

Abstract
Background: The importance of safe medication delivery is paramount. Although medication lateness is mentioned in medical literature, there is no standard available for benchmarking. In addition, benchmark data for Respiratory Care (RC) is non-existent. In recent years, the focus has been on information technology systems to avoid medication errors (ME). Safeguards like dose-error-reduction systems, barcode scanners, and independent double checks help to reduce some avoidable ME, but errors still exist when the medications are not delivered timely. According to recent data, a third of all ME causing patient harm, occur in the medication preparation and administration phases.1 We aimed to develop a baseline for medication lateness (ML) in our RC department and develop a plan for continued monitoring and improvement. Methods: IRB approval was obtained, and medication administration data was obtained for 2017 (baseline data) in our pediatric hospital system. All aerosolized medications on inpatient units were included. ML was defined as a medication administered more than 60 minutes after the scheduled time. Data was analyzed and reported to the RC staff for all months of 2018. Throughout the year, education on appropriate re-timing of medications, expected timeliness of delivery, and a trial of certain twice-daily medications on units was performed. Feedback from Respiratory Therapists (RTs) and pharmacy staff were solicited, and an and-on tracker was utilized to document barriers to timely medication delivery at twice-daily department huddles. Results: The baseline ML for 2017 was 4.04%, and the mean for 2018 was 3.34%. Increases in ML were associated with twice-daily administration times and with pentamidine delivery. No correlations between RT staffing, assignments, or medication type were substantiated. Adding twice-daily medications to automated dispensing cabinets for availability directly at the point of care did not improve medication lateness. Conclusions: Timeliness of medication delivery is an essential metric for RC departments to monitor that directly impacts patient safety and satisfaction. By utilizing a model of open communication, awareness, and soliciting feedback, we were able to improve overall ML in our department by over 20%. Further research must be done to establish benchmarks and implications for the field of RC. Reference: Smeulers M et al. Quality indicators for safe medication preparation and administration. PLos One 2015;10(4):e0122695. doi: 10.1371/journal.pone.0122695.

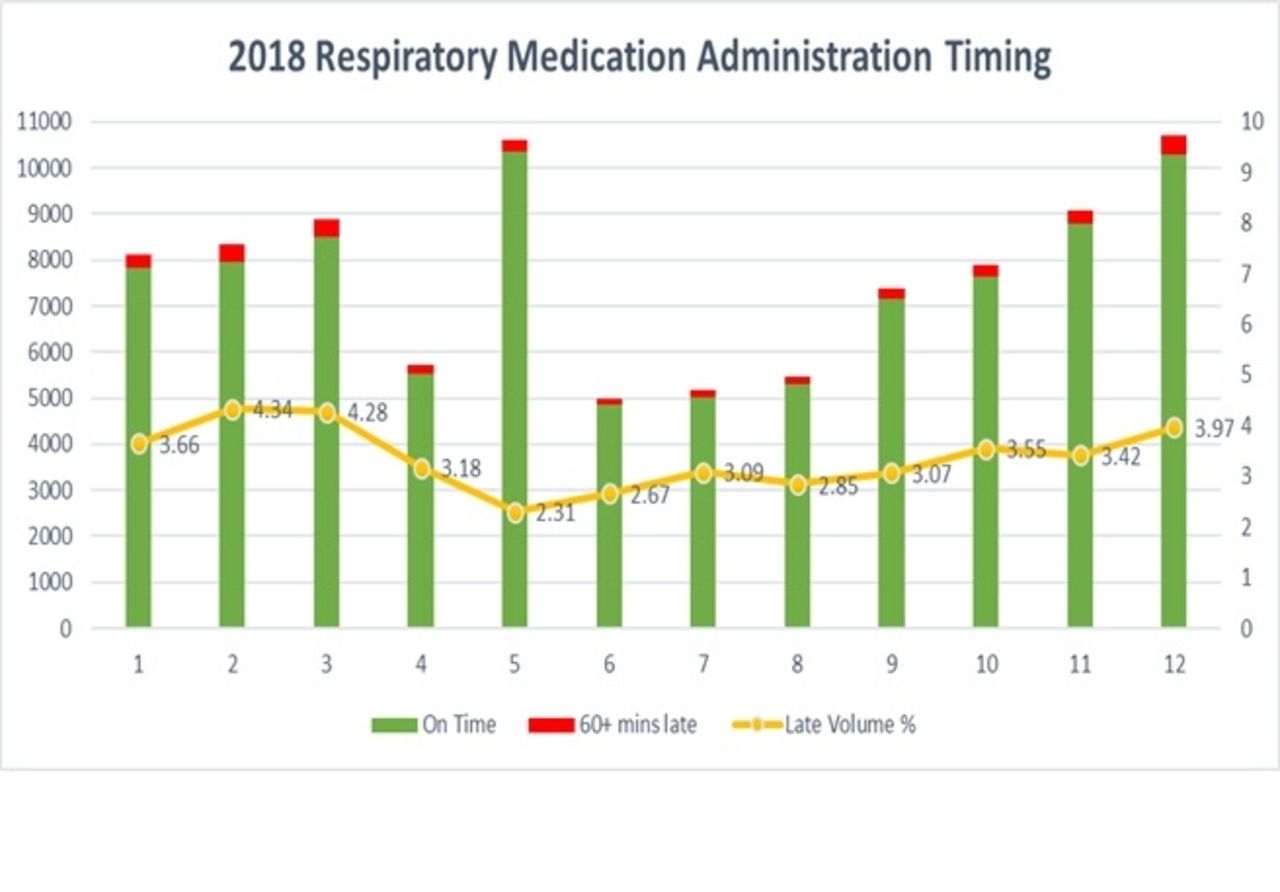
Thsi graph displays the total number of medications given by RTs in 2018 with a breakdown of the timeliness of delivery.
Footnotes
Commercial Relationships: None
- Copyright © 2019 by Daedalus Enterprises




{kind=link}