPD at particular risk of hospital readmission.18 Evidence suggests that patients with COPD readmitted for a comorbid condition, such as infarction, pneumonia, septicemia, or pulmonary heart disease, are more likely to die within 30 d than are those readmitted with COPD alone.19 Properly managed and effective care transitions for patients with COPD can mitigate the risk of readmission and mortality, particularly for those who require complex care from a wide range of services.
Transitional care has been adopted by some health systems as a discharge intervention for patients with chronic conditions. Transitional care refers to a time-limited intervention designated to promote safety and timely transfer of patients between levels of health care or across care settings.20,21 Evidence indicated that transitional care components varied among the existing models, which mostly included predischarge and postdischarge elements and were delivered by a multidisciplinary team.20,22 However, transitional care for patients with COPD remains challenging due to the complexity of disease conditions. Although a meta-analysis showed effectiveness of transitional care in reducing hospital readmission rates in subjects with COPD at > 6 and 18 months after discharge,23 this effect was found in a meta-analysis involving only a few studies including papers published from 1999 to 2013. With such a small number of analyzed trials, findings of the effectiveness of transitional care on readmission have been inconclusive. Through searching more databases, this meta-analysis was conducted to provide updated evidence on the effect of transitional care for subjects with COPD in order to inform clinical practice. Moreover, the effect of transitional care interventions on mortality has not been examined systematically. To elucidate this effect, this meta-analysis examined the effect of transitional care interventions on hospital readmissions and mortality rates in adults with COPD. Additional analyses were performed to identify potential moderators of the effects of transitional care on outcomes and to identify sources of heterogeneity across studies, if any, by analyzing covariates in moderator analyses.
Methods
This meta-analysis included randomized controlled trials with participants who were ≥ 18 y old and diagnosed with COPD. Trials were included if the study utilized transitional care interventions prior to hospital discharge, or after hospital discharge, or if the study used bridging programs (Fig. 1). We compared a transitional care intervention with any form of nontransitional care, defined by primary studies as conventional care, usual care, standard care, or no treatment. This analysis included studies that reported COPD-related readmissions, all-cause hospital readmissions, COPD-specific mortality, and all-cause mortality as study outcomes.

Flow chart. RCT = randomized controlled trial.
The Preferred Reporting Items for Systematic Review and Meta-Analysis24 was adopted to specify objectives and methods of this meta-analysis. Ten electronic databases (ie, CINAHL, Embase, Scopus, MEDLINE, Cochrane, PubMed, Web of Science, Airity, BMJ Respiratory Research Journal, and the National Digital Library of Theses and Dissertations) were searched with no limit on language, date of publication, or outcomes for records until April 26, 2017. MeSH terms used as key words for searching articles encompassed chronic obstructive pulmonary disease, COPD, COPD transitional care or care transition, continuity of patient care, patient discharge, and patient transfer. Reference lists of the included trials were screened to identify relevant articles for this study that could have been missed during the article search.
All identified duplicate papers were removed. A 2-step trial selection was then performed by 2 reviewers [ESR and YLW]. First, the titles and abstracts were screened independently by the 2 reviewers. Second, full texts of the potential eligible articles were retrieved and reviewed by the reviewers independently based on the eligibility criteria. Consensus was reached by the 2 reviewers on the eligible references to be included for further synthesis and analysis.
We performed the methodology quality assessment. The quality of the study for individually included trials was assessed independently by the 2 reviewers using the Cochrane Collaboration tool for assessing risk of bias in randomized trials, as summarized in Table 1. Each reviewer made impartial determinations of the risk of bias of each study, focusing on random-sequence generation, allocation concealment, blinding of participants, health care personnel, outcome measurement, data collectors, outcome assessors, and any reported bias. The 2 reviewers discussed to reach consensus on any disagreements before the result was presented to the third reviewer for final decisions.
Risk of Bias Summary of Methodological Quality for Each Included Trial
Data were extracted independently by the 2 reviewers; the required modifications were made based on reviewer agreement. Any disagreements were resolved through discussion to find consensus. Information extracted from individual trials included participants' characteristics, study design, interventions, and outcome measures. All outcomes of interest at the final follow-up were extracted.
Statistical Analysis
Effect size of transitional care interventions was measured as odds ratios (ORs) with 95% CIs by using random-effect models due to differentiation of true treatment effects in each study. Heterogeneity across included trials was assessed using the Q test and I2 statistics. A Q ≥ 0.05 and I2 < 50% were considered homogeneous between trials, whereas substantial heterogeneity was defined as Q < 0.05 and I2 > 50%.25 We performed the Begg rank correlation test and the Egger intercept test with a significance level of 0.05 to assess for publication bias in all included studies. A funnel plot was also created as a visual tool to determine publication bias.26 Moderator and meta regression analyses were performed to identify sources of heterogeneity and potential moderators of the relationship of transitional care with readmission and mortality. Data were analyzed with Comprehensive Meta-Analysis Software 2.0 (BioStat, Edgewood, New Jersey).
Results
Identification of the Trials
Searches of the 10 electronic journal databases identified 702 articles. After removing duplicate articles, we screened titles and abstracts of 170 articles for eligibility. Studies were discarded if they provided interventions other than transitional care for subjects with COPD or were not randomized controlled trials. For further assessment, 38 full-text studies were retrieved. We excluded studies that did not have outcome data of interest,16 did not meet inclusion criteria,6 and addressed transitional care in COPD and other diseases.3 We retained 13 trials that met the inclusion criteria for quantitative meta-analysis.
Study Characteristics
The characteristics of the 13 included trials are summarized in Table 2. In total, 2,029 subjects diagnosed with COPD were included. The mean age of trial participants was 69.9 y (range 64.4–76.4 y); 60% of the participants were male. Of those included in the trials, 69.2% were categorized as having severe COPD with average predicted value of FEV1 = 42.2% (36%–47.6%). Severe COPD was identified in 9 studies.27–35 The subjects' comorbid index at baseline was addressed in 5 trials.27,28,30,34,36 Nine trials28,30–37 included active-smoker subjects. Most included trials had 2 arms divided into transitional care and usual care groups, with 1,096 (54%) and 933 (45%) subjects, respectively. In terms of geographical locations, 2 studies (15.3%) studies were conducted in the United States, 6 (46.1%) in European countries, and 5 trials (38.4%) in the Asia-Pacific region. In terms of outcomes, one study presented both COPD-related and all-cause hospital readmissions as outcomes. Nine studies only had the data on all-cause hospital readmissions, three had only the outcome on COPD-related readmissions, and one study had both data all-cause and COPD-related readmissions. 6 studies presented outcome data on all-cause mortality, and 1 study had data of COPD-specific mortality.
Summary Characteristics of Included Trials
The 13 trials varied in elements of intervention: 5 trials (38.5%) included structure assessment as an intervention element;28,31,33,34,38 8 studies (61.5%) provided predischarge education and training;27,28,31,33,34,38 2 studies (15.3%) consisted of a structured care plan;27,28 7 trials (53.8%) involved a home visit program;28,29,34,35,37–39 8 studies (61.5%) included telephone follow-up;28,31–36,38 and 5 studies (38.4%) encompassed a postdischarge educational program.30,34,36,38,39 Six trials (46.1%) comprised other follow-up methods and extended interventions, such as web-based applications,27,28 educational booklets,37 telemonitoring,35 24-h access to respiratory nurses and out-patient arrangements,33,34 and structured exercise and supervision programs.30
The median intervention duration was 3 months (range, 2–14 months). The duration of intervention was ≤ 6 months in 8 studies (61.5%) and > 6 months in 6 trials (38.5%). Intervention providers were classified into a single profession (38.5%) or multiple professions (ie, multifaceted interventions; 61.5%). Most trials compared transitional care with usual care. Notably, one trial compared early discharge with home treatment supported by respiratory nurses and conventional treatments with hospital management for patient exacerbations of COPD.29 Another trial37 evaluated the effects of home-managed support on hospital readmission as compared with usual care (ie, standard hospital admission).
Pooled Effects
Figure 2 presents the pooled effect of transitional care on all-cause hospital readmission from 10 included trials (OR = 0.720, 95% CI 0.531–0.978, P = .035). This finding indicated that transitional care had a significant effect on reducing all-cause hospital readmissions.
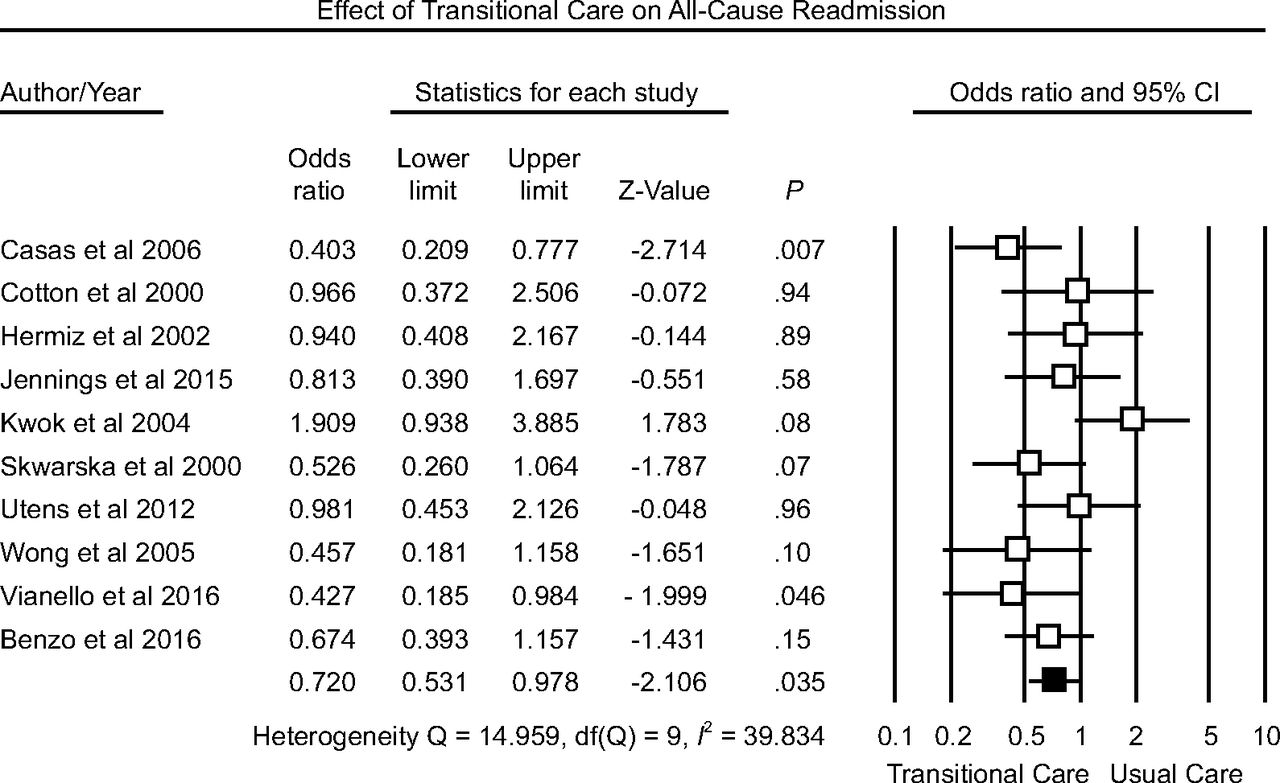
Forest plot of effect sizes and pooled odds ratios of transitional care intervention for trials measuring all-cause hospital readmission in subjects with COPD using a random-effect model. Data on the events of all-cause hospital readmission were obtained from 10 trials. The black square represents the summary statistic, and lines show 95% CI. A heterogeneity test on each subgroup's analysis showed no evidence of heterogeneity among studies.
Four studies provided the data on the events of COPD-related hospital readmission (Fig. 3). The pooled OR was 0.599 (95% CI 0.421–0.852, P = .004), indicating a significant effect of transitional care on reducing the odds of COPD-related hospital readmissions.

Forest plot of effect sizes and pooled odds ratios of transitional care intervention for trials measuring COPD-related readmission in subjects with COPD using a random-effect model. Data on the events of COPD-related hospital readmission were obtained from 10 trials. The black square represents the summary statistic, and the lines show 95% CI. A heterogeneity test on each subgroup's analysis showed no evidence of heterogeneity among studies.
The effects of transitional care on mortality rate were presented from 6 studies that provided data on the all-cause mortality (Fig. 4). There were 1,117 subjects with COPD from the 6 included studies (pooled OR = 0.863, 95% CI 0.576–1.294, P = .48). This finding indicated that the effect of transitional care interventions on mortality rate was not statistically significant.

Forest plot of effect sizes and pooled odds ratios of transitional care intervention for trials measuring all-cause mortality rate in subjects with COPD using a random-effect model. 6 studies provided data on the events of mortality. The black square represents the summary statistic, and lines show 95% CI among homogenous studies.
Publication Bias
Results from both the Begg rank correlation and the Egger regression test did not reveal significant publication bias among the studies assessing COPD-related hospital readmission (P = .73 and P = .54, respectively), among those assessing all-cause hospital readmissions (P = .85 and P = .84, respectively), and among those assessing mortality (P = .060 and P = .15, respectively).
Moderator Analyses
We conducted moderator analyses to determine the effect of 3 dichotomous moderator variables on the relationship between transitional care and readmission. Table 3 presented results of all included trials with outcomes on either COPD-related or all-cause readmissions. Eight studies had intervention duration of ≤ 6 months or shorter, and 6 studies had an intervention duration of > 6 months. The pooled ORs of the group with intervention duration of ≤ 6 months or shorter and that of the group with intervention duration of > 6 months were 0.930 (P = .63) and 0.531 (P < .001), respectively; the point estimates between the 2 groups were significantly different (P < .001).
Results of Moderator Analyses on All-Cause and COPD-Related Hospital Readmission
In 9 studies,27,28,31,32,34–36,38 interventions were provided by multidisciplinary teams, whereas in 5 studies29,30,36,38,39 the interventions were delivered by care providers of a single profession. The pooled ORs were 0.693 for studies using multiple professions (95% CI 0.519–0.925, P = .01) and 0.667 for studies used a single profession (95% CI 0.427–1.043, P = .07); the pooled ORs between the 2 groups were significantly different (P = .002).
Eight studies28,31–34,38 included telephone follow-up, and 6 studies27,29,30,37,39 did not include telephone follow-up as an intervention element. The point estimates were 0.668 for studies using telephone follow-up (95% CI 0.482–0.926, P = .02) and 0.707 for trials not including telephone follow-up (95% CI 0.491–1.018, P = .062); the point estimates were significantly different between the 2 groups (P = .002).
The pooled results of moderator analysis, which included 10 studies with the outcome of all-cause hospital readmissions, indicated a significant effect of duration intervention in moderating the association between transitional care and readmission. The pooled OR was 0.982 (95% CI 0.705–1.367, P = .91) for studies with an intervention duration of ≤ 6 months, whereas the pooled OR for studies with an intervention duration of > 6 months was 0.532 (95% CI 0.373–0.734, P < .001); the point estimates between the 2 groups were significantly different (P = .007). However, the type of care providers and the use of telephone follow-up did not moderate the relationship between transitional care and all-cause hospital readmissions significantly (P = .051 and P = .054, respectively). Moreover, the findings of a meta regression analysis, performed with age and sex as predictors, revealed that age and percentage of males were not significantly associated with the effect size of transitional care for hospital readmissions (P = .25 and P = .068, respectively).
Discussion
Our meta-analysis examined the effect of transitional care interventions on hospital readmissions and mortality in subjects with COPD. We identified 13 trials that provided data on outcomes of interest for 2,029 subjects. Our findings indicate a significant effect of transitional care on reducing all-cause hospital readmissions and COPD-related readmissions in subjects with COPD. The odds of all-cause and COPD-related readmissions for those who received transitional care interventions decreased by 28% and 44%, respectively. Our findings also indicate that transitional care interventions were not significantly associated with reduced all-cause mortality rate.
Although characteristics of transitional care interventions vary considerably across different systems of care, our findings support the valuable role of a transitional care approach in reducing frequent use of health care services by patients with COPD. The progression of COPD varies widely among patients; some patients have stable courses of progress, whereas others have persistent episodes of breathlessness, frequent acute relapses, and respiratory failure.40 Worsening airway function and COPD symptoms can be triggered by infection or air pollution. The triggers are preventable; however, failure to prevent them can lead to advanced disease severity, morbidity, negative effects on health-related quality of life, and mortality.6,7,9 These can account significantly for the consumption of health care resources.41 The worsening of COPD symptoms is related to frequent use of health care services; thus, discharge management to improve continuity of care has a role in eliminating the triggers of disease progression. A review indicated that when patients with COPD endure ongoing hospital treatments or emergency visits caused by exacerbation, care continuity is crucial in maintaining fragmented treatment regimens and providing necessary responses to any changes in a patient's respiratory system or prognosis.42 Furthermore, our findings concur with several meta-analyses showing the importance of transitional care interventions as programs with clinically meaningful effects in reducing the odds of patient readmissions and emergency visits in populations with heart failure.43,44 Similarly, a previous study showed that a transitional stroke program reduced the odds of 30-d readmission by 48%.45 Our findings suggest the importance of transitional care as a tool to reduce hospital readmissions for patients with COPD.
Our moderator analyses revealed the significant effects of the care provider type, intervention duration, and telephone follow-up on the relationship between transitional care and hospital readmission. This finding can provide additional explanations regarding factors that may modify the success of the transitional care intervention in reducing hospital readmissions in patients with COPD, even though evidence on these elements of interventions may highlight some inconsistencies. Our findings concur with those from previous studies46,47 that a multidisciplinary team intervention may decrease 30-d readmission rates and other forms of hospitalizations compared with usual care. In addition, the narrative analysis conducted by Hickman et al48 supported the notion that a multidisciplinary team underpinned with clear communication strategies can reduce readmission rates, mortality, and functional decline of older people. Furthermore, to some extent, the use of telephone follow-up provides beneficial effects on transitional care. Although Mistiaen and Poot49 presented inconclusive evidence of the effectiveness of telephone interventions for managing postdischarge problems, other studies reported telephone follow-up as low-cost, feasible, and no-harm interventions.50–52 Thus, the transitional care intervention has a greater effect on reducing hospital readmission when the intervention lasted for > 6 months, was provided by a multidisciplinary team, or incorporated telephone follow-up as an intervention element.
This meta-analysis found that transitional care interventions were ineffective in reducing mortality rates in subjects with COPD. In all included trials, one study reported a significant effect of transitional care for COPD-specific mortality, whereas other trials failed to support a beneficial effect of transitional care on all-cause mortality. The elements of transitional care interventions may require adjustments to more effectively address the mortality risk. Mortality risk factors for COPD are associated with acute relapse events and depend on the synergistic effect of predictive factors as well as the result of systematic care and prognosis effects of exacerbation.6 However, this finding should be interpreted with caution because it suggests that specific elements of transitional care interventions may be required to reduce mortality rates among patients with COPD.
This study has several limitations. First, heterogeneity across studies might have arisen from differences in intervention designs and assessment tools. Moderator analyses were likely insufficient for exploring whether intervention duration, care provider type, and telephone follow-up reduced mortality rates because the numbers of such studies were limited. Second, the results should be interpreted with caution because many included trials were subject to selection, performance, and detection bias as a result of ineffective concealment or lack of blinding to participants, research personnel, and outcome assessors.
Conclusions
Transitional care can be an effective approach for addressing the high number of hospital readmissions of patients with COPD. However, evidence of the beneficial effect of transitional care on the mortality rate of patients with COPD remains insufficient. The effects of transitional care interventions on hospital readmissions are moderated by the intervention duration, multidisciplinary approach, and use of telephone follow-up. Because patients with COPD vary in disease conditions, in risks of being readmitted to the hospital, and in risks of mortality, it is important to tailor transitional care interventions according to disease-related factors.
Footnotes
- Correspondence: Pei-Shan Tsai PhD, School of Nursing, College of Nursing, Taipei Medical University, 250 Wu Xing Street, Taipei, Taiwan. E-mail: ptsai{at}tmu.edu.tw.
Mr Ridwan has disclosed a scholarship provided by the Indonesia Endowment Fund for Education and the Ministry of Research, Technology, and Higher Education. The other authors have disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}