

Abstract
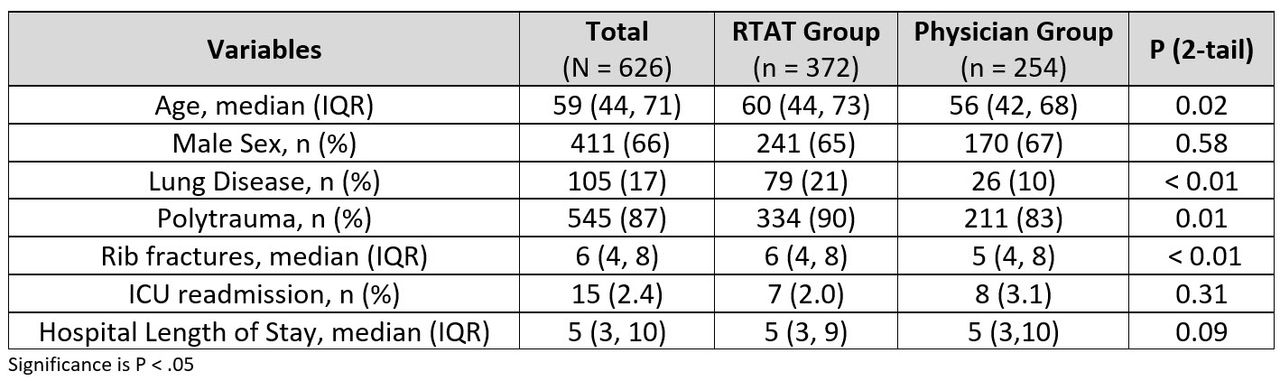
Background: Patients with acute rib fractures have significantly higher rates of pulmonary related complications and increased ICU readmissions from acute care units. A Respiratory Therapy Assess and Treat protocol (RTAT) was developed to assess and manage respiratory care interventions based off a scored patient assessment algorithm. We sought to determine if an RTAT Protocol impacted outcomes when compared to a physician directed approach. Null hypothesis: Among adult subjects with > 3 rib fractures, there is no association in pulmonary related ICU readmissions when comparing a RTAT Protocol Group to a Physician-ordered Respiratory Care Treatment Group (Physician Group). Methods: This was an IRB approved single-center retrospective and prospective analysis. Data from 626 subjects was evaluated. The Physician Group (n = 254) was evaluated from January 2016-December 2016. RTAT Protocol Group (n = 372) was evaluated from June 2017-December 2018. The primary outcome was pulmonary related ICU readmissions between Groups. Secondary outcomes were age, presence of lung disease, prevalence of polytrauma, hospital length of stay and number of rib fractures. Descriptive characteristics are reported as median (IQR) and frequency count (%). Chi-square of independence and Mann-Whitney U tests were applied as appropriate. Alpha (2-tailed) < 0.05. Factors independently associated with pulmonary related ICU readmissions were assessed by multivariate logistic regression modeling. Results: There was no difference in pulmonary related ICU readmissions when comparing the RTAT Group (1.9% [n = 7/372]) to the Physician Group (3.1% [n = 8/254]); P = 0.31. Multivariate logistic regression modeling revealed the following variables were independent predictors of respiratory related ICU readmission: Presence of lung disease (OR 5.3 [1.7-16.4], P <0.01) and Group assignment (OR 0.31 [0.09-0.96], P = 0.04). There was a difference in age (P = 0.02), Presence of lung disease (P < .01), polytrauma (P = .01) and number of rib fractures (P < .01) in the RTAT managed Group (Table). Conclusions: There was no difference in the relationship between pulmonary related ICU readmissions when comparing a RTAT Protocol to physician ordered therapy. The RTAT Group had greater age, higher prevalence of lung disease, polytrauma and number of rib fractures compared to the Physician Group. In a predictive model, the RTAT Group was found to have less likelihood of a pulmonary related ICU readmission.

Footnotes
Commercial Relationships: Drager, Phillips, Mallinckrodt
- Copyright © 2019 by Daedalus Enterprises




{kind=link}