

Abstract
BACKGROUND: Nebulizer therapy is an important treatment component for patients with cystic fibrosis (CF). Nebulizer manufacturers’ guidelines advocate thorough nebulizer drying after washing. The aim of this study, therefore, was to examine the microbiology associated with nebulizer drying, particularly related to Pseudomonas control, and to examine microbiologically non-adherence to the recommended drying procedures.
METHODS: Four aspects of nebulizer drying were examined in 3 common nebulizers, including examination of the drying profile, improvement to the drying profile of assembled nebulizers, survival of Pseudomonas aeruginosa in tap water and in tap water plus 0.5% (v/v) dishwashing detergent, and the effect of drying of P. aeruginosa in tap water and tap water plus residual sputum (1%v/v, 10%v/v). Microbiologic examination was performed by using P. aeruginosa (5 clinical CF strains plus 1 National Collection of Type Cultures Reference strain).
RESULTS: There were differences in the time to complete dryness between disassembled and fully assembled nebulizers. Vigorous repeated shaking was unable to drive off all residual water on assembled nebulizers. P. aeruginosa counts did not decrease significantly in either tap water or in tap water plus detergent after 24 h storage at ambient temperature. In contrast, all Pseudomonas organisms were killed when nebulizers were dried for 24 h, even when contaminated with 1% and 10% sputum. Dishwashing detergent did not demonstrate any antibacterial activity.
CONCLUSIONS: This study demonstrated that nebulizer drying, if applied properly, had the ability to reduce counts of P. aeruginosa to non-detectable levels. Equally, this study showed that, if the device was not dried thoroughly and moisture remained, then the device was able to support the survival of P. aeruginosa at high numbers, which constituted an infection risk to the patient with CF. This information may help educate and inform the patient with CF about the importance of proper nebulizer drying for Pseudomonas control to improve patient awareness and safety.
Introduction
Cystic fibrosis (CF) is an autosomal recessive disease that affects the ability of the CF transmembrane conductance regulator membrane protein to form functioning ion channels that conduct chloride ions across epithelial cell membranes. The disease manifests itself mainly through the production of purulent and sticky mucus in the lungs that is difficult to clear due to the dysfunction of the mucocillary clearance mechanism. This allows for the entrapment and colonization of several environmental bacterial pathogens, mainly Pseudomonas aeruginosa, in the small airways, which leads to chronic infection and inflammation of the respiratory tract in people with CF. Infection with such bacterial pathogens leads to increased morbidity and mortality, and, therefore, avoidance of infection and treatment plays a major role in the life of patients with CF.1
The delivery of nebulized therapy is an important component of the care in patients with CF, in which this modality is used to effectively deliver, mainly, antibiotics and mucolytic agents.2 Proper maintenance of the nebulizer in terms of ensuring that its performance is maintained optimally as well as ensuring that devices are effectively cleaned and disinfected becomes an important element of nebulized therapies.
A recent cross-sectional, observational, multicenter study conducted in 7 CF centers in Brazil showed that nebulizer contamination was 71.6%, with organism frequency of Candida species. (52.9%), Stenotrophomonas maltophilia (11.9%), non-mucoid P. aeruginosa (4.8%), Staphylococcus aureus (4.8%), and Burkholderia cepacia complex (2.4%).3 This study also showed that the use of tap water in cleaning and outdoor drying of the nebulizer parts significantly increased the chance of contamination of the nebulizer.3
Since 2003, there have been at least 12 seminal infection control guidelines published by learned organizations or bodies, as cited in the 2013 update to the Infection Prevention and Control Guideline for Cystic Fibrosis.4 These updated Cystic Fibrosis Foundation guidelines4 have integrated relevant recommendations from the 2003 Infection Control Guidelines for CF and from other existing infection control guidelines. Readers are particularly guided to sections IV.E.2 and IV.E.3 of the guidelines,4 which relate to CF nebulizer cleaning and disinfection. Issues that relate specifically to device cleaning and infection control in aerosol therapy have also recently been addressed in a seminal review by O’Malley.5
Most health-care institutions instruct patients with CF to follow the washing and disinfection guidelines of their nebulizer as stated by the nebulizer manufacturer. An analysis of such manufacturer guidelines shows that all advocate thorough drying of the nebulizer after washing (Table 1). Although drying has been firmly embedded into nebulizer manufacturer maintenance regimes, there has been a paucity of data that specifically examined drying of nebulizers in terms of the microbiologic effect on contaminating bacteria. It, therefore, was the aim of this study to emulate typical nebulizer drying procedures and to examine the consequences of these on Pseudomonas survival as well as emulating the microbiologic consequences of non-adherence to such guidelines for patient safety.
Comparison of Manufacturer’s Drying Instructions from Common Nebulizer Types Used in Cystic Fibrosis
Quick Look
Current Knowledge
Nebulizer maintenance through washing, disinfection, and drying is critically important in patients with cystic fibrosis (CF) to help reduce infection or re-infection from contaminated nebulizers. Most nebulizer manufacturers instruct washed nebulizers to be thoroughly dried after each use. There are few data available to show how nebulizer microbiology is influenced by nebulizer-drying practice.
What This Paper Contributes to Our Knowledge
This study demonstrated that fully assembled nebulizers dry more slowly than fully disassembled devices. We also showed that Pseudomonas aeruginosa was able to survive at high numbers in residual moisture due to poor and inadequate nebulizer drying, which constitutes an infection risk to the patient with CF. Nebulizer drying, if applied properly, had the ability to reduce counts of P. aeruginosa to non-detectable levels. These data may help educate and inform the patient with CF about the importance of proper nebulizer drying for Pseudomonas control to improve patient awareness and safety.
Methods
Nebulizers Used
Three types of nebulizers were used in the study, namely, Pari LC Plus, Pari e-Flow Rapid (PARI Respiratory Equipment, Midlothian, Virginia), and Philips Respironics Sidestream (Philips Healthcare, Philips Centre, Guildford, United Kingdom). All nebulizers used were new and previously unused.
Bacterial Strains Used
P. aeruginosa (6 strains) were used in this study. These strains were obtained from the Northern Ireland HSC Microbiology Culture Repository housed at the Northern Ireland Public Health Laboratory, Belfast City Hospital. Five P. aeruginosa strains were originally isolated from the sputum of adult patients with CF and one strain was the Reference strain P. aeruginosa National Collection of Type Cultures 12903. All isolates were recovered on Columbia blood agar (CM0031, Oxoid, Basingstoke, United Kingdom), supplemented with 5% (v/v) defibrinated horse blood for 24 h at 37°C under aerobic conditions and passaged a further 3 times, before use.
Nebulizer Drying Experiments
Examination of the Drying Profile.
The drying profile of nebulizers was examined by comparing the nebulizer disassembled into its individual components and the nebulizer fully assembled. Nebulizers were washed and rinsed thoroughly in running tap water before use. For the disassembled configuration, nebulizers were disassembled into their individual components and submerged fully in tap water. Individual components were shaken vigorously 10 times to remove excess water and were placed on a stainless-steel surface and allowed to air dry at room temperature (20°C) with no forced air or air conditioning. Individual components were weighed collectively (to 0.1 g) until a constant weight was achieved, and the mass of residual water (g) and time (min) were recorded throughout.
For the assembled configuration, fully assembled nebulizers were completely submerged in tap water. Assembled nebulizers were shaken vigorously 10 times to remove excess water and were placed on a stainless-steel surface and allowed to air dry at room temperature (20°C) with no forced air or air conditioning. Assembled nebulizers were weighed (to 0.1 g) until a constant weight was achieved, and the mass of residual water (g) and time (min) recorded throughout.
Improvement to the Drying Profile of Assembled Nebulizers.
Fully assembled nebulizers were completely submerged in tap water, which allows for the removal of any trapped air bubbles. The nebulizers were removed and vigorously shaken 10, 20, and 30 times. The mass of residual water was measured (to 0.1 g) after each frequency of shaking. The experiment was repeated by using tap water plus dishwashing detergent (0.0075% [v/v]).
Survival of P. aeruginosa in Tap Water and in Tap Water Plus 0.5% (v/v) Dishwashing Detergent.
P. aeruginosa (5 isolates) were prepared individually by culturing on standard plate count agar (CM0463, Oxoid) for 24 h at 37°C aerobically. After this, inocula were prepared in 0.1% (weight/volume) peptone saline diluent (CM0733, Oxoid) and inoculated in sterile tap water (10 mL) or in sterile tap water plus dishwashing detergent (0.5% [v/v]) (10 mL) to give ∼106–107 colony-forming units/mL. Water-bacterial suspensions were incubated at room temperature (20°C) for 24 h. Bacteria were counted before incubation and after 24 h, and the counts were expressed as colony-forming units/mL water.
Effect of Drying of P. aeruginosa in Tap Water and in Tap Water Plus Residual Sputum (1% v/v, 10% v/v).
P. aeruginosa (5 isolates) were prepared individually by culturing onto standard plate count agar (CM0463, Oxoid) for 24 h at 37°C aerobically. After this, inocula were prepared in 0.1% (weight/volume) peptone saline diluent (CM0733, Oxoid) and inoculated into either sterile tap water (10 mL), sterile tap water plus 10% (v/v) sterile CF sputum (10 mL), or sterile tap water plus 1% (v/v) sterile CF sputum (10 mL). Inocula (100 μL; ∼106 colony-forming units) of each P. aeruginosa, in combination with the tap water plus sputum combinations, as described above, was placed onto a sterile plastic petri dish (Sterilin, Newport, Gwent, United Kingdom) and dried for 24 h under 2 conditions: room temperature (20°C, no forced air) and in an incubator (37°C for 24 h). After this, 10 mL nutrient broth (CM1, Oxoid) was added to each dish and incubated for 24 h at 37°C, then the broths were checked for bacterial growth and were subcultured (10 μL) onto standard plate count agar for a further 24 h at 37°C and rechecked for bacterial growth.
Statistical Analyses
Statistical significance was determined by a 2-tailed paired t test, with P < .05 (5%) considered significant.
Results
The mean mass of residual water that remained during the drying process with the 3 nebulizer types is shown in Figure 1. For the Pari e-Flow Rapid nebulizer, the time difference to complete dryness was 649 min between a disassembled nebulizer and a fully assembled nebulizer. Likewise, with the Philips Sidestream nebulizer, the time difference to complete dryness was 759 min between a disassembled nebulizer and a fully assembled nebulizer.

Comparison of drying for A: Pari e-Flow Rapid, B: Pari LC Plus, and C: Philips Sidestream.
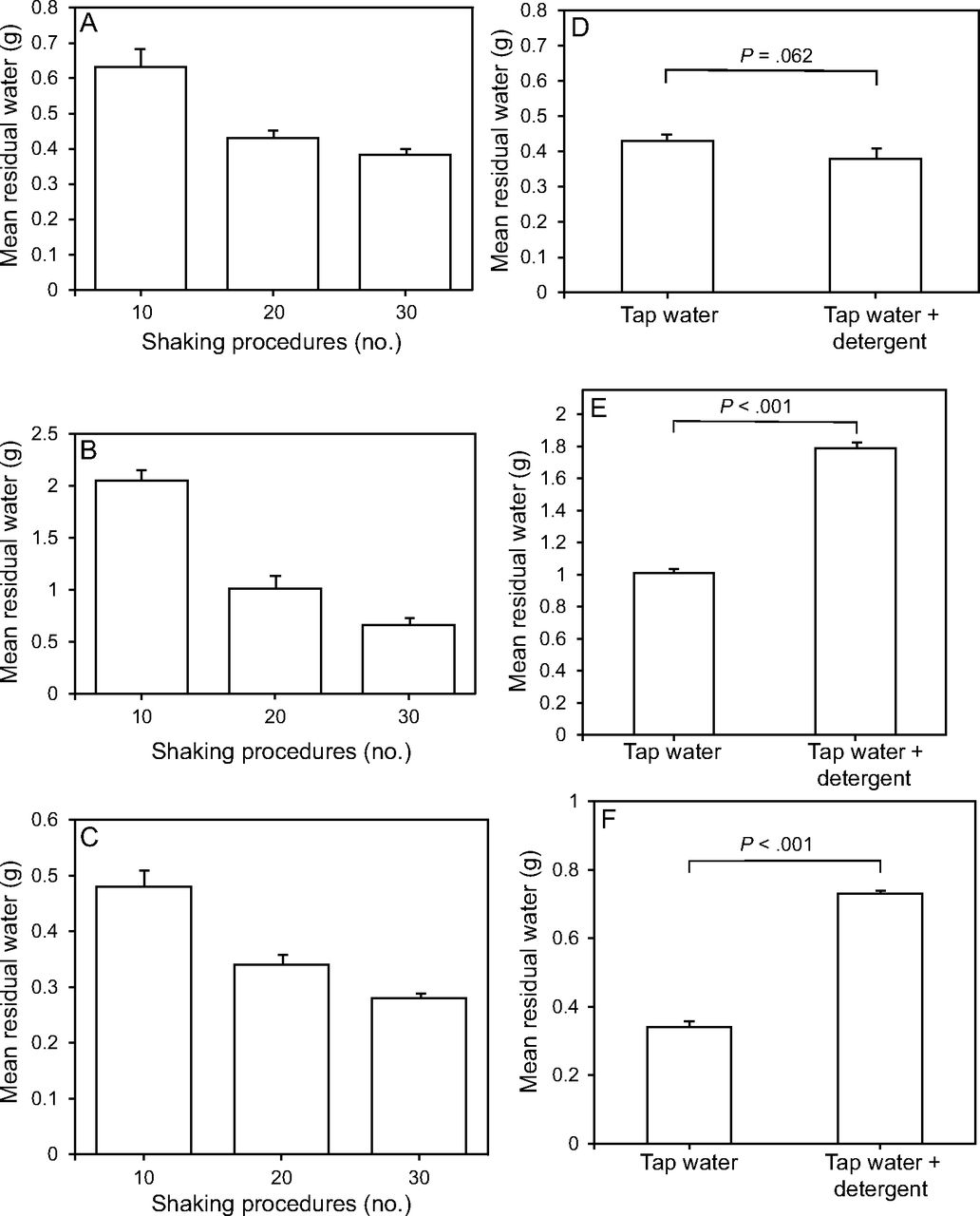
The mean mass of residual water that remained with assisted drying (vigorous shaking) in assembled nebulizers during the drying process with the 3 nebulizer types is shown in Figure 2A. A comparison of the mean mass of residual tap water and tap water plus detergent (0.0075% [v/v]) is shown in Figure 2B. The survival of P. aeruginosa (n = 5 isolates) at room temperature for 24 h is shown for tap water and for tap water plus detergent (0.5% [v/v]) (Fig. 3). The mean bacteriologic counts in tap water and in tap water plus detergent (0.5%) at 24 h are compared in Figure 3C.

The effect of vigorous shaking on drying of assembled nebulizers (A, B, C) and residual detergent (0.0075% [v/v]) on drying (D, E, F). Nebulizers shown are Pari eFlow (A and D), Pari LC Plus (B and E), and Philips Sidestream Plus (C and F).

A: Survival of Pseudomonas aeruginosa with tap water (P = .23), B: tap water plus dishwashing detergent (0.5% [v/v] (P = .45)), and C: comparison of the survival of P. aeruginosa in tap water and in tap water plus dishwashing detergent (0.5% [v/v]) (P = .89).
The survival of P. aeruginosa (5 isolates) on plastic surfaces at room temperature for 24 h is shown for tap water, tap water plus detergent (0.5% [v/v]), tap water plus 10% (v/v) sputum, with assisted drying (in an incubator) and tap water plus 1% (v/v) sputum with assisted drying (in an incubator). The effect of drying on P. aeruginosa (5 isolates) in tap water that contained 1% (v/v) on plastic surfaces at room temperature for 24 h, with no forced or assisted drying is shown in Figure 4.

A: Drying effect on the survival of Pseudomonas aeruginosa in tap water and in tap water plus dishwashing detergent (0.5% [v/v]); B: tap water plus 10% (v/v) sputum and 1% (v/v) sputum dried under assisted conditions at 37°C; and C: tap water plus 1% (v/v) sputum dried under passive conditions at room temperature.
Discussion
Although many of the infection prevention and control guidelines advocate thorough drying of nebulizers, there are few existing data to substantiate this guideline4 in terms of the effect of drying on the microbiology of bacteria on nebulizers. The first aspect that we examined in this study was to compare the efficiency of unassisted (passive) nebulizer drying with fully disassembled nebulizers versus fully assembled nebulizers. A difference between such drying times in the same nebulizer type, depending on whether the device was disassembled, is demonstrated in Figure 1. Fully assembled nebulizers that had been thoroughly rinsed with tap water required extremely long drying times, of ∼800 min for the Pari e-Flow Rapid and Philips Sidestream plus nebulizers, whereas the Pari LC Plus nebulizer still contained residual moisture at 800 min.
The reason for these extended drying times was the capture and holding of residual water mainly in the drug chamber, during the rinse process, which was unable to escape quickly via drying due to the enclosed convoluted nature of the device, which aided water retention. In contrast, the opening up of such devices during a disassembled drying process allowed for the release of significantly large areas of the device to drying, thereby significantly decreasing drying times. Thus, the added value of disassembling the device into its respective components before washing and drying is seen in shorter drying times, of ∼82 min (∼1.5 h) versus at least 11–13 h for the fully assembled nebulizer.
Second, given the extended drying times for the fully assembled nebulizers, we attempted to speed up the drying times of the 3 nebulizer types by including a vigorous shaking procedure in an attempt to drive off residual moisture (Fig. 2). Here, we compared vigorous shaking with 10, 20, and 30 consecutive shakes. Although such shaking was able to reduce residual water that remained by approximately half, this procedure was unable to drive off all the remaining water, for the nebulizer to be safely stored or used because it was not completely dry. Therefore, from our data, the nebulizers should be completely disassembled before washing, rinsing, and drying. Nebulizers should not be washed, rinsed, and dried in an assembled state.
Third, we wanted to examine the effect of not thoroughly rinsing all residual detergent from the nebulizer from the washing and rinsing stage before device drying by including dishwashing detergent in tap water at a concentration of 0.0075 (v/v) and to assess the consequence of this on retention of residual water in and/or on fully assembled nebulizers (Fig. 2). Overall, with the 3 nebulizer devices, water retention increased by 60.1% when detergent was not completely rinsed off due to the reduction in surface tension by the surfactant in the detergent, which thereby increased the wetting properties of the water-detergent mixture on the nebulizer. The consequence of inadequate rinsing with water would lead to increased water retention and, therefore, increased drying times. Therefore, from our data, before drying, nebulizers should be rinsed thoroughly to remove all residual detergent.
Fourth, we wanted to examine the survival of P. aeruginosa in water and in water that contained residual detergent (0.5% [v/v]) over a 24-h period, emulating what would happen to P. aeruginosa in moisture droplets that remain on an inadequately dried nebulizer (Fig. 3). For water, mean P. aeruginosa counts decreased by 0.58 log units, and, with water–residual detergent mixtures, the mean P. aeruginosa counts decreased by 0.65 log units; neither of these reductions in P. aeruginosa counts were statistically significant (P > .05). There was no antibacterial activity with the dishwashing detergent. Clinically, this translates that inadequately dried nebulizers will harbor approximately the same bacterial load 24h after rinsing, as at time of initial rinsing.
Fifth, we wanted to examine the effect of thorough drying of nebulizers on P. aeruginosa survival, when retained moisture contained water, water that contained detergent (0.5% [v/v]), water that contained 1% (v/v) sputum, and water that contained 10% (v/v) sputum. In addition, we wanted to compare forced drying at 37°C, by using an incubator, with passive drying in ambient conditions (Fig. 4). In all of these scenarios, we were unable to recover any culturable P. aeruginosa organisms after incubation for 24 h. Sputum was added to emulate carryover from poorly washed and rinsed devices because the sputum may act as a protector against the P. aeruginosa drying out and being killed on the plastic surface of the nebulizer. According to our data, nebulizers should be thoroughly dried before being used. This is a critical control for Pseudomonas control.
It is important to note that the time to full drying may vary based on several parameters, including configuration of the nebulizer (assembled or disassembled), surrounding air temperature, the presence of residual detergent, relative humidity of the immediate drying environment, and if the drying process is active (ie, using forced air circulation) or passive. Given these variables, the nebulizer drying process can become subjective with patients because it can be difficult to judge whether the nebulizer has dried absolutely or if moisture still remains in the device.
From the discussion above, we note that any remaining moisture will support the survival of P. aeruginosa organisms without any significant reduction in bacterial numbers. Therefore, it is important for the patients to risk assess and risk manage their specific circumstances that relate to how they personally maintain their nebulizer device to finally use a fully dried device with minimum risk of P. aeruginosa contamination. Given the subjective nature of assessing what is thoroughly dried and what is not, patients with CF may want to use a second replicate nebulizer device, which they dry and store in a dry environment for 24 h before use and thus alternate using 2 nebulizers on a consecutive “day-on, day-off” basis, in an attempt to maximize optimum drying of their devices.
A recent survey achieved a consensus on 10 research priorities in CF, in which simplifying the treatment burden of people with CF ranked as the top priority.6 Coupled with this, a previous patient survey showed that some subjects did not clean their nebulizer as often or as well as recommended by manufacturers’ guidelines, primarily because they were busy doing other tasks during their day.7 Consequently, nebulizer drying may be compromised due to the time required for nebulizer care and hygiene, which results in potential survival of P. aeruginosa, which was acquired from tap water, the washing-drying environment, and/or the patient’s sputum.
In our studies, the killing of P. aeruginosa was achieved through desiccation. The biology of the organism plays a crucial role as to how susceptible the bacteria are to drying. Certain organisms, especially the spore-forming bacteria from the genera Bacillus and Clostridium can tolerate extremes of desiccation due to the physiologic resilience of their spores. However, vegetative cells are more susceptible to varying degrees of drying, in which bacterial cell death results from several drying-related processes, including the following: shrinkage of capsular layers, an increase in intracellular solute levels, crowding of macromolecules, changes in the volume of cell compartments, changes in the biophysical properties (eg, surface tension), reduced fluidity (increased viscosity), damage to external layers (eg, pili, membranes), and changes in physiologic processes (eg, growth arrest).8
The manipulation of these lethal events with bacteria through drying can lead to cell death, and it is important that we have the evidence to allow exploitation of these physiologic weakness through effective infection prevention interventions, to achieve the desired outcome of cell death. In the case of P. aeruginosa, the organism can respond to desiccation stresses through the production of biofilm and extracellular polysaccharide in an attempt to hydrate the immediate environment and so sustain survival. For this reason, we designed several experiments in the present study to address protection to P. aeruginosa from drying offered by this survival strategy.
Analysis of our data showed that, in the absence of any protection, P. aeruginosa cells were non-culturable within 24 h. We then wanted to examine what protection (if any) was offered by P. aeruginosa biofilm and sputum during the drying process. Here, we attempted to emulate a poor nebulizer washing procedure with incorporation of 1% (v/v) and 10% (v/v) sputum, to mimic residual carryover of sputum. Even in the presence of such contamination, we were unable to culture any P. aeruginosa after 24 h of drying in both assisted drying and passive (air) drying.
Overall, in this study, we attempted to emulate potential scenarios that related to nebulizer drying that the patient may encounter when maintaining his or her nebulizer device. Although this study was performed with clinical strains of the Gram-negative organism, P. aeruginosa, it was not possible to extrapolate the findings of the current study to other organisms, including Gram-positive organisms (S. aureus) or the non-tuberculous mycobacteria, (eg, Mycobacterium abscessus). Given that these non-Pseudomonas organisms have a different biology than the Gram-negative organisms in terms of their architectural and biochemical structure of their cell membranes and cell walls, it would be unwise to use these data generated for P. aeruginosa and to cross-apply these data to other bacterial species and genera. Therefore, this study needs to be repeated for each of these other organisms separately and the data from such experiments used to determine the drying dynamics specific for each different bacterial species.
Conclusions
Results of this study demonstrated that drying of the nebulizer, if applied properly, had the ability to reduce counts of P. aeruginosa to non-detectable levels and, therefore, to minimize the risk to the patient of acquiring P. aeruginosa from the nebulizer device. Equally, this study showed that, if the device is not dried thoroughly and moisture remains, then the device is able to support the survival of P. aeruginosa at high numbers, which constitutes an infection risk to the patient with CF. The information contained within this study may help educate and inform the patient with CF about the importance of proper nebulizer drying for Pseudomonas control to improve patient awareness and safety.
Footnotes
- Correspondence: John E Moore PhD, Northern Ireland Public Health Laboratory, Department of Bacteriology, Belfast City Hospital, Lisburn Rd, Belfast BT9 7AD, Northern Ireland, UK. E-mail: jemoore{at}niphl.dnet.co.uk
This study was supported by the Northern Ireland Working Group on Nebuliser Care & Hygiene in Cystic Fibrosis, which has received educational grants from Vertex Pharmaceuticals and Chiesi (UK).
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}