

Abstract
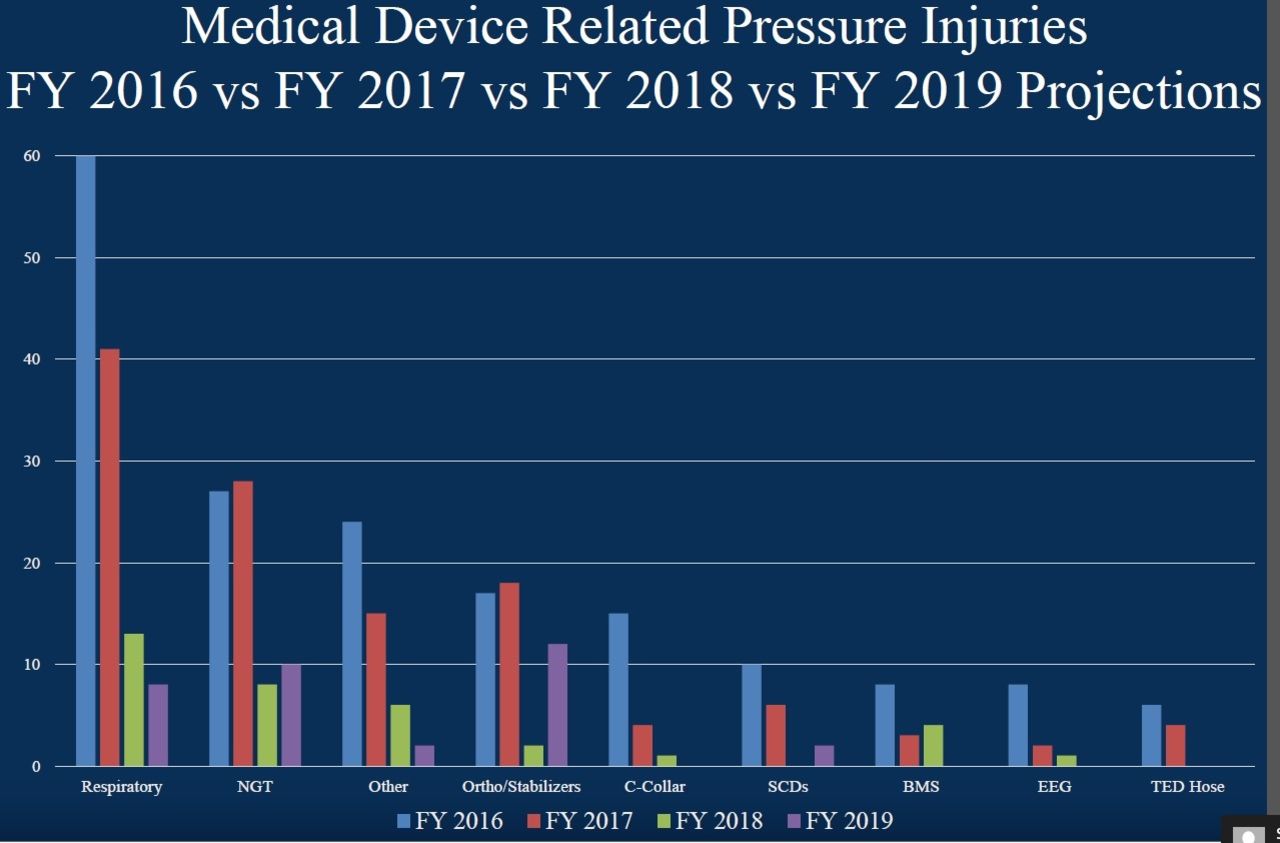
Background: The FY2016 Agency for Healthcare Research and Quality (AHRQ) Quality Indicators report indicated our hospital had a performance worse than expected O/E ratio for PSI 03 Pressure Ulcer Rate. We have had a Pressure Ulcer Prevention (PUP) team in place actively working to manage and reduce hospital acquired pressure ulcers (HAPU) within the Department of Nursing. Data routinely compiled by our Wound Ostomy Care Department provided detailed information on pressure injuries by type and location occurring in the hospital. In FY16, 40% of all HAPU were medical device related pressure ulcers (MDRPU); 37% of all MDRPU were respiratory device related. An opportunity existed to reduce respiratory device related HAPU with a collaborative effort between Respiratory and Nursing Departments. Methods: Initially, we developed a Pareto chart to identify what devices caused the most respiratory related injuries. OETT and NIV masks accounted for 57% of respiratory device related injuries in FY 16. We focused on two goals in adult ICU patient population. Our first goal was to decrease pressure injuries related to OETT devices in the ICU by 30% for FY2017. Our second goal was to decrease pressure injuries related to NIV masks by 15% for FY2017. Using brainstorming, our group identified possible causes and solutions related to OETT and NIV pressure injuries. With this data, we created an effort/yield matrix and a focused action plan on reducing pressure injuries which included standardization of OETT and NIV maintenance and rotation processes, education of RT and nursing staff on these protocols, concurrent rounding audits of adherence to the protocols with immediate feedback to caregivers, and proper ventilator arm positioning, repair or replacement as necessary. Results: Our results exceeded both of the goals. On our goal to decrease pressure injuries related to OETT/securement devices in the ICU by 30%, we attained a decrease of 57% from 21 in FY2016 to 9 in FY2017. The second goal was to decrease pressure injuries related to NIV masks in the intensive care units by 15%, and we attained a decrease of 31%. Conclusions: In conclusion, the collaboration of both respiratory staff, nursing staff and Wound Ostomy Care Department to reduce respiratory device related injuries proved successful. We continue to show improvement and meet quarterly to review data and ensure that identified reduction strategies continue to prevent respiratory device related injuries.

Footnotes
Commercial Relationships: None
- Copyright © 2019 by Daedalus Enterprises




{kind=link}